

Review Article
Tibiofibular Syndesmosis Injury-Comparative Analysis Between Suture Button and Transindesmal Screw Fixation-A Systematic Review with Meta-Analysis
- Bianca Gabriella de Oliveira 1*
- Thiago de Souza Costa 2
- Chrisd’Angelo Dias Verçosa 3
- Leandro Ayres Montenegro 4
- Antônio de Figueiredo Barbosa Neto 4
- Melissa Alves Aires Marques 5
1Medical student at Universidade Salvador-UNIFACS, Salvador, BA, Brazil.
2Orthopedist and Traumatologist, Complexo Hospitalar Manoel André, Arapiraca, AL.
3Resident Orthopedist and Traumatologist, Carvalho Beltrão Hospital, Coruripe, AL.
4Resident Orthopedist and Traumatologist, Hospital Carvalho Beltrão, Coruripe, AL.
5Medical student at Universidade Iguaçu, Itaperuna, RJ.
*Corresponding Author: Bianca Gabriella de Oliveira, Medical student at Universidade Salvador-UNIFACS, Salvador, BA, Brazil.
Citation: Bianca G. Oliveira, Thiago S. Costa, C.A.D. Verçosa, Leandro A. Montenegro, A.F.B. Neto, et al. (2024). Tibiofibular Syndesmosis Injury: Comparative Analysis Between Suture Button and Transindesmal Screw Fixation-A Systematic Review with Meta-Analysis, Clinical Interventions and Clinical Trials, BioRes Scientia Publishers. 2(2):1-9. DOI: 10.59657/2993-1096.brs.24.021
Copyright: © 2024 Bianca Gabriella de Oliveira, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 24, 2024 | Accepted: March 11, 2024 | Published: April 16, 2024
Abstract
Objective: The aim of this study was therefore to compare the functional results obtained by the suture button and transindesmal screw fixation techniques in the treatment of tibiofibular syndesmosis lesions.
Methodology: This is a retrospective study based on a systematic review with meta-analysis registered with the International prospective register of systematic reviews (PROSPERO) under ID CRD42024512033in order to improve the quality and suitability of the results to the proposed objectives.
Results: A total of 185 articles were selected during the search process; after excluding those published more than 15 years ago, 54 remained. Analysis of the title and abstract allowed 35 articles that did not correspond to the objective of this study to be excluded. A complete reading of 19 articles was carried out, 13 of which were excluded because they did not meet the inclusion criteria, and finally 6 were selected for the article.
Discussion: The American Orthopaedic Foot and Ankle Society (AOFAS) is a form of clinical and functional assessment for the ankle and hindfoot. In all the studies used for analysis, patients in the SB group had a slightly better score when compared to the SS group. The suture button was also related to a better post-operative VAS (pain analogue scale) index, fewer complications, loosening or need for reoperations.
Conclusion: It can be concluded that suture button therapy is as reliable and reproducible as the screw method, and can even be used as an alternative with similar clinical results. It is still controversial as to which is the best option, but lower rates of second procedures, lower patient and clinical costs and faster loading times were found with suture-button therapy. It may be more beneficial for patients, and consequently for orthopaedic surgeons, to opt for dynamic fixation rather than the usual and traditional static fixation.
Keywords: tibiofibular syndesmosis injury; suture button; transindesmal screw fixation
Introduction
Syndesmosis is the result of ankle rotational mechanisms commonly associated with ankle fractures. It reflects a prevalence of 40% of trauma patients with syndesmotic injury, also referred to as distal tibiofibular instability. Isolated ligament injuries are rare and mostly result from sports practice, which can have repercussions on the functionality of the joint, making early diagnosis and appropriate treatment essential, especially in association with ankle fractures [1]. There is no precisely established standard therapeutic protocol, given the high prevalence of ankle fractures and the high incidence of associated syndesmophyte injuries. Syndesmosis fixation consists of the surgical insertion of a syndesmotic screw through the fibula into the tibia with the aim of reduction as the ligaments undergo the healing process [2,3]. Ligament healing takes place within 8 to 12 weeks, including the functional regenerative process: gradual biomechanical capacity in view of the severity of the injury, thus questioning the redundancy of whether or not the orthopaedic implant needs to remain in place [3,4,5]. In light of this, the removal of this screw is discussed due to the possibility of a proposed reduction in range of motion and the presence of unnecessary hardware. In addition to another theory which supports the defense of screw breakage over time by raising the question of limiting the normal movement of rotation and translation of the fibula in the distal tibio-fibular joint which occurs during weight bearing, leading some professionals to adopt routine removal as a standard treatment procedure [6,7].
