

Research Article
Treatment Outcome and Associated Factors Among Severely Malnourished Under-five Children Admitted to Zewditu Hospital October, 2023
- Tsion Seife Adere 1**
- Tewodros Kassahun Tarekegn 1*
- Kirubel Tesfaye Hailu 2
- Michael Yefrashowa Betemariam 1
- Hamlet Mulu Aberha 1
- Feven Negasi Abriha 2
- Buure Ayderuss Hassen 1
- Birukti Gebreyohannes Habtezgi 1
- Rediet Habtu Lebelo 3
- Helen Assefa Berhe 4
- Solomon Endale Dagnachew 1
- Surafel Alemayehu Tsegaye 5
1Department of Medicine, Hayat Medical College, Addis Ababa, Ethiopia.
2Department of Medicine Jimma University Oromia Region, Ethiopia
3Department of Medicine, Mekelle University, College of Health Science, Mekelle. Ethiopia
4Department of Medicine, Addis Ababa University, Tikurs Anbessa, College of Health Sciences, Ethiopia.
5MPH Candidate at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, USA.
*Corresponding Author: Tewodros Kassahun Tarekegn, Department of Medicine, Hayat Medical College, Addis Ababa, Ethiopia.
Citation: Tsion S. Adere, Tewodros K. Tarekegn, Kirubel T. Hailu, Michael Y. Betemariam, Hamlet M. Aberha, et al. (2024). Treatment Outcome and Associated Factors Among Severely Malnourished Under-five Children Admitted to Zewditu Hospital October, 2023, International Journal of Nutrition Research and Health, BioRes Scientia Publishers. 3(1):1-12. DOI: 10.59657/2871-6021.brs.24.010
Copyright: © 2024 Tewodros Kassahun Tarekegn, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 07, 2023 | Accepted: December 29, 2023 | Published: January 05, 2024
Abstract
Background: Severe acute malnutrition (SAM) remains a major contributor to under-five mortality globally. In Ethiopia, the 2019 Demographic and Health Survey showed a SAM prevalence of 1% among children under 5 years of age. Objectives: To assess treatment outcomes and factors associated with nutritional recovery among children admitted for SAM at Zewditu Hospital, Addis Ababa, Ethiopia.
Methods: A cross-sectional study was conducted through retrospective review of 409 medical records of children <5 years admitted for SAM from July 2021 to June 2022. Nutritional recovery was compared across demographic and clinical factors using binary logistic regression analysis. Results: The recovery rate was 65.2%, below the minimum international standard of >75%. Age <24 months (AOR 0.24, 95% CI 0.28-0.67), female gender (AOR 0.37, 95% CI 0.27-0.53), lack of breastfeeding (AOR 3.4, 95% CI 1.40-4.30), pneumonia (AOR 0.35, 95% CI 0.17-1.08), and diarrhea (AOR 0.475, 95% CI 0.31-1.15) were associated with lower likelihood of nutritional recovery.
Conclusion: Suboptimal recovery rates and associated factors like young age, gender disparities, breastfeeding gaps, and co-morbidities underscore the need to improve quality and equity of care through context-specific interventions engaging communities and health workers. Addressing broader socioeconomic and health systems determinants will also be key.
Recommendations: Targeted programmed ought to priorities the early identification and treatment of SAM in children under two years old, the promotion of optimal breastfeeding, integrated disease management, and specialized interventions that address gaps in the health systems and sociocultural barriers.
Keywords: severe acute malnutrition; treatment outcome; risk factors; under-five mortality; ethiopia
Keywords: severe acute malnutrition; treatment outcome; risk factors; under-five mortality; ethiopia
Introduction
Severe malnutrition is defined as a very low weight for height/length (< 3> 6 months or a weight-for-height < − 3 z-scores according to WHO’s growth standards for under-five children; and nutritional edema with kwashiorkor; that is, the presence of clinically confirmed bilateral, pitting edema. Acute malnutrition is a major challenge for achieving sustainable development goals (e.g., Goals 2 and 3–Zero Hunger and Good Health and Wellbeing) as it is associated with major causes of under-five mortality [2].
Malnutrition leads to adverse maternal and child health consequences including retarded school performance and aggravating maternal related problems especially in poorer settings. For instance, 2% of children (nearly 13 million) suffer from SAM in developing countries of which over 90% live in South- East Asia and sub-Saharan Africa. Indeed, SAM is a common indication for pediatrics hospital admission and inpatient treatment in these countries. Thus, mortality of children from SAM in inpatient set-ups in sub-Saharan Africa still remains significantly high, with ten-folds higher the risk of death than well-nourished children [3].
Statement Of the problem
Across the globe, an estimated 16 million children under the age of 5 are affected by severe acute malnutrition. This number is staggering, most importantly because children with severe acute malnutrition are nine times more likely to die than well-nourished children. Severe acute malnutrition is a major cause of death in children under five, and its prevention and treatment are critical to child survival and development [4]. Based on the 2019 Ethiopia Demographic Health Survey (EDHS), 7% of children under five are wasted, and 1% of these are severely wasted. Mortality remains high among children with severe acute malnutrition, who often die because of several factors such as associated childhood co-morbidities, e.g., diarrhea, pneumonia, shock, and non-adherence to management protocols by health care professionals. Among the children, 66 (12.52%) were dead, and 357 (67.7%) were recovered at the end of follow-up [5].
