

Case Report
A Rare Case of Cholecystitis Secondary to Prolonged Ketamine Use in a Patient with Major Depressive Disorder
MBBS Smt. NHL Municipal College Ahmedabad, Gujarat, India.
*Corresponding Author: Abhishek Chaudhary, MBBS Smt. NHL Municipal College Ahmedabad, Gujarat, India.
Citation: Chaudhary A. (2024). A Rare Case of Cholecystitis Secondary to Prolonged Ketamine Use in a Patient with Major Depressive Disorder, International Clinical Case Reports and Reviews, BioRes Scientia Publishers. 2(1):1-3. DOI: 10.59657/2993-0855.brs.24.011
Copyright: © 2024 Abhishek Chaudhary, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 22, 2024 | Accepted: June 07, 2024 | Published: June 12, 2024
Abstract
We present a rare case of cholecystitis secondary to prolonged ketamine use in a 48-year-old male with a history of major depressive disorder. The patient presented to the emergency room with complaints of right upper quadrant abdominal pain, fever, and jaundice. Imaging studies revealed an inflamed gallbladder consistent with acute cholecystitis. Further history revealed that the patient had been undergoing ketamine therapies for depression and anxiety through an online company not approved by regulatory authorities. This case underscores the importance of considering ketamine abuse in the differential diagnosis of cholecystitis, particularly in patients with atypical presentations and a history of substance use. Clinicians should remain vigilant for potential complications of ketamine use beyond its primary effects on the central nervous system and be aware of the risks associated with unregulated ketamine therapies.
Keywords: cholecystitis; prolonged ketamine; depressive disorder
Introduction
Ketamine, originally devised as an anesthetic agent, has transcended its conventional role and garnered significant attention for its versatile applications across diverse medical domains, spanning anesthesia, pain management, and psychiatric treatment. Recent developments have witnessed the emergence of online platforms offering ketamine for depression and anxiety, despite lacking FDA approval. Concerningly, reports have surfaced indicating a potential association between ketamine use and cholecystitis, prompting scrutiny into its safety profile. Cholecystitis, characterized by inflammation of the gallbladder, conventionally arises from gallstones or biliary obstruction. However, emerging evidence suggests a plausible link between ketamine use and hepatobiliary complications, including cholecystitis. Despite its primary effects on the central nervous system, ketamine's secondary impacts on the hepatobiliary system may precipitate inflammatory cascades and disrupt gallbladder function. This introduction endeavors to delve in to the potential nexus between ketamine use and cholecystitis, underscoring the necessity for clinicians to factor in ketamine abuse when evaluating patients with cholecystitis, particularly those exhibiting atypical presentations or a history of substance use. By shedding light on this association, healthcare providers can enhance their awareness and vigilance in identifying and managing the hepatobiliary complications linked to ketamine use.
Narrative
A 48-year-old male with a history of major depressive disorder, presented to the emergency room with complaints of severe right upper quadrant abdominal pain, fever, and jaundice. His symptoms had progressively worsened over the past week, prompting him to seek medical attention. On examination, the patient appeared visibly uncomfortable, with tenderness noted upon palpation of the right upper quadrant and signs of scleral icterus.
Upon further inquiry, the patient revealed a history of chronic ketamine use for the management of his depressive symptoms. He disclosed that he had been undergoing ketamine therapies through an online platform, Mind bloom, which offered ketamine treatments for depression and anxiety without FDA approval. Despite initial relief from his psychiatric symptoms, the patient noticed the onset of abdominal discomfort following several months of regular ketamine use.
Laboratory investigations revealed elevated liver enzymes, bilirubin levels, and inflammatory markers, suggestive of hepatobiliary involvement. Imaging studies, including ultrasound and computed tomography (CT) scan, demonstrated signs of acute cholecystitis, with gallbladder wall thickening and pericholecystic fluid collection.
Given the severity of his symptoms and imaging fundings, the patient was promptly admitted for further evaluation and management. He was initiated on intravenous fluids, broad- spectrum antibiotics, and analgesics for pain relief. Surgical consultation was sought, and after stabilization, the patient underwent laparoscopic cholecystectomy, which confirmed the diagnosis of acute cholecystitis. Postoperatively, the patient's symptoms gradually improved, and he was discharged home with instructions for close follow-up with his primary care physician. He was counseled on the risks associated with ketamine use, particularly its potential hepatobiliary complications, and advised to refrain from further ketamine therapies.
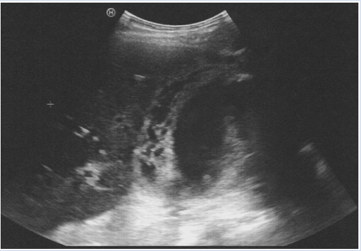
Figure: The gallbladder wall is thickened, with outer and inner hyperechoic layers and a central hypoechoic layer
Discussion
The presented case underscores the potential hepatobiliary complications associated with ketamine use, particularly in the context of unregulated therapies offered by online platforms. Cholecystitis, although traditionally linked to gallstones or biliary obstruction, can manifest as a rare adverse effect of ketamine, as observed in this patient.