On the other scientific side, there is an orthopedic class in favor of retaining screws, weighing up the fact that there is no significant improvement in functional results and the unnecessary submission to another surgical procedure, which includes: tissue recovery, increased costs, time off work, possible surgical risks, infection and scar aesthetics, since it is a fact that all surgery generates an endocrine-metabolic response to trauma, albeit smaller and less invasive [8]. The main therapeutic choice for syndesmotic injuries associated with ankle fractures has been static fixation using a syndesmotic screw. This can be metallic or bioabsorbable, of different diameters and lengths and inserted in different positions. However, in recent years, the use of the dynamic suture button technique has been considered instead of screws. This technique involves fixing the syndesmosis using a trans-syndesmotic fiber thread fixed with knotless sutures, regularly on a fibular plate. Its main advantage is that it allows physiological movement between the tibia and fibula while maintaining a correct reduction, as well as eliminating the need to remove the implant, which is one of the biggest disadvantages of static fixation [1,2,3,18,21,23,24,25,26]. The aim of this study was therefore to compare the functional results obtained by the suture button and transdermal screw fixation techniques in the treatment of tibiofibular syndesmosis lesions.
Methodology
This is a retrospective study based on a systematic review with meta-analysis registered with the International prospective register of systematic reviews (PROSPERO) under ID CRD42024512033in order to improve the quality and suitability of the results to the proposed objectives.
Database and Bibliographic Survey
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline9 and is a retrospective study carried out using a systematic review with METANALYSIS. The search was carried out using the following search terms in the PubMed, EMBASE, Scopus, Ovid and Cochrane Library databases. A text search strategy was employed using the search sequence syndesmosis injury OR syndesmosis injury, excluding all articles not pertaining to the ankle. As this was a meta-analysis of published studies, there was no need for approval by the ethics committee or institutional scientific review board. The reference lists of the included and previously published articles were searched for more relevant studies that met the eligibility criteria. In order to select the studies, the inclusion criteria were studying whose sample included patients with tibiofibular syndesmosis lesions treated using the suture button and transdermal screw procedures. Studies with other approaches were excluded from the search.
We sought to analyze the applicability of the surgical procedure in the approach to tibiofibular syndesmosis injuries, such as eligibility criteria for the procedure, associated risks and benefits, correlation between the procedure and functionality after surgery or length of hospital stay after the procedure. Three independent reviewers applied the eligibility criteria and selected the studies for inclusion in the systematic review. The researchers were blind to each other's decisions. Information on study design, study methodology, participant demographics (age, gender), baseline characteristics (degree of injury, previous surgeries) was extracted from the studies. The Systematic Review Data Repository-Plus software tool was used. It was also decided to use the Cochrane risk of bias tool for greater reliability of the results. The results were synthesized qualitatively and by combining data from individual studies that addressed the associated benefits and/or risks.
Results
A total of 185 articles were selected during the search process; after excluding those published more than 15 years ago, 54 remained. Analysis of the title and abstract allowed 35 articles that did not correspond to the objective of this study to be excluded. A complete reading of 19 articles was carried out, 13 of which were excluded because they did not meet the inclusion criteria, and finally 6 were selected for the article (Figure 1).
