

Case Report
A Case Report of MELAS Syndrome in a 7-year-old Girl Presented with Neurological Manifestations at Northwest General Hospital and Research Centre, Peshawar, Pakistan
- Moula Ghulam
- Mubashir Akbar
- Imran Khan
- Nouman Anthony *
- Talha Idrees
- Sajid Ali
General Medicine, Rehman Medical Institute, Peshawar, Pakistan.
*Corresponding Author: Nouman Anthony, General Medicine, Rehman Medical Institute, Peshawar, Pakistan.
Citation: Ghulam M, Akbar M, Khan I, Anthony N, Idrees T, et al. (2023). A Case Report of MELAS Syndrome in a 7-year-old Girl Presented with Neurological Manifestations at Northwest General Hospital and Research Centre, Peshawar, Pakistan. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 2(3):1-4. DOI: 10.59657/2992-9989.brs.23.018
Copyright: © 2023 Nouman Anthony, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 13, 2023 | Accepted: November 27, 2023 | Published: December 26, 2023
Abstract
MELAS is a mitochondrial disorder called mitochondrial encephalomyopathy, lactic acidosis, and stroke-like events that largely affect the muscles and neurological system. MELAS manifests in children or young adults as repeated episodes of localized neurological impairments, headache, myopathy, and encephalopathy. We present a case of 7-year-old patient presented with epilepsy, recurrent vomiting and reduced vision for over a year. She underwent routine blood sampling which showed high lactic acid, high serum potassium and high ALP. After which a CT brain was conducted showing atrophied areas of brain along with ventricular dilation. Therefore, a diagnosis of MELAS syndrome was made and was treated accordingly.
Keywords: melas syndrome; neurological manifestation; neurological impairment; headache; myopathy; encephalopathy
Introduction
MELAS is a mitochondrial disorder called mitochondrial encephalomyopathy, lactic acidosis, and stroke-like events that largely affect the muscles and neurological system. MELAS manifests in children or young adults as repeated episodes of localized neurological impairments, headache, myopathy, and encephalopathy [1]. MELAS is a hereditary condition that affects the mitochondria. Only the tail of the sperm contains paternal mitochondria, therefore, they are lost during fertilization, and mitochondrial diseases like MELAS are passed down through the mother [1]. By adolescence or early adulthood, neurological damage has set in due to the condition’s relentless progression [2].
Even if Genetic testing comes out to be inconclusive, current guidelines do not encourage invasive testing, such as skeletal muscle biopsy [2]. Rarely, random mutations without a family history might cause MELAS. These mutations affect the mitochondrial functions, particularly oxidative phosphorylation and energy production leading to mitochondrial genetic diseases. A frequent m.3243A> G mutation in the mitochondrial tRNALeu (UUR) (MTTL1) gene is present in more than 80% of MELAS cases [3]. The disruption of protein assembly into respiratory chain complexes is thought to result from tRNA mutations in MELAS, while the precise mechanisms are still unknown. Mitochondria are their powerhouses and any mitochondrial dysfunction will have an impact on the body most metabolically active organs, including the muscles and brain [4]. Although the exact cause of the stroke-like episodes in MELAS is still unknown, recent research has suggested that endothelial cell mitochondrial failure may be the cause of small vessel angiopathy [5]. This disorder is among the most difficult to diagnose because it is uncommon and has a complicated clinical appearance. It is particularly challenging to distinguish between MELAS and an ischemic stroke [6]. Despite their widespread prevalence, they are still frequently underdiagnosed particularly in low- and middle-income nations like Pakistan [7].
History
This 7-year-old girl from Afghanistan presented to our OPD with complaints of bilaterally reduced vision and seizures for the last 1 year. The reduction in vision was sudden in nature with only light perception at the time of presentation to OPD. She had an episode of epilepsy 1 year ago and ever since she was repeatedly hospitalized for epilepsy in her hometown. Each episode would last for 20 minutes followed with loss of consciousness, eye rolling, and frothiness however there was no faecal or urinary incontinence. She also complained of increased frequency of recurrent vomiting for the last 1 year. Her home medication included Epival and clonazepam citrate which she failed to take regularly. Further Laboratory investigations were conducted and mainly all were normal except for Lactate= 69, ALP=240, potassium=4.7. On the basis of presenting sign and symptoms along with increased lactate levels a provisional diagnosis of MELAS syndrome was made. To further confirm the underlying pathology a CT brain was conducted showing bilateral occipital lobe infarcts with brain atrophy and dilated ventricles. She was started on Ascard, CAP and Lerrace, Hepa-Merz, Lysovit. She had a significant neonatal history of ingestion of unknown and unprescribed drugs by her mother during pregnancy. She was advised to continue the medications and review in 1 months’ time.
