

Case Report
A Rare Case of Primary Glioblastoma Multiforme in the Cerebellum, Case Report and Literature Review
1 Department of Neurosurgery, Mashhad University of Medical Sciences, Iran.
2 Resident Physician in Adult Neurology University of Toronto, Canada.
*Corresponding Author: Farajirad M, Department of Neurosurgery, Mashhad University of Medical Sciences, Iran.
Citation: Farajirad M, Farajirad E, Mohazzab-Torabi S and Ganavizian M. (2023). A Rare Case of Primary Glioblastoma Multiforme in the Cerebellum, Case Report and Literature Review. Journal of Clinical Surgery and Surgical Research, BRS Publishers. 2(2); DOI: 10.59657/2992-9989.brs.23.011
Copyright: © 2023 Mohammad Farajirad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 09, 2023 | Accepted: May 22, 2023 | Published: May 29, 2023
Abstract
Glioblastoma multiforme (GBM) is a highly aggressive and malignant tumor that can arise in the central nervous system, including the cerebellum. We presented a case of GBM in cerebellum who was the 27 years - old male presented with gate ataxia and dysphagia. MRI demonstrated brain mass in right cerebellum with enhancement. Patient underwent surgical resection, followed by radiation therapy and chemotherapy. Further researches are needed to identify optimal treatment strategies and improve outcomes for patients with GBM in the spinal cord. Close monitoring and follow-up care are essential to manage potential complications and optimize quality of life for affected individuals.
Keywords: neuro-oncology; glioblastoma multiform; cerebellum
Introduction
Glioblastoma, also known as glioblastoma multiforme or GBM, is the most aggressive and deadliest form of glioma, with a median survival time of around 15 months [1]. When glioblastoma occurs in the cerebellum, it is called cerebellar glioblastoma. Cerebellar glioblastoma is a relatively rare form of brain tumor, accounting for less than 5% of all primary brain tumors [2]. The symptoms of cerebellar glioblastoma can vary depending on the location and size of the tumor. Common symptoms include headache, nausea, vomiting, dizziness, difficulty walking or maintaining balance, and changes in vision or hearing. Because the cerebellum is located near the brainstem, which controls vital functions such as breathing and heart rate, cerebellar glioblastoma can also cause life-threatening complications. The treatment of cerebellar glioblastoma typically involves a combination of surgery, radiation therapy, and chemotherapy [3]. However, due to the aggressive nature of this tumor, complete surgical resection is often difficult to achieve. In addition, cerebellar glioblastoma tends to spread rapidly to other parts of the brain, making it challenging to treat. As a result, the prognosis for patients with cerebellar glioblastoma is generally poor, and survival rates remain low despite advances in treatment [4]. Despite their rarity, glioblastomas in the cerebellum pose unique challenges for diagnosis and treatment due to the complex anatomy and function of this brain region. Diagnosis typically involves imaging studies such as MRI or CT scans, followed by a biopsy to confirm the presence of a glioblastoma [5]. Despite advances in treatment, the prognosis for GBM in the spinal cord remains poor, with a median survival time of less than two years. However, early detection and prompt treatment can help improve outcomes for patients with this condition. Close monitoring and follow-up care are essential to manage potential complications and optimize quality of life for affected individuals. Following, we will focus on rare case of young male with cerebellar mass which was diagnosed with GBM in further evaluation.
Case Presentation
A 27-years-old male presents to the emergency department with a history of progressive headaches and vomiting for the past month. He reports a recent onset of difficulty with balance and coordination. His past medical history is unremarkable. On examination, the patient appears uncomfortable but is alert and oriented. He has mild dysarthria and nystagmus. There is no facial weakness or sensory deficit. The motor system is intact, but he has ataxia and dysmetria on the left side. Cerebellar testing reveals bilateral dysmetria, dysdiadochokinesia, and intention tremor. Funduscopy is normal, and there is no papilledema.
An MRI of the brain confirms the presence of a 2 cm x 2.5 cm heterogeneously enhancing mass in the right cerebellar hemisphere with perilesional edema and hydrocephalus. (Figure 1A, 1B). Contrast-enhanced CT of the chest, abdomen, and pelvis shows no evidence of metastatic disease. A surgical procedure was carried out to perform posterior fossa craniotomy. Via transhemispheric approach, tumor was near totally resected. Microscopic analysis of the biopsy showed the presence of neoplastic cells with vascular proliferation and focal necrosis when viewed under hematoxylin and eosin stains (Figures 2). Isocitrate dehydrogenase-1 (IDH1) was not detected upon immunohistochemical staining (Figure 3). These findings indicate the presence of giant cell glioblastoma, IDH wild-type, World Health Organization grade IV in the thoracic spinal cord. Genetic testing for mutant-type IDH1 was not performed on the tumor biopsies due to the negative IDH1 immunohistochemical staining.