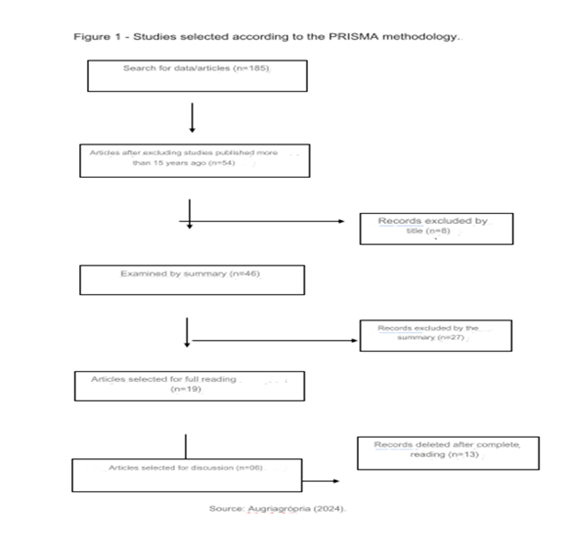
Figure 1: Studies selected according to the PRISMA methodology
The six articles selected featured patients diagnosed with tibiofibular syndesmosis injuries who underwent treatment using a suture button or transindesmal screw. Functional assessment was carried out using the Ankle Hindfoot Scale of the American Orthopaedic Foot and Ankle Society (AOFAS), as well as the VAS (Analog Pain Assessment) and OMAS (Olerud-Molander Ankle Score) scales, which have been relaxed in some studies. A total of 390 patients were included. Of these, 211 underwent the surgical procedure for tibiofibular syndesmosis injury using the suture button (SB) technique and 179 using the transindesmal screw (SS). Table 1 shows the articles selected and their results (Table 1). Table 2 contains the American Orthopaedic Foot and Ankle Society (AOFAS) post-operative score after one year of the procedure [10,11,12,13,14,15].
Table 1: Resultados obtidos pelos estudos selecionados.
| Study | Approach | Patients F/M | Results |
| Grove e coli | suture button Syndesmosis screw fixation | 16/ 27 | American Orthopaedic Foot and Ankle Society (AOFAS); Olerud-Molander Ankle Score (OMAS) e o RAND-36 Item Health Survey for Quality-of-Life (RAND-36) |
| Kurtogluv has heard | suture button Syndesmosis screw fixation | 22/47 | Complications, interval to weight bearing, fracture pattern, postoperative American Orthopedic Foot and Ankle Society (AOFAS) score, Foot and Ankle Disability Index (FADI) scores |
| Saves e coli | suture button Syndesmosis screw fixation | 33/64 | American Orthopedic Foot and Ankle Society (AOFAS); Olerud-Molander Ankle (OMA); EuroQol-5D15 index (EQ-5D); visual analog scale (VAS); range of motion; complications. |
| Kocadal is col | suture button Syndesmosis screw fixation | 19/33 | American Orthopaedic Foot and Ankle Society (AOFAS); avaliação radiologica. |
| Xu e col | suture button Syndesmosis screw fixation | 43/33 | American Orthopedic Foot and Ankle Society (AOFAS); AO classification; Olerud-Molander Ankle Score; complications |
| Andersen et al | suture button Syndesmosis screw fixation | 23/30 | American Orthopedic Foot & Ankle Society (AOFAS); Olerud-Molander Ankle (OMA), the visual analogue scale (VAS) and the EuroQol-5D Index (EQ-5D) and VAS. |
Table 2: American Orthopedic Foot and Ankle Society (AOFAS) postoperative score 1 year after the procedure.
| Study | Sample | Age | Screw fixing | suture button |
| Lehtola e co | 43 patients | 45 years | 88 +- 7.1 | 78 +- 7 |
| Kurtogluv has heard | 69 patients | 37 years | 84 +- 10 | 86 +- 10 |
| Saves e coli | 97patients | 45 years | 87 +- 6 | 96 +- 7 |
| Kocadal is col | 52 patients | 44,8 years | 86,1 +- 14 | 88,4 +- 9,2 |
| Xu e col | 76 patients | 38,9 years | 90.6 +- 13,8 | 91.1 +- 10 |
| Andersen et al | 53 patients | 40 years | 86 +- 9 | 96 +- 10 |
Figure 2 shows the American Orthopaedic Foot and Ankle Society (AOFAS) analysis of the functional assessment of patients undergoing treatment for tibiofibular syndesmosis lesions [10,11,12,13,14,15].