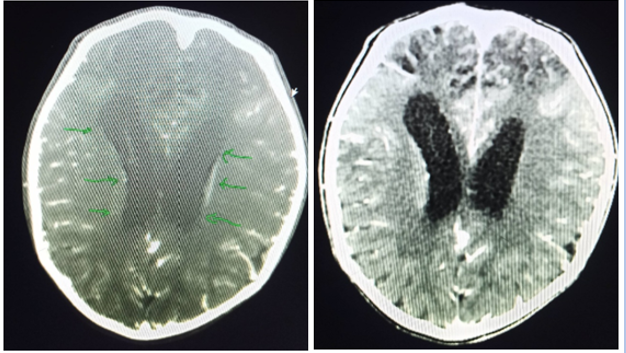
Figure 1
Discussion
The patient in the current case report had an epileptiform seizure, altered consciousness, hemianopsia, and blurred vision. These signs and symptoms mimicked MELAS syndrome’s clinical features. MELAS syndrome, which stands for mitochondrial encephalopathy, lactic acidosis, and stroke-like events, is an uncommon condition that typically manifests between the ages of two and fifteen and mostly affects the neurological system and muscles. Typical manifestations of MELAS syndrome include seizures, recurring headaches, loss of appetite, and recurrent vomiting which were similar to the sign and symptoms of present case [8]. Hemiparesis, a condition similar to a stroke that causes temporary muscle weakness on one side of the body, can cause altered states of consciousness, vision and hearing loss, loss of motor abilities, and intellectual incapacity [9]. MELAS is brought on by mitochondrial DNA mutations, and in certain individuals, POLG1 nuclear gene abnormalities have also been linked to this condition [10]. Due to its very variable geno type, complex, varied, and non-specific clinical symptoms MELAS is frequently misdiagnosed. Early detection and prompt treatment, therefore, help to slow the course of the disease and enhance prognosis. The differential diagnosis for MELAS is important as many of its symptoms overlap with Cerebral Hemiatrophy and Leigh syndrome [11,12]. Laboratory assays in the presented case resulted in raised lactate, which when correlated clinically suggests MELAS syndrome as shown in many reported casses of MELAS syndrome. False-negative results are possible if blood molecular investigations do not find any causal pathogenic variations. Extensive testing on other tissues, such as skin fibroblasts or muscle, can be thought about if clinical suspicion is still strong [13].
The disease frequently targets and primarily involves the temporal, parietal, occipital and the basal ganglia region, which typically only affects cortical and subcortical white matter and exhibits gyriform abnormalities signal shadow [14]. The ingestion of unsupervised and un-prescribed drugs by the mother also poses a potential threat to the fetus of growing mitochondrial defects [15]. MELAS requires multi-specialist intervention once it has been diagnosed. Treatments focus on maintaining mitochondrial function through vitamin and antioxidant supplementation, preventing acute neurological deterioration (rapid loss of consciousness without apparent cause, for instance in stroke-like episodes), treating progressive neurodegeneration, preventing convulsions, and managing symptoms [5]. To track the development and the emergence of new symptoms, affected people and their at-risk families should be on surveillance on a frequent basis. It is advised to have an annual examination of their eyes, ears, and heart (including an electrocardiogram and echocardiography). Additionally, such patients are advised for annual urinalyses and fasting blood glucose levels. Mitochondrial toxins such as alcohol, tobacco, antibiotics i.e., linezolid, aminoglycoside, valproic acid, metformin because of the potential for lactic acidosis, and dichloroacetate (DCA) because of the potential for peripheral neuropathy shall be avoided during gestation [2].
Conclusion
MELAS syndrome, which stands for mitochondrial encephalopathy, lactic acidosis, and stroke-like events, is an uncommon condition that typically manifests between the ages of two and fifteen and mostly affects the neurological system and muscles. Early diagnosis of MELAS syndrome yet remains a challenge in developing and under developed countries therefore more focused observation is necessary for patients presenting with such sign and symptoms along with lactic acidosis and neurological defects on imaging. There is also a need of further studies on the condition.