Ketamine's primary mechanism of action involves antagonism of N-methyl-D-aspartate (NMDA) receptors, leading to dissociation and analgesia. However, its secondary effects on the hepatobiliary system remain less understood. While the precise pathophysiological mechanisms underlying ketamine-induced cholecystitis are not fully elucidated, it is hypothesized that ketamine metabolites may directly or indirectly trigger inflammatory responses within the gallbladder, leading to acute inflammation and dysfunction.
In this case, the patient's history of chronic ketamine use, coupled with the onset of right upper quadrant abdominal pain, fever, and jaundice, prompted further evaluation for hepatobiliary pathology. Laboratory funding's of elevated liver enzymes and bilirubin levels, in conjunction with imaging studies demonstrating signs of acute cholecystitis, supported the diagnosis. Prompt surgical intervention in the form of laparoscopic cholecystectomy provided definitive treatment and confirmed the diagnosis.
The association between ketamine use and cholecystitis warrants careful consideration by healthcare providers, particularly in patients presenting with atypical symptoms or a history of substance abuse. Clinicians should maintain a high index of suspicion for ketamine- induced cholecystitis, as delayed recognition may lead to complications such as gallbladder perforation, abscess formation, or sepsis.
Furthermore, the proliferation of online platforms offering ketamine therapies for psychiatric conditions without regulatory over sight poses significant public health concerns. Patients may be exposed to potential harms without adequate monitoring or guidance. Healthcare providers should educate patients about the risks associated with unregulated ketamine use and encourage them to seek evidence-based treatments from licensed healthcare professionals.
In conclusion, this case highlights the importance of vigilance in recognizing and managing hepatobiliary complications associated with ketamine use. Clinicians should remain attentive to the potential adverse effects of ketamine, particularly in patients with chronic use or atypical presentations. Additionally, regulatory measures are needed to mitigate the risks posed by unregulated ketamine therapies offered by online platforms.
Patient Perspective
The agony in my abdomen drove me to the emergency room, a stark contrast to the relief I once sought from ketamine treatments for my depression. Initially promising, these therapies now seem to have led me to this excruciating bout of cholecystitis. As I lay in the hospital bed, grappling with regret and questioning the price of my pursuit for mental well-being, I'm determined to approach future treatments with greater caution and mindfulness.
Conclusion
This case highlights the significance of recognizing ketamine-induced cholecystitis as a potential complication of chronic ketamine use, particularly in patients seeking regulated treatments for psychiatric conditions. Prompt diagnosis and management, as demonstrated through surgical intervention in this case, are crucial in mitigating potential complications. Furthermore, the proliferation of online platforms offering ketamine therapies without regulatory oversight underscores the need for healthcare providers to educate patients about the associated risks and advocate for evidence-based treatments. By raising awareness and implementing regulatory measures, clinicians can improve patient outcomes and promote safer treatment practices in this population.
Acknowledgments
We extend our sincere appreciation to the patient for their consent to share their medical experience in this case report. We also wish to acknowledge the healthcare professionals involved in the diagnosis, treatment, and care of the patient, whose expertise and dedication were invaluable. Furthermore, we recognize the contributions of the medical literature and research community, which have enhanced our understanding of ketamine-induced cholecystitis and informed the discussion presented in this report.
References
- Anderson DJ, Zhou J, Cao D, et al. (2022). Ketamine-Induced Cystitis: A Comprehensive Review of the Urologic Effects of This Psychoactive Drug. Health Psychology Research, 10(3).
Publisher | Google Scholor - Elaina M Blair, Katharine L Dickson, Michelle A O’Malley. (2021). Microbial communities and their enzymes facilitate degradation of recalcitrant polymers in anaerobic digestion. Current Opinion in Microbiology, 64:100-108.
Publisher | Google Scholor - The Keta-Cov research group. (2021). Intravenous ketamine and progressive cholangiopathy in COVID-19 patients. Journal of Hepatology, 74(5):1243-1244.
Publisher | Google Scholor - Johannesson, Elisabet, Simrén, Magnus, Strid, Hans, Bajor, Antal, Sadik, Riadh. (2011). Physical Activity Improves Symptoms in Irritable Bowel Syndrome: A Randomized Controlled Trial. American Journal of Gastroenterology, 106(5):915-922.
Publisher | Google Scholor - KL Lui, WK Lee, Michael KK Li. (2014). Ketamine-induced cholangiopathy. Hong Kong Med J, 20(1):e1-e2.
Publisher | Google Scholor











