

Case Report
All Those Liver Masses Are Not Necessarily from The Liver: A Rare Case of Giant Renal Cyst Mimicking Hepatic Lesion in A CLD Patient
- Khurram Khaliq Bhinder *
- Aroosa Kanwal
- Aroosa Kanwal
- Amna Mehboob
- Nasir Khan
Radiology Department, Shifa International Hospital, Islamabad, Pakistan.
*Corresponding Author: Khurram Khaliq Bhinder, Radiology Department, Shifa International Hospital, Islamabad, Pakistan.
Citation: Khurram K. Bhinder, Kanwal A, Naveed A, Mehboob A, Khan N. (2024). All Those Liver Masses Are Not Necessarily from The Liver: A Rare Case of Giant Renal Cyst Mimicking Hepatic Lesion in a CLD Patient. International Clinical Case Reports and Reviews, BioRes Scientia Publishers. 2(1):1-4. DOI: 10.59657/2993-0855.brs.24.009
Copyright: © 2024 Khurram Khaliq Bhinder, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 01, 2024 | Accepted: May 16, 2024 | Published: May 20, 2024
Abstract
Massive renal cysts are rarely reported. Smaller cysts are usually asymptomatic however larger cyst may become symptomatic by causing mass effect on surrounding structures. In our case known Hep B patient with diffuse abdominal pain. Ultrasound was performed that showed cirrhotic liver morphology with undulating hepatic margins and incidental finding of large right interpolar region cyst that mimicked as hepatic lesion. Incidental finding of cyst of the renal origin mimicking as a hepatic lesion in a CLD patient is rarely reported till date.
Keywords: chronic liver disease; renal cyst; hepatitis; cirrhosis
Introduction
Renal cysts represent a prevalent benign lesion in the kidney, with an incidence exceeding 50% in individuals over 50 years old, and approximately two-thirds of the population exhibiting detectable cysts on CT scan by the age of 80 years [1]. They are acquired abnormalities found in the kidney, frequently located in the renal cortex. Although their exact cause is not fully understood, they are thought to originate from the diverticulum of the distal convoluted tubule [2]. Majority of cysts are smaller than 2 cm in size [3]. Smaller cyst is asymptomatic and typically do not necessitate treatment, often being discovered incidentally during ultrasound examinations. However, symptoms may manifest if these cysts reach a significant size. The cysts larger than 15 cm are rarely reported in literature. Misdiagnosis of large renal cyst is common. Cases have been documented in the literature where renal cysts were mistakenly identified as ascites, gallbladder issues, obesity, mesenteric cysts, and pancreatic pseudocyst [4].
Treatment options for renal cysts include open surgery, percutaneous marsupialization, percutaneous aspiration, and, more recently, laparoscopic surgery. It is highly uncommon for large renal cysts to coexist with chronic liver disease and there is no recorded instance in the literature of a renal cyst being misinterpreted as a hepatic lesion in patients suffering from chronic liver disease. So, we report a case of 61-year-old woman with chronic liver disease related to hepatitis B, who had an incidental discovery of a large renal cyst erroneously diagnosed as a hepatic lesion.
Case Presentation
We report a rare case of 61 years old woman who presented to our outpatient department with diffuse abdominal pain. Pain was mild, intermittent and localized to right upper quadrant. There were no associated vomiting, nausea or fever episodes. Her previous medical history was only positive for hepatitis B. She denied taking any medications for that. On clinical examination the patient's temperature was 39.6°C, blood pressure was 118/82 mm Hg, and heart rate was 85 beats per minute. No pertinent laboratory data was available. She was referred to radiological department for abdominal ultrasound. Mildly undulating hepatic margins were seen with caudate and left lobe lateral segment hypertrophy along with mild splenomegaly and upper abdominal collaterals. Incidental finding of a large well-defined, lobulated, anechoic area was seen arising from the interpolar region of the right kidney measuring up to 11.4 x 9.5 x 12.2 cm (AP X TRV X CC) (volume of 700 mL). The aforementioned cystic lesion had internal calcification showing posterior acoustic shadowing and measuring up to 2.2 mm. Few internal septations were noted. No definite internal vascularity was seen on Doppler images. This mass was closely abutting the left lobe of liver with inseparable fat planes. Patient loss to follow up when referred to surgery for evaluation.
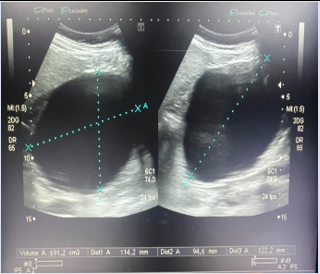
Figure 1: Grey Scale ultrasound image showing volume (691 ml) of right renal cyst.

Figure 2: Grey Scale ultrasound image showing right renal cyst arising from interpolar region.
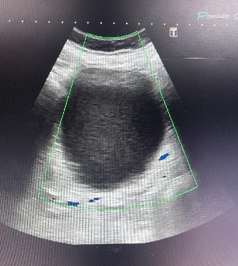
Figure 3: Color Doppler ultrasound image showing no internal vascularity in right renal cyst.
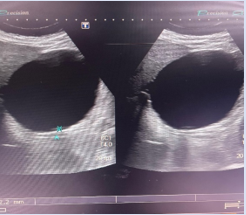
Figure 4:Grey Scale ultrasound image showing internal calcification in right renal cyst.