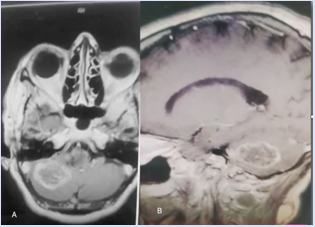
Figure 1: Preoperative axial (A) and sagittal (B) MRI; significant for enhancing heterogenous mass in right cerebellum.
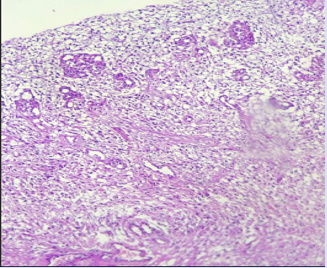
Figure 2: Neoplastic cells with vascular proliferation and focal necrosis on hematoxylin and eosin stains (100×).
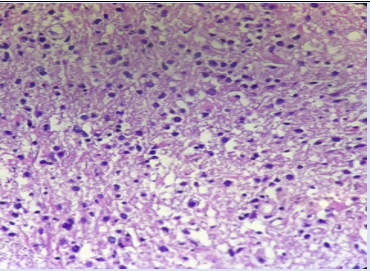
Figure 3: Negative immunohistochemical staining for isocitrate dehydrogenase-1 (200×).
Postoperative MRI showed significant improvement in spinal cord compression, with no evidence of residual tumor. The patient was then started on a course of radiation therapy and chemotherapy, consisting of temozolomide. He initially showed some improvement in neurological symptoms, with increased lower extremity strength and sensation. The patient undergoes a craniotomy and gross total resection of the tumor. The pathology report confirms the diagnosis of glioblastoma multiforme (GBM). The patient undergoes adjuvant radiation therapy and temozolomide chemotherapy.
The patient has an uneventful recovery from surgery and completes radiation therapy and chemotherapy without significant complications. The patient is started on second-line chemotherapy but ultimately succumbs to the disease six months after the initial diagnosis.
Discussion
Glioblastoma (GBM) is the primary intracranial tumor that predominantly affects adults. Despite its potential occurrence across all age groups, a significant majority of cases affect individuals in their sixth decade with an additional surge observed among patients within their first decade. (6) Further epidemiological data suggests GBM is more common among males with a 2:1 ratio compared to females [7].
Infratentorial glioblastoma multiforme (GBM) is a rare occurrence, and only a small percentage of brain tumors (0.24 to 1.00%) present as cerebellar GBM [8]. Symptoms often include increased intracranial pressure such as headaches, nausea, vomiting and ataxia; other symptoms may consist of dizziness, neck pain and mental confusion [9]. Preoperative suspicion for cerebellar GBM usually tends to be low but certain imaging features on computed tomography or magnetic resonance imaging could aid in diagnosis over others like metastatic disease or anaplastic astrocytoma among adults [10. While the cause behind the infrequency of cerebellar GBMs remains unclear amongst most experts, one proposed theory suggests that malignant transformation happens less frequently in astrocytes located within the cerebellum when compared to those found elsewhere in the brain [11].
Despite the fact that cerebellar astrocytes are less prone to becoming malignant, there are several proposed factors that suggest radiotherapy may trigger the anaplastic progression of cerebellar astrocytic cells [12]. The link between radiotherapy and the development of malignant astrocytoma in the cerebellum remains uncertain. However, a study conducted by Maat-Schieman et al. reported a case of midline cerebellar astrocytoma that occurred after radiotherapy following craniopharyngioma [13]. The transformation of pilocytic astrocytoma, medulloblastoma, and other posterior fossa midline tumors into GBM has also been reported. Nevertheless, demonstrating their malignant transformation is challenging since most of these cases received radiation therapy after the surgery [14].
