

Case Report
A Clinical Study of Gastric Outlet Obstruction
- Mayur G. Rabari
- Akanksha Patel *
- Natasha Mithiborwala
Department of General Surgery Smt. NHL Municipal Medical College, SVP Institute of Medical sciences & Research, Ahmedabad, India.
*Corresponding Author: Akanksha Patel, Department of General Surgery Smt. NHL Municipal Medical College, SVP Institute of Medical sciences & Research, Ahmedabad, India.
Citation: Mayur G. Rabari, Patel A, Mithiborwala N. (2023). A Clinical Study of Gastric Outlet Obstruction, Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers, 2(3):1-7. DOI: 10.59657/2992-9989.brs.23.016
Copyright: © 2023 Akanksha Patel, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 18, 2023 | Accepted: October 02, 2023 | Published: October 11, 2023
Abstract
Background: Diagnosis of Gastric outlet obstruction (GOO) is a challenge in 3rd world countries. Gastric outlet obstruction occurs because of impeding emptying of the stomach mechanically, and it has varied causes. This study was taken up to know the etiological factors and management.
Methods: This was a descriptive prospective study done at Smt. NHL Municipal Medical College for a period of 1 year from June 2022 to May 2023. A set of inclusion and exclusion criteria were defined and followed. Upper gastrointestinal endoscopy (OGD) was done in all cases while Barium meal study was done in a few cases to make the diagnosis. Relevant operative procedure was done, and patients were managed post operatively.
Results: Cicatrized Duodenalulcer (DU) was the commonest cause followed by Carcinoma Pyloric antrum (Ca PA). Majority of the patients were males (68%) with male to female ratio of 2.13:1. Vomiting was one of the major presenting symptoms in all the patients.
Conclusions: Cicatrized DU was the commonest cause for GOO in present study. Present study highlights the increasing incidence of Ca PA. This could be due to better management of DU at an early stage.
Keywords: cicatrized duodenal ulcer; carcinoma pyloric antrum; gastric outlet obstruction
Introduction
Diagnosis of Gastric outlet obstruction (GOO) is a challenge in 3rd world countries. GOO is a clinical condition occurred due to impeding gastric emptying either mechanically, complete or incomplete obstruction of distal stomach, pylorus or proximal duodenum [1]. The causes include both benign and malignant conditions [2]. GOO is the clinical, pathological and physiological outcome of diseases producing mechanical obstruction to gastric emptying [3].This may be due to internal causes [1,4]. Incidence is not known in 3rd world countries. It occurs in approximately 2.2% of Chronic Duodenal Ulcer (DU) patients [5]. It accounts for 5-7% of complications of ulcer disease. In developed countries, GOO occurs more in older age patient and it is associated with malignancy [6,7]. In recent times malignancy ascribing to GOO in 50-80% of cases has been note [6,7]. This study was taken up to review the changing trend in the clinical presentation, etiology and the management of GOO.
Methods
A total of 50 patients were included at Smt. NHL MMC, Ahmedabad. This study was done over a period of 1 years from June 2022 to May 2023. This was a descriptive retrospective study.
Inclusion criteria
Projectile vomiting with presence of undigested food materials, gastric peristalsis and mass. Overnight Gastric aspirate of >300ml in a NBM patient. Positive Saline load test: Retention of more than 400 ml of normal saline 30 minute safter administration of 800 ml of NS. Gastric outlet obstruction proven on Oesophago-Gastro-Duodenoscopy.
Exclusion criteria
Patients <18>400 ml in aspiration after half an hour was considered significant.
Detailed history, physical examination and investigations were done for pre-operative assessment in all cases. For diagnostic confirmation, Upper Gastrointestinal endoscopy was performed in every case. Biopsies were taken wherever required. In a few cases, Barium meal examination was done because of corrosive stricture as the scope couldn’t be passed beyond. Intra operative findings were noted down and cases were followed up in the post-operative period.
