

Case Report
An Incarcerated Inguinal Sigmoid Hernia Case Report with Large Bowel Obstruction
Department of surgery, Hawassa University college of Medicine and Health Science, Ethiopia.
*Corresponding Author: Tigabu Daniel, Department of surgery, Hawassa University college of Medicine and Health Science, Ethiopia.
Citation: Daniel T. (2024). An Incarcerated Inguinal Sigmoid Hernia Case Report with Large Bowel Obstruction, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 1(4):1-3. DOI: 10.59657/2997-6103.brs.24.020
Copyright: © 2024 Tigabu Daniel, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 05, 2024 | Accepted: July 26, 2024 | Published: August 05, 2024
Abstract
Background: Inguinal hernia is a term used to describe a protrusion of the peritoneum in the inguinal region, either with or without other contents. It's rare to find a sigmoid inguinal hernia.
Case Report: A 75-year-old patient presented with symptoms and signs consistent with large bowel obstruction. For four years, he also had a reducible swelling in his right inguinal and epigastric regions, but after four days, it stopped being reducible. Due to a prior trans vesical prostatectomy, a large bowel post-operative adhesion was taken into consideration. The patient's x-ray revealed complete large bowel obstruction. An incarcerated sigmoid colon right inguinal hernia and omental epigastric hernia were found after entering the abdomen through a vertical mid-abdominal incision. The viable sigmoid colon and momentum from each hernia were then reduced, respectively. After completing a modified Bassini procedure using separate inguinal incisions for an inguinal hernia and direct repair for an epigastric hernia, the patient was discharged after 48 hours. The epigastric hernia repair was done because it was on the vertical abdominal incision site.
Conclusion: Large bowel inguinal hernias are not common, but it's crucial to consider large bowel obstruction when there are suggestive x-ray features, like our patient.
Keywords: incarceration; hernia; obstruction
Introduction
A protrusion of the peritoneum, with or without additional contents, is called an inguinal hernia. There are two types of inguinal hernias: direct and indirect [1-3]. Of abdominal wall hernias, two thirds are inguinal hernias [4]. Small intestine and momentum are frequent inguinal hernia contents, whereas the large bowel is infrequently [1,2,5-7]. When sigmoid inguinal hernias occur, they usually occur on the left side; right side sigmoid inguinal hernias are uncommon [3]. There are various open and laparoscopic methods for treating inguinal hernias, but the most effective method will depend on the surgeon's experience [8].
Case Report
A 75-year-old male patient arrived complaining of four days of inability to pass stool and flatus. He also experiences cramping in his abdomen and distension. Additionally, he has had two incidents of vomiting of ingested matter. The patient has a four-year history of right inguinal and epigastric reducible, painless swelling. TVP was performed for BOO related to BPH around 4 years ago, and the condition improved. He takes nifedipine for hypertension; he does not have any chronic illnesses. Vital indicators during physical examination: temperature of 36.70C, respiration rate of 23, blood pressure of 120/70, and pulse rate of 84. An examination of the abdomen revealed a distended Hyper thympanethic, irreducible, non-tender epigastric mass and a right inguinal mass, however neither mass had any audible bowel sounds. Upon digital rectal examination, the rectum was empty. Additional system analysis yields no new insights. The erect abdomen x-ray (Figure 3 erect plane abdominal x-ray) revealed complete large intestinal obstruction; however, the CBC was non-revealing. He was ready for exploration once the patient had been optimized, taking into account post-operative adhesion to R/O incarcerated inguinal and epigastric hernia. The intraoperative observations revealed minor ascites, an incarcerated epigastric hernia omentum, and incarcerated right inguinal hernia sigmoid colon (Figure 1 and 2). The proximal colon was greatly dilated and edematous, but the sigmoid and omentum were both viable and had shrunk back. Ultimately, a rectal tube was placed and kept in place. Modified Bassini repair was done for inguinal hernia via separate inguinal incision after reducing the content and epigastric hernia closed through the same incision on mid abdomen. After the procedure went well and abdomen closed in layers, the patient was sent to the post-anesthesia care unit. The patient was appointed and discharged from the ward after four uneventful days.

Figure 1: Before Reduction of Incarcerated Sigmoid Colon Right Inguinal Hernia.
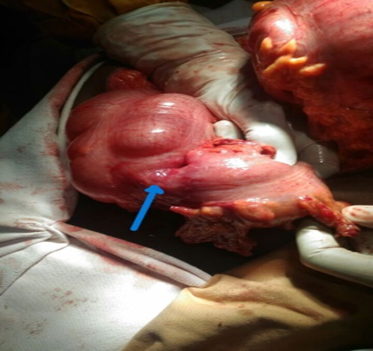
Figure 2: After Reduction of Right Incarcerated Sigmoid Colon Inguinal Hernia.