CT with contrast enhancement is a crucial diagnostic tool for identifying cerebellar GBM. However, other diseases like metastases, abscess, and cerebellar infarcts can have similar imaging patterns to GBM, making it difficult to differentiate them [15]. Among adults with posterior fossa brain masses, metastatic tumors are the most frequent alternative diagnosis. Cerebellar GBMs are typically characterized by solid tumors that enhance contrast or central hypodensity indicating necrosis [16]. Researchers have discovered that cerebellar GBM patients usually have minimal peritumoral edema, and CT scans can differentiate GBM from cerebellar metastasis through peritumoral edema or mass effect [17]. MRI has improved the accuracy of lesion characterization due to its high tissue resolution and minimal bone artifacts. Perfusion-weighted MR imaging can differentiate gliomas from metastases by examining the variations in vascularity and metabolite levels in the periphery of the tumor [18]. Gliomas have higher relative cerebral blood volumes in peritumoral areas than metastases. Spectroscopic MR examination reveals the presence of elevated choline levels in the peritumoral areas of gliomas, decreased NAA levels due to the loss of neuronal elements, and the presence of a lactate peak, all of which are indicators of a higher degree of malignancy frequently found in GBM [19].
On contrast enhanced T1 weighted images, an abscess presents a clear and slender enhancing rim. Meanwhile, diffusion weighted images exhibit an increase in signal intensity within the abscess, and the ADC map reveals a significant decrease in signal centrally [20]. It is worth noting that primary or metastatic neoplasms tend to appear as low signal on diffusion weighted images. Additionally, after infarction, contrast enhancement may occur 1 to 2 weeks later, known as the "fogging effect," possibly due to a reduction in edema and protein leakage from cell lysis. However, this lesion appears virtually normal on T2 weighted images [21]. Cerebellar and infratentorial GBMs share a similar biological behavior. However, young patients with cerebellar GBMs may have a better prognosis than those with supratentorial GBMs, similar to anaplastic astrocytomas (AAs), which have a longer survival time. It is worth noting that the median survival time for cerebellar GBMs is approximately 19 months [22].
When it comes to malignant glial tumors, it's always advisable to aim for a complete removal of the tumor. However, the infiltrative nature of glioblastoma often makes it challenging to achieve this goal [23]. Still, the infratentorial region poses a unique problem of brainstem invasion, which significantly affects the patient's prognosis [24]. In cases of tumor recurrence, it almost always happens locally, but there are rare instances of extra-cerebellar failure, such as spinal seeding through the CSF. Radiation therapy is an established treatment for malignant gliomas, but there's a debate about whether to deliver it solely to the posterior fossa, the whole brain, or the neuraxis [25]. The role of chemotherapy isn't entirely established, but it's the only reasonable complementary therapy for younger children. Considering that infratentorial glioblastomas have the same histological characteristics as supratentorial ones, using concomitant and adjuvant chemotherapy seems reasonable for its treatment.
Conclusion
Glioblastoma in the cerebellum is a highly aggressive and malignant brain neoplasm, characterized by a high degree of cellular proliferation, necrosis, and angiogenesis. It is the most common primary brain tumor in adults, accounting for 15-20% of all brain tumors, and carries a poor prognosis, with a median survival time of approximately 15 months. The diagnosis of glioblastoma in the cerebellum is based on a combination of clinical symptoms, neuroimaging studies, and histopathological examination. Research into the pathogenesis of glioblastoma in the cerebellum is ongoing, with a focus on identifying novel therapeutic targets and developing personalized treatment approaches. Clinical trials of targeted therapies, immunotherapies, and gene therapies are underway, with promising early results. Early detection and accurate diagnosis of glioblastoma in the cerebellum remain crucial for improving outcomes and increasing survival rates.
References
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. (2007). The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 114:97-109.
Publisher | Google Scholor - Nitta H, Hayase H, Moriyama Y, Yamashima T, Yamashita J. (1993). Gliosarcoma of the posterior cranial fossa: MRI findings. Neuroradiology. 35:279-280.
Publisher | Google Scholor - Kawaguchi S, Kashiwaba T, Koiwa M, Shimoyama M, Kobayashi N, Fukushi Y, et al. (1991). Two autopsied cases of radiation-induced gliosarcoma. No Shinkei Geka. 19:285-290.
Publisher | Google Scholor - Alatakis S, Stuckey S, Siu K, McLean C. (2004). Gliosarcoma with osteosarcomatous differentiation: review of radiological and pathological features. J Clin Neurosci. 11:650-656.
Publisher | Google Scholor - Malde R, Jalali R, Muzumdar D, Shet T, Kurkure P. (2004). Gliosarcoma occurring 8 years after treatment for a medulloblastoma. Childs Nerv Syst. 20:243-246.
Publisher | Google Scholor - Barresi V, Cerasoli S, Morigi F, Cremonini AM, Volpini M, Tuccari G. (2006). Gliosarcoma with features of osteoblastic osteosarcoma: a review. Arch Pathol Lab Med. 130:1208-1211.