Preoperative dehydration was corrected with intravenous fluids. Continuous drainage of gastric contents through Ryle’s tube, helps in decreasing gastric decompression. Oral fluids were started according to the tolerance of the patient. Stomach wash was given preoperatively with Normal saline. Anemia was corrected using Packed cells and hypoproteinemia was corrected using Fresh frozen plasma transfusion.
Post-operative period
Vital sheet maintained, includes Temperature, pulse, blood pressure and respiratory rate. Ryle’s tube aspiration is done to decompress the stomach. IV fluids were infused immediately in the postoperative period, then the patients were shifted on oral fluids. On the 5th postoperative day, patients were given oral fluids and shifted gradually to solid foods according to tolerance of patients. Patients were mobilized as soon as possible. Routine antibiotics were given.
Results
A total of 50 patients were included in our study. Higher incidence was seen in the age group 41-50 years of age. The commonest cause in present study was cicatrised Duodenal ulcer(DU)- 48% followed by carcinoma pylorus- 38% (Table 1).
Table 1: Age and Etiology
| Age group | Carcinoma pyloric antrum | Cicatrized duodenal ulcer | Corrosive antral stricture | Others | Total |
| 18-20 | 0 | 0 | 0 | 0 | 0 |
| 21-30 | 0 | 2 (8.33%) | 1 (25%) | 0 | 3(6%) |
| 31-40 | 3 (15.79%) | 6 (25%) | 1 (25%) | 0 | 10(20%) |
| 41-50 | 5 (26.32%) | 9 (37.5%) | 2 (50%) | 0 | 16(32%) |
| 51-60 | 8 (42.11%) | 4 (16.67%) | 0 | 2 (66.67%) | 14(28%) |
| 61-70 | 2 (10.53%) | 3 (12.5%) | 0 | 1 (33.33%) | 6(12%) |
| 71-80 | 1 (5.26%) | 0 | 0 | 0 | 1(2%) |
| Total | 19(38%) | 24(48%) | 4(8%) | 3(6%) | 50 |
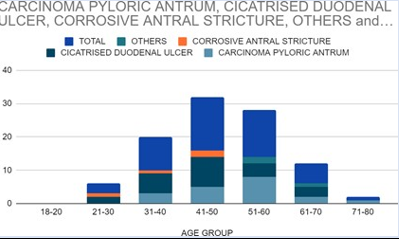
Figure 1
In higher age (>50yrs), carcinoma pyloric antrum was causing GOO more commonly than DU. In younger age groups (<50yrs>
Majority of the patients were males (68%)with male to female ratio of 2.13:1. Male to female ratio in Ca PA was 2.8:1 and in cicatrized DU was 1.89:1. 60% of the patients were smokers and they were found to have GOO secondary to cicatrized DU. Out of 50 patients, 50% were alcoholics. Alcoholism was seen to be more prevalent in low socioeconomic status populations (Figure 1). Vomiting was the predominant symptom in this study as seen in each and every case (100%) as common as abdominal pain, followed by loss of appetite which was seen in 88% of Ca PA patients and 62% of DU patients.
Table 2: Sex and Etiology
| Sex | Total number | Carcinoma antrum | Cicatrized duodenal ulcer | Corrosive antral stricture | Others |
| Male | 34 | 14 | 17 | 2 | 1 |
| Female | 16 | 5 | 9 | 1 | 1 |
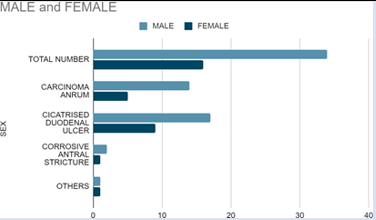
Figure 2
Table 3: Signs
| Signs | Total no (%) | Carcinoma antrum (%) | Cicatrised duodenal ulcer (%) | Corrosive antralstricture (%) | Others (%) |
| Pallor | 33 (66%) | 17 (89.47%) | 10 (41.67%) | 4 (100%) | 2 (66.67%) |
| Dehydration | 20 (40%) | 7 (36.84%) | 11 (45.83%) | 2 (50%) | 0 |
| Vgp | 26 (52%) | 10 (52.63%) | 15 (62.5%) | 0 | 1 (33.33%) |
| Epigastric tenderness | 24 (48%) | 4 (21.05%) | 16 (66.67%) | 4 (100%) | 0 |
| Mass | 14 (28%) | 14 (73.68%) | 0 | 0 | 0 |
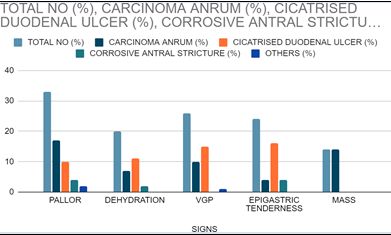
Figure 3
In the post-operative period, all the patients were given intravenous fluids, antibiotics and analgesics. Ryle's tube aspiration was done in all cases. Oral sips were allowed after Ryle’s tube removal. Patients were gradually changed to semi solid and then solid diets depending on their tolerance. Sutures were removed after the 14th postoperative day.