References
- Pia S & Lui F. (2020). Melas Syndrome. Bethesda: Treasure Island (FL): StatPearls Publishing.
Publisher | Google Scholor - El-Hattab A. W, Almannai M & Scaglia F. (2018). MELAS. In A. W. El-Hattab, M. Almannai, & F. Scaglia, Gene Reviews. Seattle: University of Washington.
Publisher | Google Scholor - Ikeda T, Osaka H, Shimbo H, Tajika M, Yamazaki M, Ueda A, . . . Yamagata T. (2018). Mitochondrial DNA 3243A & gt; T mutation in a patient with MELAS syndrome. Human Genome Variation.
Publisher | Google Scholor - Wang S, Song T & Wang, S. (2020). Mitochondrial DNA 10158T > C mutation in a patient with mitochondrial encephalomyopathy with lactic acidosis, and stroke-like episodes syndrome. Medicine (Baltimore), 20310.
Publisher | Google Scholor - Sunde K, Blackburn P. R, Cheema A, Gass J, Jackson J, Macklin S & Atwal P. S. (2016). Case report: 5year follow-up of adult late-onset mitochondrial encephalomyopathy with lactic acid and stroke-like episodes (MELAS). Molecular Genetics and Metabolism Reports, 94-97.
Publisher | Google Scholor - Khandwala K, Ahmad A & Sheikh T. (2018). MELAS: A complex and challenging diagnosis. Journal of the College of Physicians and Surgeons, 46-48.
Publisher | Google Scholor - Hettiarachchi D, Lakmal K & Dissanayake V. (2022). Mitochondrial diseases in South Asia – A systematic review. Mitochondrion, 24-30.
Publisher | Google Scholor - El-Hattab A. W, Adesina A. M, Jones, J & Scaglia, F. (2015). MELAS syndrome: Clinical manifestations, pathogenesis, and treatment options. Molecular Genetics and Metabolism, 4-12.
Publisher | Google Scholor - Vandanaa V. P, Bindu P. S, Sonam K, Govindaraj P, B. Taly A, Gayathri N, . . .Thangaraj K. (2016). Audiological manifestations in mitochondrial encephalomyopathy lactic acidosis and stroke like episodes (MELAS) syndrome. Clinical Neurology and Neurosurgery, 17-21.
Publisher | Google Scholor - Chakrabarty S, Govindaraj P, Sankaran B. P, Nagappa M, Kabekkodu S. P, Jayaram P, . . . Meena A. K. (2021). Contribution of nuclear and mitochondrial gene mutations in mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome. Journal of Neurology, 2192-2207.
Publisher | Google Scholor - Wei Y, Huang Y, Yang Y & Qian M. (2021). MELAS/LS Overlap Syndrome Associated with Mitochondrial DNA Mutations: Clinical, Genetic, and Radiological Studies. Frontiers in Neurology.
Publisher | Google Scholor - U U. F, C E. J.-K, Mathieu, M, N O. P, Ongolo C, P & W M. (2013). Differential Diagnoses of Cerebral Hemiatrophy in Childhood: A Review of Literature with Illustrative Report of Two Cases. Global Journal of Health Science, 195-207.
Publisher | Google Scholor - Sumit Parikh A. G, Saneto R, Anselm I, Cohen B. H, Falk M. J, Greene C, . . .Tarnopo M. (2015). Diagnosis and management of mitochondrial disease: a consensus statement from the Mitochondrial Medicine Society. Genetics in Medicine volume, 689-701.
Publisher | Google Scholor - Tzoulis C & Bindoff L. A. (2009). Serial Diffusion Imaging in a Case of Mitochondrial Encephalomyopathy, Lactic Acidosis, and Stroke-Like Episodes. AHA Journals, 14-17.
Publisher | Google Scholor - Morén C, Hernández S, Guitart-Mampel M & Garrabou G. (2014). Mitochondrial Toxicity in Human Pregnancy: An Update on Clinical and Experimental Approaches in the Last 10 Years. International Journal of Environmental Research and Public Health, 9897-9918.
Publisher | Google Scholor