Acute malnutrition is linked to higher risk of morbidity and mortality. It is also linked to poor growth and development, which contributes to stunting when episodes are persistent or frequent. A longitudinal study at Jima University Medical Center conducted to estimate the incidence rate of hospital-acquired infection revealed that a prolonged hospital stay (6.3 more days) was associated with hospital-acquired infection [6]. As confirmed by consecutive EDHS results, there is a decline in stunting, underweight, and wasting in children under five years of age. However, a stunting rate of 38% remains a great concern with the subsequent life-course impact of malnutrition on the long-term health of individuals and the socioeconomic development of the nation. There is a regional variation in malnutrition ranging from 15% in Addis Ababa to 46% in Amhara; seven of the regions have a rate greater than 30%, and the rate in Tigray was found to be 39%, which exceeded the national average. The national levels of wasting and underweight in children under five years of age were 10% and 24%, respectively, and in Tigray, 11% and 23%, respectively [7].
Significance of study
Ethiopia has a long history of food insecurity and nutritional problems, which have afflicted a substantial section of the population as a result of repeated droughts. Despite many initiatives to address the issue, there is no more explicit data on children’s treatment outcomes. Moreover, given the reality that Addis Ababa is the capital city of Ethiopia and has better infrastructure and supply than the rest of the region, the prevalence of SAM is expected to be lower and management to be better, but still, there is a high prevalence of malnutrition in Addis Ababa, despite the availability of treatment for children with SAM in hospitals and health centers by TFU (Therapeutic feeding unit) and OTP (Outpatient Therapeutic care Programs). So, this study aimed to assess the treatment outcomes of already managed severely malnourished children and determined the contextual factors of treatment outcome in Zewditu hospital in Addis Ababa. In addition, this study covers a wider range of target populations, which can represent public hospitals in Addis Ababa.
Literature Review
overview of malnutrition worldwide
According to a study done in India, Malnutrition attributes to 33% of global deaths and 45% of deaths in under-five children in South Asia and Sub-Saharan Africa. In India, nearly 57 million children are moderate to severely malnourished and account for more than 50% of deaths in the 0-4 years age group. Moreover, 48% of under-five children are stunted due to severe malnutrition.8 Severe acute malnutrition (SAM) is managed as per the 10 steps of standardized inpatient treatment as per the 2016 modification of guidelines [8]. The ready-to-use therapeutic foods F-75 and F-100 have increased the feasibility of community management. Despite this standardized protocol of care, in-patient mortality is as high as10%-40%, and the reasons are yet to be elucidated. It might be due to various co-morbidities associated with SAM children, improper adherence to the treatment protocol, defective management, and other socio-demographic causes. In India, more than 33% of deaths under five years of age are associated with malnutrition. This might be due to change in innate and adaptive immunity as a result of nutrient and micronutrient deficiencies. Besides these, associated co-morbidities like anemia, diarrhea, dehydration, hypoglycemia, hypothermia, electrolyte imbalance, and sepsis play a major role in increased mortality [9].
Overview of malnutrition in Africa
According to studies done in Nigeria, although there is a standard protocol for the management of SAM in children, case-fatality rates in hospitals remain unacceptably high at between 30% and 50%, especially in children with co-morbidities and medical complications including infections, diarrhea, shock, and anemia. In Southeast Nigeria, the mortality rate in a tertiary hospital for children with protein-energy malnutrition was 40.1%. A community house-to-house survey carried over two decades ago in Cross River State, Nigeria among 471 total deaths over a one-year period of children under five years of age showed protein-energy malnutrition accounted for 11% of the mortality. The Nigerian Demographic and Health Survey (NDHS) of 2018 showed that 37% of children under five years of age are stunted and 7% are wasted. Most studies on SAM in Nigeria focused on disease burden without evaluating risk factors, which may be useful in reducing mortality in hospitalized children with SAM [10].
A study done in Mozambique stated that Childhood acute malnutrition is a global health problem and life-threatening condition. Acute malnutrition is caused by complex and intertwined factors with large, time and geographic variability. Globally, acute malnutrition still affects 50.5 million children under 5 years old and those ‘who are moderately or severely wasted have higher risk of mortality’ and ‘more likely to become stunted’. Wasted children are more likely to be living in low- and middle-income countries, such as Mozambique, with many health inequalities [11].
According to studies done Uganda, In 2015, out of the thirty-three countries that accounted for 90 % of the global burden of malnutrition, twenty-two were from Africa. In Uganda, 14 % of children are severely stunted, 2 % are severely wasted and 3 % are severely underweight.
In Gulu, there is an SAM prevalence of 0·7% (0·3-1·1 %). Globally, SAM accounts for >1/3–0·5 of all deaths in children under 5-years and approximately 54 percentage deaths in developing countries. The minimum international standard set for the management of SAM is a case fatality rate (CFR) less than 10 % [12].