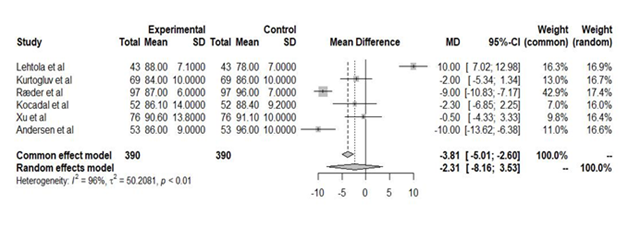
Figure 2: Gráfic forest
In the randomized clinical trial by Lehtola et al,10 21 patients underwent the suture button (SB) procedure and 22 underwent screw fixation of the syndesmosis (SS). The patients selected were skeletally mature with PER 4/Weber C ankle fractures. Of the patients in the SB group, 14.2% had an inadequate reduction at some point during follow-up, while for the SS group this figure was 28.5%. The mean OMAS (Olerud-Molander Ankle Score) was 88 in the SS group and 78 in the SB group (difference between the two of 7.1, 95% CI: -7.0-21.1, P = 0.32). In relation to the RAND-36 (Health Survey for Quality-of-Life) when assessing physical function, the results were similar between the groups, with values of 68 ( -27.7) and 77 ( -23.4) for suture screw and suture button, respectively. In the SS group, the screw was removed in 4 patients, 1 was broken, all the others showed signs of loosening, however, asymptomatic. In the SB, 2 showed signs of osteolysis, asymptomatic. Kurtoglu et al11 presented a retrospective study of 43 patients who underwent the suture button procedure (SB) and 26 syndesmosis screw fixation (SS). The average postoperative Foot and Ankle Disability Index (FADI) score was 79 (range 65-90) in the single suture button group and 77 (range 55-90) in the screw group. The AOFAS index was 86 +- 10 for the SB group and 84 +- 10 for the SS group. In the randomized clinical trial by Raeder et al12, 47 patients were included in the SB group and 47 in the SS group. The SB group had an AOFAS score of 100 (interquartile range (IQR) 92 to 100), while in the SS group this value was 90 (IQR 85 to 100). The mean OMA score was higher in the SB group, 100 (IQR 95 to 100) and 95 (IQR 75 to 100) in the SS group. After five years, there was no difference in the VAS index, EQ-5D (EuroQol-5D15 index). Ankle dorsiflexion capacity was better in the SB group.
In the study by Kocadal et al13, 26 patients underwent SS and 26 underwent SB. The mean AOFAS score was 88.4 ± 9.2 in the suture button fixation group and 86.1 ± 14.0 in the screw fixation group (P = .4). In the SS group, the implant was removed in 10 patients. The average removal period was 12.4 ± 5.1 (range 7 to 23) weeks. Screw breakage occurred in 1 patient. Another patient developed reflex sympathetic dystrophy and was treated conservatively. The study pointed out that although the functional results of the two techniques were similar, restoring fibular rotation after syndesmotic injuries via screw fixation can cause problems. In the retrospective study by Xu et al14, 34 patients took part in the SB group and 42 in the SS group. With regard to complications, the suture button group reported 1 case of implant irritation, 2 cases of recurrent diastasis of the distal tibiofibular syndesmosis, 2 cases of deep vein thrombosis and 1 case of surgical site infection. In the syndesmotic screw group, there were 2 cases of implant irritation, 2 cases of implant loosening and breakage, 1 case of deep vein thrombosis. The total weight bearing time was shorter in the suture button group than in the syndesmotic screw fixation group.
