

Case Report
Adnexal Torsion in A Postmenopausal Woman with A Giant Ovarian Mass: A Case Report and Review of the Literature
- Moad Belouad 1*
- Abdelhamid Benlghazi 1
- Ismail Belhaouz 2
- Abdelkrim Laalou 3
- Saad Benali 1
- Hamza Messaoudi 1
- Jaouad Kouach 1
1Department of Gynecology and Obstetrics, Military Hospital of Instruction Mohamed V, Rabat.
2Department of Gynecology and Obstetrics, Souissi Maternity Hospital, Chu Ibn Sina, Rabat, Morocco.
3Department of visceral surgery, gynaecology, proctology and sterilisation oued eddahab military hospital, Morocco.
*Corresponding Author: Moad Belouad, Department of Gynecology and Obstetrics, Military Hospital of Instruction Mohamed V, Rabat.
Citation: Belouad M, Benlghazi A, Belhaouz I, Laalou A, Benali S, et, al. (2024). Adnexal Torsion in A Postmenopausal Woman with A Giant Ovarian Mass: A Case Report and Review of the Literature. Journal of Women Health Care and Gynecology, BioRes Scientia Publishers. 4(1):1-6. DOI: 10.59657/2993-0871.brs.24.055
Copyright: © 2024 Moad Belouad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 03, 2024 | Accepted: July 31, 2024 | Published: August 10, 2024
Abstract
Ovarian cysts are in the majority of cases asymptomatic and can be discovered by chance during an ultrasound scan. They only become symptomatic when a complication occurs. We present a case of torsion of the right adnexa in a 67-year-old postmenopausal woman. We performed an adnexectomy in front of a 17 cm ischemic mass. On histopathological examination, the cyst was confirmed as benign serous cystadenoma of the ovary.
Keywords: ovarian cysts; menopause; adnexectomy
Background
The discovery of an adnexal mass in the postmenopausal period is a frequent situation and concerns 15 % of this population [1]. But only 1.7 % of these cysts exceed 5 cm. The definition of large ovarian cysts ranges from those measuring more than 10 cm in diameter on preoperative scans to those that extend above the umbilicus [2]. Serous cystadenoma 34% and mucinous cystadenoma 12% are the most frequent benign ovarian tumors [3] . Large ovarian serous cystadenoma is rare. In the literature, a limited number of cases of large ovarian cysts have been reported sporadically, especially in aged patients. We report the case of a 67-year-old postmenopausal woman with a giant right ovarian cyst (17 × 14 × 12cm) with adnexal torsion. Given her age and menopausal status, we performed an adnexectomy. On histopathological examination, the cyst was confirmed to be a benign serous cystadenoma of the ovary.
Case Presentation
we report the case of a 67-year-old woman, post-menopausal for 17 years, who was referred to our hospital from the local health Centre. She is hypertensive on bisoprolol 5 mg once a day with a history of hip replacement surgery for 07 years.
At the time of the consultation, she was symptomatic and complained of acute pelvic pain for a week with aggravation on the day of her consultation, with the appearance of vomiting, and a notion of constipation.
On general examination, she weighed 69 kg. The abdominal examination associated with the vaginal touch revealed a lateral uterine mass reaching the umbilicus, it was mobile and very painful to palpate. With a difficult abdominal examination due to the installation of abdominal contracture. On vaginal examination, the cervix was normal. Tumor markers were within normal limits, and CA 125 revealed 12 U/ml. Radiological ultrasound revealed a uterus of normal size and shape with a thin endometrium of 4 mm. A large right adnexal cyst, unilocular, thin-walled and smooth, and clear an echogenic content, measuring approximately 16.5 × 12cm.
We completed an abdominal and pelvic CT scan which was in favor of a thin-walled cystic mass with fluid content measuring 17× 14cm× 12cm. We planned adnexectomy given her age and her menopausal status. The abdomen was opened through a low transverse incision. We found an ischemic right ovarian cyst with early necrosis measuring approximately 16× 14 cm in size (Figure 1 et 2); no healthy ovarian tissue was seen separately. The right tube was adherent and stretched over the cyst. The left tube, left ovary, and uterus were found healthy. There were no preoperative complications.
On histopathological examination, the cyst was bilocular with a smooth, thin wall and lined with a single layer of occasional cuboidal epithelial cells.
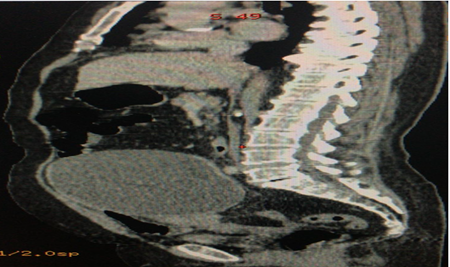
Figure 1: Abdominal-pelvic CT scan with sagittal section showing a 17 cm ovarian mass in a 67-year-old menopausal woman.
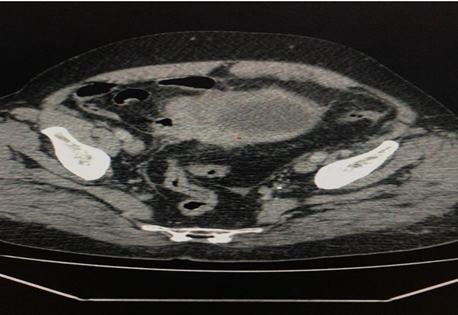
Figure 2: Abdominal-pelvic CT scan with axial section showing a 17 cm ovarian mass in a 67-year-old menopausal woman.