Publisher | Google Scholor - Babu R, Sharma R, Karikari IO, et al. (2013). Outcome and prognostic factors in adult cerebellar glioblastoma. J Clin Neurosci. 20:1117-1121.
Publisher | Google Scholor - Kuroiwa T, Numaguchi Y, Rothman MI, et al. (1995). Posterior fossa glioblastoma multiforme: MR findings. AJNR Am J Neuroradiol. 16:583-589.
Publisher | Google Scholor - Roth JG, Elvidge AR. (1960). Glioblastoma multiforme: A clinical survey. J Neurosurg. 17:736-750.
Publisher | Google Scholor - Mattos JP, Marenco HA, Campos JM, et al. (2006). Cerebellar glioblastoma multiforme in an adult. Arq Neuropsiquiatr. 64:132-135.
Publisher | Google Scholor - Louis DN, Ohgaki H, Wiestler OD, et al. (2007). The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 114:97-109.
Publisher | Google Scholor - Lieberman KA, Fuller CE, Caruso RD, Schelper RL. (2001). Postradiation gliosarcoma with osteosarcomatous components. Neuroradiology. 43:555-558.
Publisher | Google Scholor - Carstens PH, Johnson GS, Jelsma LF. (1995). Spinal gliosarcoma: a light, immunohistochemical and ultrastructural study. Ann Clin Lab Sci. 25:241-246.
Publisher | Google Scholor - Beaumont TL, Kupsky WJ, Barger GR, Sloan AE. (2007). Gliosarcoma with multiple extracranial metastases case report and review of the literature. J Neurooncol. 83:39-46.
Publisher | Google Scholor - Rodriguez FJ, Scheithauer BW, Jenkins R, Burger PC, Rudzinskiy P, Vlodavsky E, et al. (2007). Gliosarcoma arising in oligodendroglial tumors (
Publisher | Google Scholor - Rees JH, Smirniotopoulos JG, Jones RV, Wong K. (1996). Glioblastoma multiforme: radiologic-pathologic correlation. Radiographics. 16:1413-1438.
Publisher | Google Scholor - Witwer BP, Salamat MS, Resnick DK. (2000). Gliosarcoma metastatic to the cervical spinal cord: case report and review of the literature. Surg Neurol. 54:373-378.
Publisher | Google Scholor - Fischer S, Lee W, Aulisi E, Singh H. (2007). Gliosarcoma with intramedullary spinal metastases: a case report and review of the literature. J Clin Oncol. 25:447-449.
Publisher | Google Scholor - Demir MK, Hakan T, Akinci O, Berkman Z. (2005). Primary cerebellar glioblastoma multiforme. Diagn Interv Radiol. 11:83-86.
Publisher | Google Scholor - Mattos JP, Marenco HA, Campos JM, Faria AV, Queiroz LS, Borges G, et al. (2006). Cerebellar glioblastoma multiforme in an adult. Arq Neuropsiquiatr. 64:132-135.
Publisher | Google Scholor - Gupta V, Goyal A, Sinha S, Singh AK, Tatke M, Kumar S, et al. (2003). Glioblastoma of the cerebellum. A report of 3 cases. J Neurosurg Sci. 47:157-164.
Publisher | Google Scholor - Reuss DE, Kratz A, Sahm F, Capper D, Schrimpf D, Koelsche C, Hovestadt V, Bewerunge-Hudler M, Jones DT, Schittenhelm J et al. (2015). Adult IDH wild type astrocytomas biologically and clinically resolve into other tumor entities. Acta Neuropathol. 130:407-417.
Publisher | Google Scholor - Stichel D, Ebrahimi A, Reuss D, Schrimpf D, Ono T, Shirahata M, Reifenberger G, Weller M, Hanggi D, Wick W et al (2018) Distribution of EGFR amplification, combined chromosome 7 gain and chromosome 10 loss, and TERT promoter mutation in brain tumors and their potential for the reclassification of IDHwt astrocytoma to glioblastoma. Acta Neuropathol. 136:793-803.
Publisher | Google Scholor - Grahovac G, Tomac D, Lambasa S, et al. (2009). Cerebellar glioblastomas: Pathophysiology, clinical presentation and management. Acta Neurochir. 151:653-657.
Publisher | Google Scholor - Hamasaki K, Nakamura H, Ueda Y, et al. (2010). Radiation-induced glioblastoma occurring 35 years after radiation therapy for medulloblastoma: case report. Brain Tumor Pathol. 27:39-43.
Publisher | Google Scholor