In the randomized clinical trial by Andersen et al15, the mean AOFAS score was higher in the SB group (96 [interquartile range, or IQR, 90 to 100] versus 86 [IQR, 80 to 96]; p = 0.001) for the SB group.
Discussion
The American Orthopaedic Foot and Ankle Society (AOFAS) is a form of clinical and functional assessment for the ankle and hindfoot. In all the studies used for analysis, patients in the SB group had a slightly better score when compared to the SS group. The suture button was also related to a better post-operative VAS (pain analogue scale) index, fewer complications, loosening or need for reoperations [10,11,12]. Removal of the syndesmotic screw is a short surgical procedure, usually lasting less than an hour. The use of prophylactic antibiotics is therefore not routinely used. Infectious complications have a surgical site infection (SSI) rate of up to 9%. With the relatively high complication rate of screw removal in mind, it could be beneficial to retain them or remove them only if the patient presents difficulties [16,17]. The bony ankle joint corresponds to the articulation of the tibia and fibula with the talus. The ligamentous stability of the joint comes laterally from the anterior talofibular ligament, the calcaneofibular ligament and the posterior talofibular ligament; proximally from the tibiofibular syndesmosis; medially from the deltoid ligament and circumferentially from the joint capsule. Syndesmosis is defined as a fibrous joint made up of adjacent bones connected by ligaments or membranes. The tibiofibular syndesmosis is made up of four ligamentous structures: the anterior and posterior tibiofibular ligaments, the transverse ligament and the interosseous membrane [18].
The anterior tibiofibular ligament, trapezoidal in shape and wide, lies superior to the anterior arch of the ankle joint and runs postero-inferiorly from the tibia to the fibula. The posterior ligament is similar in shape to the anterior ligament and is located superiorly to the posterior arch, running anteroinferiorly from the tibia to the fibula. Posteriorly, there is the transverse ligament, which is thick and round and extends horizontally from the tibia to the fibula. Now, on to the interosseous membrane, it extends from the tibia to the fibula, running most of the length of both bones, fusing with the anterior and posterior tibiofibular ligaments. Strong but flexible, it provides a certain degree of elasticity during walking. If the ankle is fully flexed, the syndesmosis is put under strain, and if an external rotation force is added to this joint, there is a greater risk of rupture [18,19]. This injury often occurs due to a lateral force superimposed on an ankle that is dorsiflexed. This force causes the talus to press against the distal fibula, is transmitted and applies pressure to the syndesmosis. This tension causes a series of injuries that depend on the degree of force applied. The first injury is a rupture of the anterior tibiofibular ligament, accompanied by the interosseous membrane. If too much force is applied, the next to break is the posterior tibiofibular ligament, followed by medial damage to the deltoid ligament. In some cases, a spiral fracture of the proximal fibula can occur, called a Maisonneuve fracture [18].
The most common mechanisms causing injury to the syndesmosis are hyper dorsiflexion and external rotation, while inversion, eversion, plantar flexion, pronation and internal rotation are less common. These injuries commonly occur in high-impact sports activities, such as skiing and soccer, or in low-impact accidents, such as falling down a flight of stairs or slipping on ice [20,21]. It is essential to identify a syndesmosis injury in order to develop a therapeutic plan with the best results and a good recovery. Its diagnostic investigation includes a clinical and radiological assessment. Physical examinations can show tenderness during palpation of the anterior surface of the ankle, felt over the interosseous membrane, the anterior and posterior tibiofibular ligaments [19]. Clinically, it is difficult for patients to have swelling and bruising, but they do present with ankle instability, pain in the medial ankle joint and pain during loading in the anterior distal part of the tibia and fibula. If the individual is unable to perform a compression test or a single-leg jump, X-rays should be taken to rule out a possible fracture. If there is no fracture but there is diastasis, the patient can be followed up with an orthopedist for a grade 3 injury [22,23]. If there is no diastasis or fracture, it could be a grade 1 or 2 injury, and ultrasound scans should be carried out to determine the extent of the injury to the tendon. If a partial tear of the anterior tibiofibular ligament is observed, it is a grade 1 injury and can be followed up conversationally. Now, if you see a complete rupture of the ligament, you have a grade 2 injury and are referred to an orthopedist. If ultrasound images are not available at the time, the joint should be immobilized, referred to the orthopedist and MRI images obtained [24,25].