Overview of malnutrition in Ethiopia
A study done in western Ethiopia, The latest Ethiopia Mini Demography and Health Survey stated that stunting, wasting, and underweight among under-five children in Ethiopia are 40%, 9%, and 25%, respectively, and this figure is very high compared to national figure in Somali region (38.4%, 27.0%, and 38.8%), respectively. This study therefore aimed at determining the treatment outcome and the predictors of poor treatment response among undernourished children admitted to Nekemte Referral Hospital where there is paucity of this important data. The findings of this study intend to further aid clinicians to improve the outcome of these children [13]
A study done in Guji stated that, Ethiopia would only reach the millennium development goal target of halving the number of underweight children if the reduction percentage is increased to at least 1.6 percentage per year but failed. Under the umbrella of growth and transformation plan 2, the government of Ethiopia launched Health sector transformation plan which gives due considerations for nutrition than the previous other plans for reduction of prevalence of wasting from11 to 3% [14].
According to studies done in wollo zone, Inpatient therapeutic feeding units faced with a lot of challenges in handling of cases of acute malnutrition. Some of the challenges include limited in-patient capacity, lack of enough skilled staff in the hospitals to threat large number of needing care, the centralized nature of Hospitals promotes late presentations and high costs of treatment, increased risk of cross infection for immune suppressed children such as with SAM [15]
According to research done in North West Ethiopia, in Ethiopia; SAM was the third leading cause of mortality accounting for 8.1% of under-five children deaths. This might be due to immune compromission from complex, adaptive physiologic and metabolic processes secondary to insufficient nutrients. Underlying and/or concurrent medical conditions including dehydration, anemia, sepsis, hypoglycemia and hypothermia might also contributes to this high death toll. Prognosis for SAM treatment continues to be a challenge and better outcomes for inpatient interventions still remains low due to co-morbidity, poor adherence to treatment guideline, mismanagement of cases and other socio-demographic factors. As a result, health sector has upgraded nutritional interventions through the health promotion, effective treatment strategy and supplementation of essential micronutrients for children and mothers [16].
A study done in Felege Hiwot Hospital states that Ethiopia is one of the most countries in sub saran Africa with the highest rates of Severe acute malnutrition. Over the past fifteen years, the trends of malnutrition reviled that there is a reduction in stunting by 31% and underweight by 39%. However, there was only a small decline in the prevalence of wasting over the last 15 years (from 12 to 9%). In Ethiopia 3% of under five children have SAM and 2.7% are found in Amhara region. In Bahir Dar town, among all malnourished under five year children, 24.8% of them are due to SAM [17].
The latest Ethiopia Mini Demography and Health Survey stated that stunting, wasting, and underweight among under-five children in Ethiopia are 40%, 9%, and 25%, respectively, and this figure is very high compared to national figure in Somali region (38.4%, 27.0%, and 38.8%), respectively [14]. This study therefore aimed at determining the treatment outcome and the predictors of poor treatment response among undernourished children admitted to Nekemte Referral Hospital where there is paucity of this important data. The findings of this study intend to further aid clinicians to improve the outcome of these children [18].
Conceptual frame work
This conceptual frame work was developed by reviewing literatures, relevant and updated researches on related subject matters then by selecting the important variables on the treatment outcomes among severely malnourished children [17].
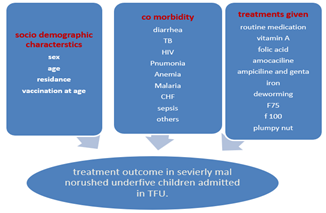
Figure 1: Conceptual frame work which explains the relationship between treatment outcome and factors that might have influence on the treatment outcomes among under five children admitted in Zewditu Hospital, 2022.
Objectives
General Objective
To assess the treatment outcome and associated factors cases among severely malnourished under-five children admitted to Zewditu hospital from July 2021 to Jun 2023.
Specific Objectives
To determine the treatment outcome among severely malnourished under-five children admitted to Zewditu hospital from July 2021 to Jun 2023. To identify factors associated with treatment outcome among severely malnourished under-five children admitted to Zewditu hospital from July 2021 to Jun 2023.
Methods and Materials
Study area
Zewditu Hospital is a public hospital in Addis Ababa, Ethiopia. It was built, owned and operated by the Seventh-day Adventist church, but was nationalized during the Derg regime in about 1976. The hospital is named after Empress Zewditu, the cousin and predecessor on the throne of Emperor Haile Selassie. Today Zewditu hospital is operated by the minister of Health. Located at Taitu st, Kirkos sub city, Addis Abeba 9˚1’6’’N 38˚45’22’’E.
Study design
A hospital based cross-sectional study using a retrospective record review was conducted from September 25 to 25 October, 2023.
Population
Source population
The source of population was all under five severely malnourished children who were admitted and treated at inpatient therapeutic feeding units in Zewditu Memorial hospital.
Study population
All under five severely malnourished children who were admitted and treated at inpatient therapeutic feeding units in Zewditu Memorial hospital during the study period.
Sample population
All randomly selected under five severely malnourished children who were admitted and treated at inpatient therapeutic feeding units in Zewditu Memorial hospital during the study period.