Table 4: Surgical Procedures Done
| Procedures | No of cases | Percentage |
| Carcinoma Antrum (19) | ||
| Billroth II Gastrectomy | 5 | 26.31% |
| Anterior Gastrojejunostomy | 10 | 52.63% |
| Anterior Gastrojejunostomy with jejunojejunostomy | 1 | 5.26% |
| Feeding jejunostomy | 3 | 15.79% |
| Cicatrizing duodenal ulcer (24) | ||
| Truncal Vagotomy with posterior gastrojejunostomy | 24 | 100% |
| Corrosive antral stricture (4) | ||
| Antrectomy with Billroth II anastomosis | 3 | 75% |
| Antrectomy + coloplasty + feeding jejunostomy | 1 | 25% |
| Feeding Jejunostomy | 0 | 0 |
| Others (3) | ||
| Triple bypass | 2 | 66.67% |
| Anteriorgastrojejunostomy | 1 | 33.33% |
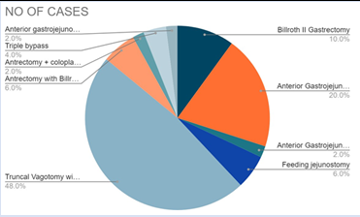
Figure 4
Table 5: Symptom distribution
| Carcinoma antrum | Cicatrized duodenal ulcer | Corrosive antralstricture |
Others | |
| Abdominal pain | 14 (73.68%) | 24 (100%) | 4 (100%) | 3(100%) |
| Vomiting | 19 (100%) | 24 (100%) | 4 (100%) | 3(100%) |
| Loss of weight | 17 (89.47%) | 7 (29.16%) | 4 (100%) | 3(100%) |
| Loss of appetite | 17 (89.47%) | 17 (70.83%) | 4 (100%) | 3(100%) |
| Malena | 4 (21.05%) | 0 | 1 (25%) | 0 |
| Hematemesis | 3 (15.79%) | 4 (16.67%) | 0 | 0 |
| H/o AcidPeptic disease | 0 | 0 | 2 (50%) | 3(100%) |
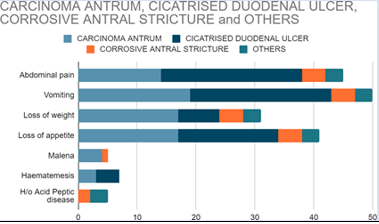
Figure 5
Discussion
Due to lack of uniformity in accepting the criteria in a case of GOO leads to differences in incidence and clinical features in different centers (Table 6). The most common cause of GOO was cicatrized DU followed by Ca PA in our study which is similar to studies done by Ellis H et al, Balint JA et al [8,9]. In recent times, the incidence of Ca PA has increased probably because of successful treatment of DU. Highest incidence was seen in the 5th decade in present study, similar to other studies [4]. In younger age groups GOO was found to be benign whereas malignant GOO was seen in older age groups. Similarly, in other studies malignant GOO was attributed to elder age group [1,2,6]. In a series of Fisher et al,18 average age was 54yrs for Ca PA and male to female ratio was 2:1 which was similar to present study [8].
