

case report
An Unknown Complication of a Rare Combination of Intestinal Invagination and Meckel’s Diverticulum Invaginated in An Adult: A Case Report
- Salvatore Ragazzi *
- Alessandro Buttafuoco
- Salvatore Dipietro
Department of General Surgery, Guzzardi’s Hospital Vittoria, Italy.
*Corresponding Author: Salvatore Ragazzi,Department of General Surgery, Guzzardi’s Hospital Vittoria, Italy.
Citation: Ragazzi S, Buttafuoco A, Dipietro S. (2023). An Unknown Complication of a Rare Combination of Intestinal Invagination and Meckel’s Diverticulum Invaginated in An Adult: A Case Report. Journal of Surgical Case Reports and Reviews. BRS Publishers. 2(1); DOI: 10.59657/2993-1126.brs.23.008
Copyright: © 2023 Salvatore Ragazzi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 28, 2023 | Accepted: May 10, 2023 | Published: May 30, 2023
Abstract
Introduction: Intestinal invagination is a common pathology amongst children, while it is a rare entity in adults. Invagination is responsible for only 1-3% of adult-onset intestinal obstruction. Meckel’s diverticulum, on the other hand, is the most common congenital anomaly of the gastrointestinal tract. Most of them are asymptomatic; they are recognized when they complicate, and can present with diverticulitis, gastrointestinal bleeding, intestinal obstruction, perforation, or invagination. Invagination with the Meckel’s diverticulum (MD) is a rare cause of chronic abdominal pain in the adults. We wish to present this first case of intestinal invagination and Meckel ‘s diverticulum invaginated.
Presentation of case: We report the case of a 17-year-old man who was admitted to the emergency room due to a diffuse abdominal pain. Abdominal CT scan showed intestinal invagination and intestinal obstruction. The exploratory laparoscopy revealed the presence of intestinal invagination and segmental resection of the small intestine was performed. The patient was discharged on the sixteen post-operative day.
Discussion: The prevalence of MD is 1 to 4%. Diagnosis is often difficult and delayed because clinical symptoms are not specific and the diagnosis is performed mainly by imaging studies. Intestinal obstruction is a more common complication in adults, whereas in children, bleeding is the more common complication. In our case, the patient had a diffuse abdominal pain with small bowel obstruction. Laparoscopy may be useful for confirming the presence of intestinal invagination, and demonstrating the underlying organic lesion serving as the lead point. Only with the laparotomy we have been able to notice the combination of intestinal invagination and MD invaginated.
Conclusion: we aimed to present the role of Meckel’s diverticulum as an initiating factor of illegible invagination, with inversion into the ileum and specifically in our clinical case can cause invagination of itself.
Keywords: intestinal invagination; meckel’s diverticulum invaginated; 17-year-old man; abdominal pain; clinical symptoms; laparotomy
Introduction
Invagination is defined as two consecutive segments of the gastrointestinal tract intertwining into each other [1]. In children, it is the second most common cause of acute abdominal pain after acute appendicitis, while it is rare in adults. It accounts for 0.02-0.003% of all hospital admissions and for 1-3% of intestinal obstructions that require surgery [1,2]. Meckel’s diverticulum is the most common congenital malformation of the gastrointestinal tract (present in 2%–4% of population) due to persistence of the congenital vitello-intestinal duct. Invagination remains a rare condition in adults, representing 1% –3% of bowel obstructions and it is a different entity in adults than in children. It is the most common congenital anomaly of the gastrointestinal system, with a rate of 1-3%. It was first described by Fabricus Hildamus in 1598, and was defined embryologically by the German anatomist Johann Friedrich Meckel in 1809 [3]. Most of them are asymptomatic; they are recognized when they complicate, and can present with diverticulitis, gastrointestinal bleeding, intestinal obstruction, perforation, or invagination. It is a true diverticulum, typically located on anti-mesenteric border, and contains all three coats of intestinal wall with its separate blood supply from the vitelline artery. This case demonstrates the utility of laparoscopy in diagnosing an intussusception of the Meckel’s diverticulum. We wish to present this extremely rare case of intestinal invagination and Meckel ‘s diverticulum invaginated, which is the first one that we have encountered in our practise, along with the accompanying diagnostic and therapeutic issues and a review of the literature.
Presentation Of Case
We report the case of a 23-year-old man who was admitted to the emergency room due to a diffuse abdominal pain. He had crampy abdominal pain with food vomiting, without fever. Abdominal distension, pain in mesogastrium, right lower quadrant tenderness and rebound were present on the examination. There was no gas or faces discharge in the last 24 hours. In the anamnesis he reported surgery for hypertrophic pyloric stenosis at the age of two months. There was gas-liquid level on the direct abdominal radiography with ileal distension. Laboratory findings showed: white blood cell count 17100 mm3, haemoglobin 13.7 g/dl, haematocrit 42.8%, and C-reactive protein (CRP) < 2>
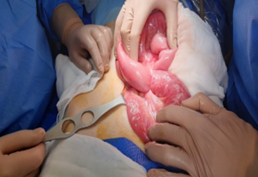
Photo 1