Inclusion and Exclusion criteria
Inclusion criteria
All under five severely malnourished children who were admitted and treated at inpatient therapeutic feeding units in Zewditu Memorial hospital during the study period.
Exclusion criteria
Children who are re-admitted children who are treated as an outpatient will be excluded from the study.
Sampling size determination and sampling technique
Sampling size determination
The required sample size is calculated using single population formula with following assumptions. 95% confidence interval, 5% margin of error, p=58.4% proportion of occurrence of cure rate (recovery rate). The proportion is taken from a study conducted in Bahir Dar Felege Hiwot referral Hospital, where the recovery outcome is lowest and we get the maximum sample size. By 10% non-respondent rate, the final sample size will be

Add 10% non-response rate; the total sample size will be 409.
Add 10% non-response rate; the total sample size will be 409.
The data was collected by reviewing records from impatient therapeutic feeding registration book and individual follow-up chart using pre tested data collection form. Data’s of under-five severely malnourished children who were admitted from July 2021 to Jun 2023 will be reviewed. Data was collected by using systemic random sampling after calculating the Kth value. (N=982/n=409 which gives ask value of 2). Where the first participant was selected using lottery method from 1-2 and every second child was enrolled until calculated sample size was reached.
Variables
Dependent variable
Treatment outcome
Independent variable
Socio demographic characteristics
Co-morbidity patterns
Treatments and feedings given for the admitted children with SAM
Operational definitions
Recovery- was considers when the admitted children with weight less than 70
Results
Socio-demographic characteristics of subject records
The table shows that the population is divided into two age groups. Approximately 130 people (32%) of the 409 participants are under the age of 24 months, while the remaining 68% (279 people) are between the ages of 24 months and 5 years. Examining the sex distribution within the studied population, the table indicates that out of the 409 participants, approximately 180 individuals (44%) are male, while the remaining 229 individuals (56%) are female. The near-equal split between males and females ensures that gender-specific factors can be adequately considered when studying health outcomes and designing targeted interventions.
Table 1: socio-demographic characteristics
| Variable | categories | Frequency | percentage |
| Age | <24mon> | 130 | 32 |
| 24mon – 5yrs | 279 | 68 | |
| Sex | Male | 180 | 44 |
| Female | 229 | 56 | |
| Place of residence | Urban | 190 | 46.5 |
| Rural | 219 | 53.5 | |
| Breast feeding | Yes | 192 | 47 |
| No | 217 | 53 | |
| Vaccinated for Age | Unvaccinated | 53 | 12.8 |
| Partial Vaccinated | 199 | 48.7 | |
| Fully Vaccinated | 157 | 38.5 |
Co-morbidities of SAM patients
Among the 409 participants, 361 individuals (88.4%) did not report experiencing diarrhea, while the remaining 48 individuals (11.6%) reported having had diarrhea. This relatively low prevalence suggests that diarrhea may not be a significant health concern within the study population. However, it is essential to consider potential contributing factors, such as access to clean water, sanitation practices, and nutritional status, which can influence the incidence of diarrhea. The data indicates that TB, HIV, and pneumonia were relatively less prevalent among the study participants. Only 13 individuals (3.1%) reported having TB, 16 individuals (3.8%) reported being HIV-positive, and 36 individuals (8.7%) reported having pneumonia. The data reveals that 180 individuals (44.1%) of the participants reported having sepsis, indicating a relatively high prevalence within the study population. In contrast, the prevalence of malaria was exceptionally low, with only 1 individual (0.2%) reporting the condition. Similarly, URTI was reported by only 20 individuals (4.8%) of the participants, indicating a relatively low occurrence compared to other health conditions. The data shows that anemia was relatively prevalent within the study population, with 300 individuals (73.4%) reporting the condition. Regarding malnutrition, marasmus was reported by 334 individuals (81.7%), while kwashiorkor was reported by 13 individuals (17.4%). Additionally, 62 individuals (15.2%) reported having marasmic-kwashiorkor.
Table 2: Co-morbidities of SAM patients
| Variables | Categories | Frequency | Percentage |
| Diarrhea | Yes | 361 | 88.4 |
| No | 48 | 11.6 | |
| TB | Yes | 13 | 3.1 |
| No | 396 | 96.2 | |
| HIV | Yes | 16 | 3.8 |
| No | 393 | 96.2 | |
| Pneumonia | Yes | 373 | 91.3 |
| No | 36 | 8.7 | |
| Sepsis | Yes | 180 | 44.1 |
| NO | 229 | 55.9 | |
| Malaria | Yes | 1 | 0.2 |
| NO | 408 | 99..8 | |
| URTI | Yes | 389 | 95.2 |
| NO | 20 | 4..8 | |
| Anemia | Yes | 300 | 73.4 |
| NO | 109 | 26..6 | |
| Marasmus | Yes | 334 | 81.7 |
| No | 75 | 18.3 | |
| Kwashakor | Yes | 13 | 17.4 |
| NO | 396 | 82.6 | |
| Marasmc-kwash | Yes | 62 | 15.2 |
| NO | 347 | 84.8 |
Treatment outcome
The data reveals that 119 individuals (28.8%) of the participants were classified as "Unrecovered" based on the final treatment outcome. These individuals did not experience significant improvement in their health conditions despite undergoing treatment.