Table 6: Comparison of an etiology in various studies
| Cause | Present study (%) | Dogo d et al 2(%) | Ellis h et al 13(%) | Balint ja et al 14(%) |
| Carcinomapylorus | 38 | 15 | 30 | 11.02 |
| Cicatrized duodenal ulcer | 48 | 65.7 | 65 | 80,5 |
| Corrosive antral stricture | 8 | - | - | - |
| Others | 6 | 18.4 | 5 | 8.5 |
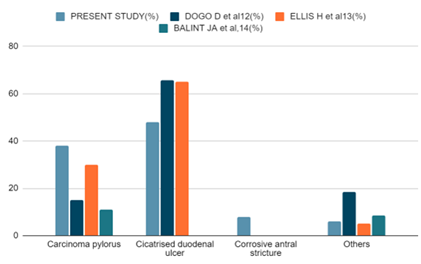
Figure 6
Higher incidence of GOO seen in males; this may be due to higher consumption of gastric irritants by them. GOO was occurred more in low socio-economic status population in present study similar to a study in North Eastern Ethiopia [4].
Table 7: Incidence of symptoms in cicatrized duodenal ulcer patients.
| Symptoms | Present study (%) | Yogiram betal,19(%) | Weiland d et al,23(%) |
| Abdominal pain | 90 | 87 | 86 |
| Vomiting | 100 | 80 | 91 |
| Loss of weight | 62 | 69.2 | 52 |
| Loss of appetite | 82 | 84 | - |
| Constipation | - | 23 | - |
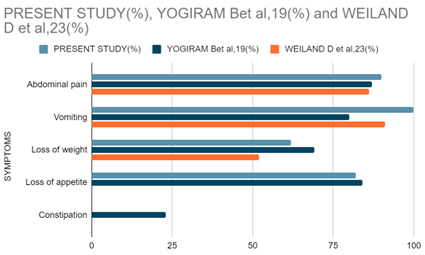
Figure 7
60% of patients were smokers and 50% of them had a history of alcohol consumption in this study which is somewhat similar to another study by Kozoll et al [10]. Most common symptom of GOO was non bilious vomiting, which was seen in 100% of the cases which is similar to other studies (Table 7) [2-4]. Weight loss was noted in 59.5% of patients in series of Kozoll DD et al, and 32% in series of Dworken HJ et al, suggesting weight loss was significant in patients with pyloric obstruction [10,11]. In Ca PA cases major symptom was vomiting, seen in 100% patients, followed by loss of weight (89.47%) and loss of appetite (89.47%). Significant weight loss in this study suggests the long-standing nature of the disease. Pallor was noted in 66% of patients. Majority (89.47%) of patients with Ca PA were anemic probably due to decreased intake and microscopic blood loss and cancer cachexia. Epigastric mass was palpable in 73.68% patients of Ca PA. Patients with carcinoma pyloric antrum had ‘A’ blood group as major blood group (47.37%). Blood group ‘O’ was the major (52.63%) group encountered in patients with cicatrizing DU. Persons with ‘O’ blood group are about three times more likely to develop acid peptic disease, signified by this study.
Upper gastrointestinal scopy was done in all cases compulsory. All patients with duodenal ulcer sequelae showed features of GOO. 7 patients with Ca PA showed fungating growth in antrum and 11 patients had prepyloric ulcer/growth. 4 patients had corrosive acid poisoning, in which Antral strictures were found. Patients with carcinoma head of pancreas and carcinoma gall bladder showed the feature of duodenal compression. 2 patients with corrosive acid poisoning had esophageal stricture, hence scope could not be passed beyond. In 1 patient of corrosive esophageal stricture, Barium meal was performed as OGD could not be passed beyond stricture. In 52.63% of patients with Ca PA, Anterior GJ was done as a palliative bypass procedure as the tumor was inoperable. A total of 26.31% patients of Ca PA underwent Billroth II gastrectomy. 3 patients underwent feeding jejunostomy out of 19 patients of Ca PA. Truncal vagotomy with posterior GJ was done in all the patients of cicatrized DU. Three patients had associated gallstone disease; cholecystectomy was done in these patients additionally.