Figure 3: Erect Plane Abdominal X-Ray.
Discussion
Of abdominal wall hernias, inguinal hernias account for two thirds [4]. Common contents are momentum and small intestine but rarely the large bowel [1,2,5-7]. A surgeon's familiarity with a particular technique will determine the optimal approach for treating an inguinal hernia, as there are several open and laparoscopic methods [8]. When sigmoid inguinal hernias occur, they usually occur on the left side; right sigmoid hernias are uncommon [9]. Similar to Anteneh et al.'s study, our patient is older, yet he still has a right sigmoid inguinal hernia [10]. Due to the lack of preoperative regular CT and contrast scan, it is challenging to diagnose incarcerated large bowel in inguinal hernia in our setup. The patient's prior pelvic surgery, which was recognized as a risk factor for post-operative adhesion, presented another challenge. A major congenital abdominal wall defect was shown in a large bowel inguinal hernia case report by Dinesh et al.; this is not usually the case with our patient report [2]. The transverse colon, cecum, and appendix may all be accommodated by this substantial concurrent congenital abdominal wall deficiency. Except for the well-known BOO that has already had treatment; our case does not have any congenital wall defects. Nothing about our case report has been reported from our nation or area. In general, patients who have an inguinal hernia and exhibit signs of significant intestinal obstruction should have sigmoid inguinal hernia taken into consideration.
Conclusion
Large bowel inguinal hernias are uncommon, but it is important to consider large bowel obstruction in the presence of suggestive x-ray features like our patient.
Abbreviations
BOO- Bladder Out Let Obstruction
BPH- Benign Prostatic Hyperplasia
CBC- Complete Blood Count
TVP- Transvesical Prostatectomy
Declarations
Ethical Clearance
Since it is case report IRB clearance is not needed but consent for publication was obtained from patient and can be availed if needed.
Consent for Publication
Written informed consent for publication was obtained from the patient. I will avail the consent at a time needed.
Availability of Data and Materials
The data in this case report will be accessed by the contact address of the corresponding Author.
Conflict of Interests
No financial or non-financial competing interests
Funding
There is no financial support.
Acknowledgements
My deepest gratitude goes to the patient, family and my fellow general surgery residents.
References
- Sanjay R, Khan F, Gupta S P A. (2021). Case Report of a Giant Inguinal Hernia Causing Intestinal Obstruction. Int Surg J. 8(8):2463.
Publisher | Google Scholor - Koirala DP, Joshi SP, Timilsina S, Shress V, Gc S, et al. (2022). Large Intestine as Content of Congenital Inguinal Hernia: A Case Report of Intestinal Obstruction. Ann Med Surg. 75:103396.
Publisher | Google Scholor - Mahajan A, Luther A. (2014). Incarcerated Right Inguinal Hernia Containing Sigmoid Colon: A Rare Case Report. Chrismed J Heal Res. 1(4):281.
Publisher | Google Scholor - Ndong A, Tendeng JN, Diallo AC, Diao ML, Sow O, et al. (2023). Adult Groin Hernia Surgery in Sub-Saharan Africa: A 20-Year Systematic Review and Meta-Analysis. Hernia. 27(1):157-172.
Publisher | Google Scholor - Editor. (2014). American Journal. Am J Econ Sociol. 73(4):627-988.
Publisher | Google Scholor - Sunday O, Africa EC, Africa C. (2015). A Case Report of a Massive Strangulated Left Indirect Inguinal a Case Report of a Massive Strangulated Left Indirect Inguinal Hernia Containing Small. Anatomy Journal of Africa. 4(2):546-550.
Publisher | Google Scholor - Karthikeyan VS, Sistla SC, Ram D, Ali SM, Rajkumar N. (2014). Giant Inguinoscrotal Hernia-Report of A Rare Case with Literature Review. Int Surg. 99(4):560-564.
Publisher | Google Scholor - Liu SH, Yen CH, Tseng HP, Hu JM, Chang CH, et al. (2023). Repair Of a Giant Inguinoscrotal Hernia with Herniation of The Ileum and Sigmoid Colon: A Case Report. World J Clin Cases. 11(2):401-407.
Publisher | Google Scholor - Salemans PB, Vles GF, Fransen SAF, Smeenk RM. (2013). Sigmoid Carcinoma in An Inguinal Hernia: A Blessing in Disguise? Case Rep Surg. 1-3.
Publisher | Google Scholor - Kibret AA, Tekle SY, Hmariam MM, Worede AG, Dessie MA. (2022). Prevalence And Associated Factors of External Hernia Among Adult Patients Visiting the Surgical Outpatient Department at The University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: A Cross-Sectional Study. BMJ Open. 12(4):1-6.
Publisher | Google Scholor