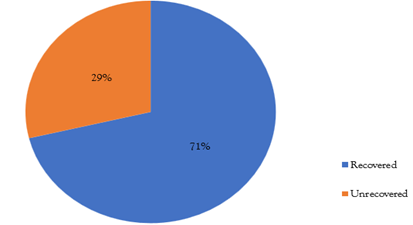
Figure 2: Treatment outcome of under-5 SAM patients admitted to ZMH in 2014
Factors associated with treatment outcome
This research investigated the relationships between treatment outcomes and age, sex, residence, breastfeeding status, immunisation status, diarrhoea, pneumonia, sepsis, anaemia, marasmus, and kwashiorkor.
The variables that demonstrated a statistically significant correlation with nutritional recovery were age, sex, breastfeeding, pneumonia, and diarrhoea. In particular, there was a decreased chance of recovery for those under 24 months old which is 130 individuals (32%) as opposed to those between 24 and 59 months old which is 279 individuals (68%) (AOR 0.24, 95% CI 0.28-0.67). Compared to 180 male patients (44%), 229 female patients (56%) had worse recovery odds (AOR 0.37, 95% CI 0.27-0.53). Compared to the 192 breastfed children (47%), 217 of the children who were not breastfed (53%) had a lower chance of recovering (AOR 3.4, 95% CI 1.40-4.30).
In comparison to individuals without these conditions, the likelihood of recovery was also decreased in 36 of those with pneumonia (8.7%) and 48 of those with diarrhoea (11.6%) (AOR 0.35, 95% CI 0.17-1.08 and AOR 0.475, 95% CI 0.31-1.15, respectively). There was no statistically significant correlation found between nutritional recovery and other factors, such as place of residence, vaccination status, sepsis, anaemia, marasmus, and kwashiorkor, in this study.
Table 3: Factors with significant association with nutritional recovery of SAM.
| Variable | Recovered frequency (%) | Not recovered frequency (%) | COR (95%CI) | AOR (95%CI) | |
| Age | <24> months | 62 (23) | 68 (48.5) | 0.31(0.12 - 0.56) | 0.24 (0.28 –0.67) |
| 24 months – 5 yrs | 207 (67) | 72 (51.5) | 1 | ||
| Sex | Female | 169(62.8) | 60 (42.8) | 0.41 (0.24 -0.70) | 0.37 (0.27- 0.53) |
| Male | 100(37.2) | 80 (57.2) | 1 | ||
| Pneumonia | Yes | 252(93.6) | 104 (74.2) | 0.478 (0.31 -0.73) | 0.35 (0.17–1.08) |
| No | 17 (6.4) | 36 (27.8) | 1 | ||
| Anemia | Yes | 203 (75.4) | 97 (69.2) | 1.36 (0.97-1.86) | 1.32 ( 0.31- 1.77) |
| No | 66 (24.6) | 43 (30.8) | 1 | ||
| Breast Feeding | Yes | 153 (56.8) | 39 (27.8) | 3.72 (2.89-3.92) | 3.4 (1.40– 4.30) |
| No | 116 (43.2) | 101 (72.2) | 1 | ||
| Diarrhea | Yes | 232 (86.2) | 129 (92.1) | 0.53 (0.40- 0.75) | 0.475 (0.31 – 1.15) |
| No | 37 (13.8) | 11 (7.9) | 1 | ||
Discussion
This study examined treatment outcomes and related factors for under-five severely malnourished patients admitted to Ethiopia's Zewditu Hospital. The main conclusions were that the recovery rate was only 65.2% overall, which is less than the minimum international standard of greater than 75% [19]. Nutritional recovery was significantly correlated with age, sex, breastfeeding status, pneumonia, and diarrhea. In contrast to comparable studies carried out in other regions of Ethiopia, including Woldia (85%) [20], Southern Ethiopia (82.4%) [21], and Jimma (77.8%) [22], the recovery rate in this study is lower. Suboptimal adherence to treatment protocols and a high default rate may be the cause of the lower recovery rate [23]. In contrast to results from Bahir Dar, Ethiopia (58.4%), the recovery rate was higher [24] This suggests that although there has been progress, the management of childhood SAM in the research setting still needs to be improved. Younger age (less than 24 months) was linked to a lower chance of recovery, which is consistent with another research [25] [26]. Higher infection risk, inadequate breastfeeding, and inadequate therapeutic feed preparation in this age group are among the potential causes [27]. For young SAM children, targeted interventions are required to enhance screening, referral, and treatment outcomes [28]. As in research from Bangladesh [29] and India [30], female sex was linked to worse outcomes for recovery. This emphasizes the necessity of gender-sensitive interventions that address gender biases and sociocultural factors when it comes to girl children seeking healthcare [31]. The gender gap in SAM recovery may be closed with the support of gender equality as well as equitable treatment access [32].