Currently, there are static and dynamic surgical methods that can be used for stabilization. The main aim of both methods is to restore the ankle to its original anatomical structure. This restructuring allows the syndesmosis to heal properly. The first step in preventing post-traumatic arthritis is to reduce the fibula in the fibular notch [24,25,26,27]. For years, the syndesmotic screw has been the main therapeutic method for stabilizing syndesmosis injuries. However, an inflexible screw to re-establish the dynamic function of the syndesmotic ligaments is unnatural, as well as preventing a rapid return to a full range of movement and weight bearing [19,28]. With regard to the surgical procedure, the screw is inserted parallel to the tibiotalar joint, avoiding displacement of the fibula, and is generally placed 2 to 4 centimeters above the tibial pilon and at an anteromedial angle of 30 degrees. This angle provides adequate fixation of the fibula in the tibiofibular notch. It is also common to insert the screw with the foot in dorsiflexion, due to the talus widening the ankle [18]. The disadvantages added to the high levels of invasiveness that screw insertion requires, the high risk of infectious complications, non-union or delayed consolidation, the discomfort and loosening of the screw must be weighed up when choosing this form of treatment. Generally, the patient is immobilized and non-weight bearing for six to eight weeks before the second surgery to remove the screw. In addition, during these weeks, there is a risk of recurrence of diastasis and breakage of the screw due to force [19,20,21,29]. Even though screws require secondary surgery for removal, there is still no agreement on whether or not this device should be removed. Some authors recommend removal after the initial procedure, while others do not. In addition, complications associated with the additional procedure include recurrent syndesmosis diastasis, deep and superficial infections. The literature shows that early removal of screws before ligament healing is related to the risk of recurrent diastasis [18,19,30,31,32,33].
For this reason, the implanted suture button offers advantages over the screw, being an alternative method, a dynamic fixation. This includes faster return to mobility, lower levels of pain caused by hardware and recurrent syndesmotic diastasis, maintenance of physiological movement even in reduction, early rehabilitation and no need to remove the prosthesis. The dynamic suture-button technique involves fixing the distal tibiofibular syndesmosis using a trans-syndesmotic fiber thread fixed with knotless sutures to a fabric plate [20,22,33,34,35,36]. Surgeons have become increasingly familiar with suture-button fixation devices due to the various manufacturers. In general, a pass-through guide wire is used to position a button device on the medial cortex of the tibia, which is turned, allowing cortical fixation. The lateral button is then tightened onto the lateral cortex of the fibula or the fibula reinforcement plate [37]. This dynamic technique allows movement between the tibia and fibula, guarantees a reduction in syndesmosis and rules out a second surgery to remove the device. In addition, the patient has less pain and discomfort and a greater range of movement, which may help with earlier full weight bearing [38,39].
However, button devices carry a certain risk of deep infections, subsequent erosion by the fiber thread and entrapment of the neurovascular bundle. Osteomyelitis has been reported as a complication, including intraosseous migration of the lateral endobutton and incorrect positioning of the medial endobutton. There have also been reports of knot irritation and subsidence of the bone by the fiber wire [40,41,42]. The question of cost-effectiveness between traditional syndesmotic screw and suture-button methods has been analyzed. One study found that button devices have a removal rate of 10% and screws 20%, showing that the suture-button is more economical than the traditional therapeutic option. Furthermore, the current Up-To-Date literature advises removing 100% of screws before full loading, increasing the cost of second procedures [40,4].