Photo 2
therefore, the invaginated segment was resected and side-to-side ileoileal anastomosis was performed. At the opening of the operating piece, we noticed the rarity of the clinical case: intestinal invagination and Meckel ‘s diverticulum invaginated. Microscopic examination disclosed an ectopic gastric mucosa with ischemic changes on the whole ileum examined and confirmed the macroscopic appereance of intestinal invagination and Meckel ‘s diverticulum invaginated (Photo 3-5). The patient tolerated the procedure and the postoperative period was complicated from a partial iatrogenic thrombosis of the left humeral vein confirmed by upper limb ultrasound. The patient was discharged on the sixteen post-operative day.

Photo 3

Photo 4
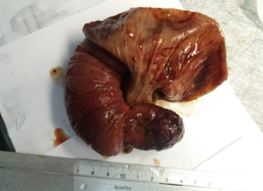
Photo 5
Discussion
This case report presents the unusual case of intestinal invagination and Meckel ‘s diverticulum invaginated. By reviewing the literature, we aim to identify the management of this variant.
Intestinal invagination is a common pathology amongst children, while it is a rare entity in adults.Ninety-five percent of invaginations occur in childhood. Invagination is responsible for 1-2% of adult-onset intestinal obstruction [2]. The invagination shows itself frequently with complete obstruction findings, as acute abdominal pain, nausea and vomiting, as it may present with subacute and chronic findings, as a result of partial obstruction. In 24-42% of the studies, it was observed that it can produce symptoms of an abdominal mass [13]. Our case had abdominal pain of acute onset, with subsequent distension and nausea and vomiting. Ultrasonography (USG) is accepted as the most valuable non-invasive diagnostic tool in patients who are thought to have invagination. The findings of invagination on USG are as follows: soft tissue mass with 2.5-5 cm diameter, target sign, multiple concentric ring sign, “pseudo kidney” sign, and the sandwich sign. The sensitivity, specificity and negative predictive value of USG for the diagnosis of invagination are 98-100%, 88% and 100%, respectively [14]. Although the gold standard for invaginations is CT, it provides 50- 80% diagnostic data (2). In our case, abdominal USG was performed for atypical abdominal pain, and the invagination image was seen. As the invagination was diagnosed with suspected clinic of progressing obstruction, imaging studies including abdominal USG and CT scan were performed under emergency conditions and revealed ‘target lesions’ suggestive of small bowel intussusception and free-fluid in the abdominal cavity. Intestinal invagination is a common pathology amongst children, while it is a rare entity in adults. Invaginations are classified as gastroduodenal, enteric, ileocecal, and colonic, according to their localizations [13,15].
MD is an intestinal diverticulum that results from incomplete obliteration of the most proximal portion of the vitelline or omphalos-mesenteric duct during the fifth week of fatal development [4]. The failure of closure of the duct can result in an umbilical fecal fistula, umbilical sinus, fibrous cord, enterocystoma, mesodiverticular band or MD (distal ductal closure) [5]. MD contains all the three intestinal layers. It contains heterotopic tissue in 50
Conclusion
The complications related with MD should be kept in mind in the pre-diagnosis in young patients presenting with acute abdomen and ileus. A good knowledge of the clinical findings of MD would facilitate the decision to operate and the timing of the surgery, thereby preventing problems such as misdiagnosis and increase in morbidity in patients with a pre-diagnosis of acute abdomen. Although intestinal invagination and Meckel ‘s diverticulum invaginated is extremely rare, general surgeons should be aware of the possibility of this presentation.
References
-
-->