Discussion
Renal cysts are among the most prevalent benign kidney lesions, occurring more frequently than 50% of the population. Sometimes they are large enough for the patient to feel during a standard clinical examination. The etiology of these is mostly unknown. Renal cysts are kidney-acquired lesions [5, 6]. They are frequent in the renal cortex, and while the cause is unknown, it is thought to stem from the diverticulum of the distal convoluted tubule. The majority of benign kidney cysts are asymptomatic and do not require treatment; they are frequently discovered during routine ultrasonography examinations. When they are large enough, they can produce a wide range of clinical symptoms. It is widely thought to be a harmless abnormality. However, reports of massive renal cysts are extremely unusual [4]. Renal cysts are one of the most frequent benign kidney lesions, appearing at a frequency more than 50% over the age of 50, and up to two-thirds of the population has a cyst identifiable on a CT scan by the age of 80. They are occasionally large enough to be felt during a typical clinical examination or by the patient himself. The majority of cysts are less than 2 cm in size. Kidney cysts are typically oval or circular in form, bordered by a single layer of flattened epithelium, and filled with clear or straw-colored fluid [7].
It is highly uncommon for giant renal cysts to coexist with chronic liver disease (CLD), and reports of these cases are rare. Cases presenting simply with progressive abdominal distension can lead to a misdiagnosis as we have reported in our case. An examination that is useful is ultrasound. Its noninvasiveness, accessibility, and lack of radiation are highly valued.
The causes of these cysts are unclear. Neonatal renal cysts have been associated with posterior urethral valves [8], but valves have not been linked to cysts in older children. This blockage is most likely etiological, with the cysts developing from calyceal diverticula in utero. The pathophysiology of cysts that appear at a later stage is less known. If developmental, they might be anomalies from previous generations of uriniferous tubules that remain as cystic collections. If acquired, they may indicate renal tubular obstruction caused by localized ischaemia and inflammation, which have been shown in experiments to create epithelial cysts. Giant renal cysts were misinterpreted for palpable gallbladders, as well as fat. Renal cysts can be treated by percutaneous aspiration with or without sclerosant injection, percutaneous marsupialization, open surgery, and, most recently, laparoscopic surgery via transperitoneal or retroperitoneal access [9]. This form of large cyst has seldom been documented in the medical literature, however Brown et al. [10] did describe a huge renal cyst measuring 25 cm in diameter and presenting with significant abdominal distension. To the best of our knowledge, our case is the largest renal cyst reported in the medical literature, in a CLD patient mimicking as a liver lesion.
Conclusions
Incidental finding of cyst of the renal origin mimicking as a hepatic lesion in a CLD patient is seldom reported till date. Determining the origin of cyst preoperatively can sometimes be challenging and needs accurate diagnosis. It is important to be aware that in a small percentage of situations, outcomes may be deceptive for practitioners.
Declarations
Conflict of Interest
All authors declare no conflict of interest.
Funding Role
None to declare.
Author Contributions
All authors contributed equally to the drafting of study.
Ethical Statement
The patient signed an informed consent form, as per the ethical guidelines of hospital board.
References
- Laucks SP Jr, Mc Lachlan MSF. (1981). Ageing and simple cysts of the kidney. Br J Radiol, 54:12.
Publisher | Google Scholor - Baert I, Steg A. (1977). Is the diverticulum of the distal and collecting tubules a preliminary stage of the simple cyst in the adult? J Urol, 118:707-710.
Publisher | Google Scholor - Tada S, Yamagishi J, Kobayashi H. et al. (1983). The incidence of simple renal cyst by computed tomography. Clin Radiol, 150:207.
Publisher | Google Scholor - Riyach O, Ahsaini M, Tazi K, Tazi MF, Mellas S, El Ammari JE, Khallouk A, El Fassi MJ, Farih MH. (2014). A huge renal cyst mimicking ascites: a case report. BMC Res Notes, 7:39.
Publisher | Google Scholor - Pedersen JF, Emamian SA, Nielsen MB. (1993). Simple renal cyst: relations to age and arterial blood pressure. Br J Radiol, 66:581-584.
Publisher | Google Scholor - Lezrek M, Fassi-Fehri H, Badet L, Marechal M, Martin X. (2002). Remission of erythrocytosis and hypertension after treatment of giant renal cyst. Urology, 164.
Publisher | Google Scholor - Sandeep S, Vikas K, Harminder P, Dinesh G. (2006). A case report: an unusual cause of giant renal mass. J Indian Acad Clin Med, 7(3):252-254.
Publisher | Google Scholor - Holl WH, Delporto GB, Keegan G, Turner WR. (1976). Simple renal cyst in children. J Urol, 115:465-466.
Publisher | Google Scholor - Paananen I, Hellström P, Leinonen S, Merikanto J, Perälä J, Päivänsalo M, Lukkarinen O. (2001). Treatment of renal cysts with single-session percutaneous drainage and ethanol sclerotherapy: longterm outcome. Urology, 57:30-33.
Publisher | Google Scholor - Ahallal Y, Khallouk A, Tazi MF, Tazi E. et al. (2009). Remission of hypertention after treatment of giant simple renal cyst: a case report. Cases J, 2:9152.
Publisher | Google Scholor