One patient with corrosive antral stricture underwent antrectomy with coloplasty and feeding jejunostomy Antrectomy with Billroth II anastomosis was done in three patients with corrosive antral strictures. 2 patients of carcinoma head of pancreas underwent triple bypass procedure. One Patient with a carcinoma gall bladder underwent anterior gastrojejunostomy. Gastrojejunostomy (GJ) was the most common type of procedure done in our study which is similar to other studies [8,10]. All patients had Ryle's tube in situ post operatively for continuous drainage of gastric contents. Ryle’s tube was removed on the 5th postoperative day and oral fluids started. Later on, the patient gradually changed to a solid diet. All the patients of carcinoma stomach, carcinoma head of pancreas and carcinoma gallbladder were referred to the Department of Medical Oncology for further therapy.
Few patients encountered post operative complications. No immediate post-operative mortality was seen in our study. One patient who underwent coloplasty came with stricture at the site of anastomosis in the neck, endoscopic dilatation was done in that patient. Dumping syndrome was seen in 4 patients who underwent Truncal Vagotomy and Posterior GJ, patients were advised diet therapy. Three patients who underwent Billroth II gastrectomy came with complaints of biliary gastritis, who were managed with bile chelating agents.
Conclusion
Commonest cause for GOO in current study found to be cicatrized DU. Increasing incidence of Ca PA was seen in present study. This may be due to better management of DU at an early stage. In 3rd world countries, incidence of carcinoma increased may be due to changing dietary habits and environmental factors.
References
- Samad AB, Whanzada TW, Shoukat IM. (2007). Gastric outlet obstruction: change in etiology. Pak J Surg, 23(1):29-32.
Publisher | Google Scholor - Appasani S, Kochhar S, Nagi B, Gupta V, Kochhar R. (2012). Benign gastric outlet obstruction–spectrum and management. Tropical Gastroenterol, 32(4):259-266.
Publisher | Google Scholor - Ashwin K et al. (2018). A Clinical Study of Gastric Outlet Obstruction. Int Surg J, 5(12):3913-3918.
Publisher | Google Scholor - International Surgery Journal (2018), 5(12):3917
Publisher | Google Scholor - Tendler DA. (2002). Malignant gastric outlet obstruction: Bridging another divide. Am J Gastroenterol, 97:4-6.
Publisher | Google Scholor - Kotisso R. (2000). Gastric outlet obstruction in Northwestern Ethiopia. East Centre Africa J Surg, 5(2):25-29
Publisher | Google Scholor - Broderick JT, Mathews JB. (2007). Ulcer complications: Zinner MJ, Ashley SW. Maingot’s Abdominal Operations. 11th ed. New York: McGraw Hill, 365.
Publisher | Google Scholor - Shone DN, Nikoomanesh P, Smith-Meek MM, Bender JS. (1995). Malignancy is the most common cause of gastric outlet obstruction in the era of H2 blockers. Am J Gastroenterol, 90(10):1769-1770.
Publisher | Google Scholor - Primrose JN. (2008). Stomach and duodenum. In Williams NS, Bulstrode CJK, O’Connell PR. Bailey and Love’s short practice of surgery. 25th ed. London (uk): Arnold Publisher, 1045-1079.
Publisher | Google Scholor - Ellis H, Nyhus LM, Wastell C. (1986). Surgery of Stomach and Duodenum, 4th ed, Little Brown Publications, Boston, 475.
Publisher | Google Scholor - Balint JA, Spence MP. (1959). Pyloric stenosis. Br Med J, 1(5126):890.
Publisher | Google Scholor - Kozoll DD, Meyer KA. (1964). Obstructing gastro duodenal ulcer, symptoms and signs. Arch Surg.
Publisher | Google Scholor - Dworken HJ, Roth HP. (1962). Pyloric obstruction associated with peptic ulcer: a clinicopathological analysis of 158 surgically treated cases. JAMA, 180(12):1007-1010
Publisher | Google Scholor