Lower recovery was predicted by not breastfeeding, which is in line with research demonstrating the protective effects of breastfeeding towards infections and mortality risk in malnourished children [33] [34]. Therefore, improving outcomes through career counseling could involve promoting optimal breastfeeding practices [35]. Consistent with other reports, co-morbidities such as pneumonia and diarrhea hampered the healing process [36] [37]. It is imperative to address childhood illnesses and SAM together in order to counteract the synergistic effect on mortality [38] Recuperation could be further improved by bolstering early infection treatment and prevention through nutrition promotion, immunization, and care access [39]. In general, a multisectoral strategy is needed, addressing both the more general social, cultural, and structural determinants of SAM and the proximal health service factors [40, 41]. In order to address the various factors influencing the treatment outcomes of SAM, context-specific interventions involving local stakeholders and communities may prove advantageous [42].
Strengths and Limitations
Strengths
The study tackles childhood severe acute malnutrition, a serious public health issue that contributes significantly to under-five mortality in Ethiopia and other developing nations. To close knowledge gaps, it offers detailed data on treatment outcomes and related variables from an Ethiopian hospital setting. The reliability and precision of the quantitative results are increased by using a reasonably large sample size (n = 409). The methodology and study design are suitable for achieving the goals and enable statistical examination of the variables influencing nutritional recovery. Important factors that are precisely defined and measured include co-morbidities, age, sex, breastfeeding status, and treatment outcome.
Tables, figures, and text with a clear structure are used to present the results. Principal results are emphasized. Clinical records offer anthropometric and health data that are objective and unaffected by reporting bias. The results provide interventions aimed at enhancing the management of childhood SAM with relevant and practical evidence. Conclusion and recommendations clearly outline the implications for future research, practice, and policy. The study's results are compared to earlier research and the state of the regional health systems. The work is timely and relevant nationally due to its focus on an urgent child health priority in Ethiopia. In summary, this thesis's main strengths are its relevance to public health, its use of appropriate design and rigorous methods, its presentation of useful evidence, and its contribution to our understanding of one of the biggest problems affecting the nation's rates of child mortality and morbidity.
Limitations
Since a cross-sectional study design was used, it is not possible to establish a causal relationship between the factors examined and the results of nutritional recovery. The results of this retrospective study, which was conducted at a single centre, might not apply to other Ethiopian contexts with distinct patient populations, resources, and treatment practices. Data on some important variables, such as household socioeconomics, maternal factors, and qualitative insights, were unavailable due to the reliance on the review of medical records. The medical records under review may have inconsistent information, biases in reporting, or missing data. lack of ability to account for longitudinal effects or adjust for confounding variables due to the analysis's retrospective design.
The accuracy and comprehensiveness of the hospital's medical records could have affected how well the data was extracted. Possibility of subjectivity in treatment choices and nutritional evaluations were noted in patient records. Insufficient consideration of the community, health system, and policy-level elements influences SAM management. Qualitative data obtained from interviews with patients care givers may offer deeper insights not possible through quantitative methods. Overall, the limitations of this study underscore the need for more reliable study designs, data sources, and qualitative insights in order to fully comprehend the complex factors that influence children's nutritional recovery, even though it offers valuable evidence on the outcomes of SAM treatment.
Conclusions and Recommendation
Conclusion
In this study, severely malnourished under-five children admitted to Zewditu Hospital in Ethiopia were to have their treatment outcomes and associated factors evaluated. The most important conclusion was that, at 65.2% overall, the recovery rate was much lower than the minimum international standard of >75%. This suggests that the current state of managing severe acute malnutrition in this context is not optimal. A number of characteristics have been linked to a decreased chance of nutritional recovery, including being younger, female, not breastfeeding, and having co-morbid conditions like pneumonia and diarrhea. These correlations suggest that there are gaps in the early diagnosis of SAM, societal barriers, inadequate management of concurrent illnesses, and subpar feeding practices.
The necessity to give priority to SAM screening and prompt treatment in this high-risk age group is underscored by the noticeably poorer recovery observed in children younger than 24 months. To address the gender gap in treatment outcomes, targeted interventions are needed. It's also crucial to support the best breastfeeding practices by counseling careers. The detrimental effects of co-morbid infections must be addressed through integrated management of SAM and pediatric illnesses. Overall, the study shows that severe acute malnutrition is still a big concern in Ethiopia even with recent progress. In order to improve the quality and equity of care, communities, healthcare professionals, and stakeholders at all levels must work together to implement customized, context-specific interventions. Resolving more general socioeconomic, cultural and health systems issues will be essential to long-term improvement of SAM treatment results. Policy and programming can be guided by additional factors that can be clarified through further research.
Recommendation
Given the significant association between age and nutritional recovery, it is crucial to focus on early intervention strategies. Efforts should be made to identify SAM cases promptly and provide timely and appropriate treatment, particularly for children below 24 months. This includes strengthening community-based screening programs, promoting early detection, and ensuring swift referral to treatment centers. The observed gender disparity in nutritional recovery underscores the need for gender-responsive interventions. It is essential to address societal and cultural factors that contribute to differential outcomes between male and female children with SAM. This can be achieved by promoting gender equality and empowerment, ensuring equitable access to treatment and supportive services, and engaging communities in challenging gender-based norms and biases.