His postsurgical phase was considered normal. The onset of walking and ambulation occurred 12 hours after surgery. She was discharged on the third postoperative day in excellent condition.
Discussion
Adnexal torsion is a rare emergency condition that happens at any age. Adnexal torsion happens in 2-15% of women who have had previous surgical treatment for adnexal masses or cysts. Most adnexal and/or ovarian torsions occur at reproductive age and are not as frequent at postmenopausal age [4].
Serous tumors develop by invagination of the surface epithelium of the ovary and secrete serous fluid. Generally benign and produce non-specific symptoms as a feeling of pressure in the lower abdomen and symptoms of the gastrointestinal and urinary systems [5]. The most frequent symptoms of adnexal torsion and/or ovarian torsion a are acute abdominal pain, nausea and vomiting. The duration of pain before admission is generally longer in the postmenopausal group. This longer period may be explained by a delay in referral for gynecological evaluation, as this group of patients may be considered primarily for more common reasons of acute abdominal pain. Long duration of pain may suggest adnexal necrosis and ischemia [6].
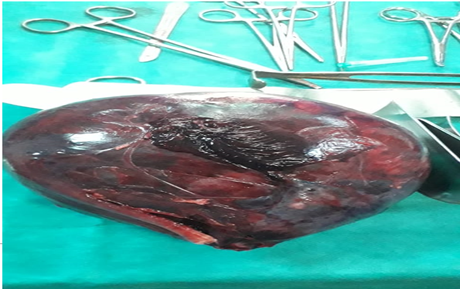
Figure 3: Postoperative image of the excised adnexa, including the ovary, containing the ovarian cyst and the fallopian tube and showing the beginning of necrosis.
Ultrasound is the most important diagnostic tool in cases of suspected adnexal affection. Magnetic resonance imaging (MRI) is useful in diagnosing adnexal/ovarian torsion and can show additional detail about the components of the ovarian mass [7].
The rate of malignancy in premenopausal women with ovarian torsion is considered low with rates of 0.5% to 2.4% [8]. In contrast, in postmenopausal patients, the global incidence of malignancy is highest, and ovarian preservation in this population is less important. As such, salpingo-oophorectomy is reasonable to exclude malignancy and prevent recurrence.
In most studies, laparoscopic surgery with ovarian preservation was performed in the vast majority of premenopausal women, whereas 50% of postmenopausal women were treated with laparotomy and radical surgery in most cases [6].
laparoscopic surgery should be performed as the first approach, while keeping in mind the option of conversion to laparotomy if necessary, and adnexectomy is generally the treatment of choice in any postmenopausal woman.
This case report presents a rare case of adnexal torsion in a postmenopausal woman to emphasize that adnexal torsion can happen at all ages and that the existence of an ovarian mass or cyst predisposes to adnexal torsion at any age.
Conclusion
Even adnexal torsion in postmenopausal women is a rare event, it should not be overlooked. A longer delay between admission and surgery may be attributed to the rare and irregular symptoms of the disease in this age group. Ovarian malignancy is not uncommon in this group of patients, so consideration should be given to preparation for more extensive surgery.
Declarations
Conflict of interest
No conflict of interest.
Funding
No funding
Consent
Informed written consent obtained from the patients.
References
- Dørum A, Blom GP, Ekerhovd E, Granberg S. (2005). Prevalence and histologic diagnosis of adnexal cysts in postmenopausal women: an autopsy study. American journal of obstetrics and gynecology, 192(1):48-54.
Publisher | Google Scholor - Agrawal SP, Rath S, Aher G, Gavali U. (2015). Large ovarian tumor: A case report. International Journal of Scientific Study, 3(3):144-146.
Publisher | Google Scholor - Kehila M, Kebaili S, Hidar S, Boughizane S. (2014). Tumeurs de l'ovaire chez la femme ménopausée: à propos de 100 cas et revue de la literature. The Pan African Medical Journal, 19.
Publisher | Google Scholor - Ci H, Hong M, Ding D. (2017). A review of ovary torsion. 29(3):143-147.
Publisher | Google Scholor - Messaoudi H, Guelzim K, Belouad M, Benlghazi A, Kouach J. (2021). Masse géante de l’ovaire en périménopause: à propos d’un cas. The Pan African Medical Journal, 38.
Publisher | Google Scholor - Cohen A, Solomon N, Almog B, Cohen Y, Tsafrir Z, Rimon E, et al. (2017). Adnexal torsion in postmenopausal women: clinical presentation and risk of ovarian malignancy. Journal of Minimally Invasive Gynecology, 24(1):94-97.
Publisher | Google Scholor - Naffaa L, Deshmukh T, Tumu S, Johnson C, Boyd KP, Meyers AB. (2017). Imaging of acute pelvic pain in girls: ovarian torsion and beyond☆. Current problems in diagnostic radiology, 46(4):317-329.
Publisher | Google Scholor - Herman HG, Shalev A, Ginath S, Kerner R, Keidar R, Bar J, et al. (2015). Clinical characteristics and the risk for malignancy in postmenopausal women with adnexal torsion. Maturitas, 81(1):57-61.
Publisher | Google Scholor