Recognizing the diverse contexts in which SAM occurs, interventions should be tailored to address specific local determinants. Factors such as socioeconomic status, access to healthcare, and cultural practices can significantly influence nutritional recovery. Therefore, interventions should be context-specific, considering the unique challenges and resources within each community. This may involve collaboration with local stakeholders, community engagement, and adaptive programming.
List of abbreviation
AACAHB - Addis Ababa city Administration Health Bureau
CFR - Case Fatality Rate
EDHS - Ethiopia Demographic Health Survey
HIV - Human immunodeficiency virus
NDHS - Nigerian Demographic and Health Survey
OTP - Outpatient Therapeutic care Programs
SAM - severe acute malnutrition
TB - Tuberculosis
TFU - Therapeutic feeding unit
URTI - Upper Respiratory Tract Infection
WHO - World Health Organization
References
- Workneh, z. (2020). treatment outcome of severe acute malnutrition and predictors of recovery in under five children in Ethiopia. BMC pediatrics, 3-4.
Publisher | Google Scholor - fasil wagaw, G.D. Meta analysis of inpatient tratment of severe acute malnutration and its predictors of mortality among under 5 childrens in Ethiopia, 4-5.
Publisher | Google Scholor - legesse, M, (2020). factors associated with child survival children admited to inpatient wards in public health institutions in Afar region. joural of health,population and Nutration, 4.
Publisher | Google Scholor - Gebretsadkan birhanu, k.z. (2020). Time of recovery from SAM and its predictors among under five childrens admitted in TFU in referal hospitals of tigray rigion. bmc pediatrics, 2020.
Publisher | Google Scholor - Yilma, D. (2018). predictors of recovery time from SAM among children who have been admitted to TFU in hospitals of southern Ethiopia. BMC pediatrics.
Publisher | Google Scholor - Getnet mekuriya, T.d. (2019). Treatmentoutcome and associated factors among under five children in Finote selam and Debremarkos hospitals. Bmj pediatrics, 3.
Publisher | Google Scholor - yohannes, m., treatment outcomes of SAM children admitted in TFU in wolayta zone, Ethiopia. Joural of health,population and nutration, 6.
Publisher | Google Scholor - Bihandari, N. (2019). Efficiecy of three feeding regimens for home-based managment of children with uncomplicated SAM in India. BMJ health, 5.
Publisher | Google Scholor - Das, k. (2020). Risk and adverse outcome factors of SAM children, a hospital-based study in Odishia. BMC pediatrics, 7.
Publisher | Google Scholor - Ikobah, J.m. (2021). Predictors of inpatient mortality of SAM of Hospitalized children in a Tirtiary facility in southers Nigeria. BMC pediatrics, 6.
Publisher | Google Scholor - Zaba, T., (2020). Factors associated with acute malnutrition among children 6-59 months in rural Mozambique. Maternal and child nutration, 5.
Publisher | Google Scholor - Muwanguzi, E., (2021). Treatment outcome and associated factors for severely malnourished children (1–5 years) admitted to Lacor Hospital and Gulu Regional Referral Hospital in Uganda. Joural of health,population and Nutration, 6.
Publisher | Google Scholor - Damtew, A., (2019). Prevalence, outcome and quality of care among children hospitalized with severe acute malnutrition in wastern Ethiopia: A multi-site observational study. BMC pediatrics, 9.
Publisher | Google Scholor - Gemechu, D.S. (2020). Determinants of severe acute malnutrition among children aged 6–59 months in the pastoral community of Liban District, Guji Zone, Oromia Regional State, Southeastern Ethiopia: a case–control study JNS, 8.
Publisher | Google Scholor - Abate, B.B. (2019). Treatment outcome of Severe Acute Malnutrition and associated factors among under-five children in outpatient therapeutics unit in Gubalafto Wereda, North Wollo Zone, Ethiopia. Plus, one, 6.
Publisher | Google Scholor - fasil wagaw, G.D. (2021). Treatment cure rate and its predictors among children with severe acute malnutrition in northwest Ethiopia: A retrospective record review. Plus, one, 8.
Publisher | Google Scholor - Hanna Demelash Desyibelew, A.F. Recovery rate and associated factors of children age 6 to 59 months admitted with severe acute malnutrition at inpatient unit of Bahir Dar Felege Hiwot Referral hospital therapeutic feeding unite, northwest Ethiopia. Plus One.
Publisher | Google Scholor - Muluken Berhanu Mena, M.G.D. (2021). Treatment Outcome of Severe Acute Malnutrition and Its Determinants among Pediatric Patients in West Ethiopia. Plus one, 8.
Publisher | Google Scholor - WHO. (2013). Updates on the management of severe acute malnutrition in infants and children. Geneva: World Health Organization.
Publisher | Google Scholor - Nigusse B, Haidar J, Mekonnen Y. (2021). Treatment outcome of severe acute malnutrition and predictors of recovery in under-five children in Woldia Hospital, Ethiopia. Nutrition.
Publisher | Google Scholor - Bisetegn A, Mihretie A, Wolde T. (2020). Predictors of time to recovery from severe acute malnutrition among children aged 6-59 months in Southern Ethiopia: a prospective cohort study. BMC Pediatr. 20(1):294.
Publisher | Google Scholor - Roba KT, O’Connor TP, Belachew T, O’Brien NM. (2016). Outcome of severe acute malnutrition in children aged 6-59 months: A prospective study from northern Ethiopia. Eur J Clin Nutr. 70(10):1139-1145.
Publisher | Google Scholor - Lelisa A, Shumet S. (2019). Time to recovery and associated factors among children with severe acute malnutrition treated at outpatient therapeutic care program in Sidama Zone, South Ethiopia: Retrospective Cohort Study. BMC Nutrition, 5(1):21.
Publisher | Google Scholor - Desyibelew HD, Fekadu A, Woldie H. (2019). Recovery rate and associated factors of severely malnourished children admitted to therapeutic feeding unit of Felege Hiwot Referral Hospital, Bahir Dar, Ethiopia. BMC Res Notes, 12(1):1-6.
Publisher | Google Scholor - Bulti A, Chane T, Dibaba Y, Garoma W. (2020). Treatment outcome and associated risk factors of severely malnourished under five children admitted to therapeutic feeding centers of Wolisso town, South West Shoa Zone, Oromia, Ethiopia: a retrospective cohort study.
Publisher | Google Scholor - Bahru B, Mesert Y, Godana W. (2017). Time to recovery and determinants of nutritional recovery time among severe acute malnourished children admitted to stabilization centers in Gedeo zone: prospective longitudinal study. BMC Pediatr. 17(1):1-2.
Publisher | Google Scholor - Kerac M, Briend A, Ag Ben’Farhat M, et al. (2020). Infectious comorbidities in acute malnutrition: A prospective cohort study from Niger. Am J Clin Nutr. 111(2):519-26.
Publisher | Google Scholor - Bhutta ZA, Das JK, Rizvi A, et al. (2013). Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 382(9890):452-77.
Publisher | Google Scholor - Chisti MJ, Salam MA, Bardhan PK, et al. (2015). Treatment failure and mortality amongst children with severe acute malnutrition presenting with cough or respiratory difficulty and radiological pneumonia. PLoS One, 10(10):e0140327.
Publisher | Google Scholor - Mahgoub HM, Adam I. (2012). Morbidity and mortality of severe malnutrition among Sudanese children in New Halfa Hospital, Eastern Sudan. Trans R Soc Trop Med Hyg. 106(2):66-68.
Publisher | Google Scholor - Hossain M, Chisti MJ, Hossain MI, Mahfuz M, Islam MM. (2012). Efficacy of World Health Organization guideline in facility-based reduction of mortality in severely malnourished children from low- and middle-income countries: a systematic review and meta-analysis. J.
Publisher | Google Scholor - Bergeron G, Castleman T. (2012). Program responses to acute and chronic malnutrition: divergences and convergences. Adv Nutr., 3(2):242-249.
Publisher | Google Scholor - Olofin I, McDonald CM, Ezzati M, et al. (2013). Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: a pooled analysis of ten prospective studies. PLoS One, 8(5):e64636.
Publisher | Google Scholor - Black RE, Victora CG, Walker SP, et al. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 382(9890):427-451.
Publisher | Google Scholor - Lamberti LM, Fischer Walker CL, Noiman A, Victora C, Black RE. (2011). Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health, 11(3):1-2.
Publisher | Google Scholor - Heikens GT, Bunn J, Amadi B, et al. Case management of HIV-infected severely malnourished children: challenges in the area of highest prevalence. Lancet, 371(9620):1305-1307.
Publisher | Google Scholor - Maitland K, Berkley JA, Shebbe M, et al. (2006). Children with severe malnutrition: can those at highest risk of death be identified with the WHO protocol? PLoS Med., 3(12):e500.
Publisher | Google Scholor - Sunguya BF, Poudel KC, Mlunde LB, et al. (2013). Effectiveness of nutrition training of health workers toward improving caregivers’ feeding practices for children aged six months to two years: a systematic review. Nutr J., 12:66.
Publisher | Google Scholor - Lenters LM, Wazny K, Webb P, Ahmed T, Bhutta ZA. (2013). Treatment of severe and moderate acute malnutrition in low- and middle-income settings: a systematic review, meta-analysis and Delphi process. BMC Public Health, 13(3):1-5.
Publisher | Google Scholor - Khara T, Dolan C. (2014). Technical Briefing Paper: Associations between Wasting and Stunting, policy, programming and research implications. Emergency Nutrition Network.
Publisher | Google Scholor - Briend A, Khara T, Dolan C. (2015). Wasting and stunting-similarities and differences: policy and programmatic implications. Food Nutr Bull, 36(1):S15-S23.
Publisher | Google Scholor - Bliss J, Lelijveld N, Briend A, et al. (2018). Use of mid-upper arm circumference by novel community platforms to detect, diagnose, and treat severe acute malnutrition in children: a systematic review. Glob Health Sci Pract, 6(3):552-564.
Publisher | Google Scholor