Conclusion
It can be concluded that suture button therapy is as reliable and reproducible as the screw method, and can even be used as an alternative with similar clinical results. It is still controversial as to which is the best option, but lower rates of second procedures, lower patient and clinical costs and faster loading times were found with suture-button therapy. It may be more beneficial for patients, and consequently for orthopaedic surgeons, to opt for dynamic fixation rather than the usual and traditional static fixation.
References
- Sanders FRK, Birnie MF, Dingemans SA, et al. (2021). Functional outcome of routine versus on-demand removal of the syndesmotic screw: a multicentre randomized controlled trial. Bone Joint J, 103(11):1709-1716.
Publisher | Google Scholor - Zhang YW, Rui YF. (2021). A systematic review of the
Publisher | Google Scholor - Khurana A, Kumar A, Katekar S, et al. (2021). Is routine removal of syndesmotic screw justified? A meta-analysis. Foot (Edinb), 49:101776.
Publisher | Google Scholor - Bragg JT, Masood RM, Spence SS, et al. (2023). Predictors of Hardware Removal in Orthopaedic Trauma Patients Undergoing Syndesmotic Ankle Fixation with Screws. Foot Ankle Orthop, 8(3):24730114231198841.
Publisher | Google Scholor - Fenelon C, Murphy EP, Galbraith JG, Kearns SR. (2019). The burden of hardware removal in ankle fractures: How common is it, why do we do it and what is the cost? A ten-year review. Foot Ankle Surg, 25(4):546-549.
Publisher | Google Scholor - Desouky O, Elseby A, Ghalab AH. (2021). Removal of Syndesmotic Screw After Fixation in Ankle Fractures: A Systematic Review. Cureus, 13(6):15435.
Publisher | Google Scholor - Clanton TO, Whitlow SR, Williams BT, et al. (2017). Biomechanical Comparison of 3 Current Ankle Syndesmosis Repair Techniques. Foot Ankle Int, 38(2):200-207.
Publisher | Google Scholor - Hamid N, Loeffler BJ, Braddy W, Kellam JF, Cohen BE. (2009). Outcome after fixation of ankle fractures with an injury to the syndesmosis: the effect of the syndesmosis screw. J Bone Joint Surg Br, 91(8):1069-1073.
Publisher | Google Scholor - Page MJ, McKenzie JE, Bossuyt PM, et al. (2022). A declaração PRISMA 2020: diretriz atualizada para relatar revisões sistemáticas The PRISMA 2020 statement: an updated guideline for reporting systematic reviewsDeclaración PRISMA 2020: una guía actualizada para la publicación de revisiones sistemáticas. Rev Panam Salud Publica, 46:112
Publisher | Google Scholor - Lehtola R, Leskelä HV, Flinkkilä T, Pakarinen H, Niinimäki J. (2021). Suture button versus syndesmosis screw fixation in pronation-external rotation ankle fractures: A minimum 6-year follow-up of a randomised controlled trial. Injury, 52(10):3143-3149.
Publisher | Google Scholor - Kurtoglu A, Kochai A, Inanmaz ME, Sukur E, Keskin D. (2021). A comparison of double single suture-button fixation, suture-button fixation, and screw fixation for ankle syndesmosis injury: A retrospective cohort study. Medicine (Baltimore), 100(13):25328.
Publisher | Google Scholor - Ræder BW, Figved W, Madsen JE, Frihagen F, Jacobsen SB. et.al. (2020). Better outcome for suture button compared with single syndesmotic screw for syndesmosis injury: five-year results of a randomized controlled trial. Bone Joint J,102-(2):212-219.
Publisher | Google Scholor - Kocadal O, Yucel M, Pepe M, Aksahin E, Aktekin CN. (2016). Evaluation of Reduction Accuracy of Suture-Button and Screw Fixation Techniques for Syndesmotic Injuries. Foot Ankle Int, 37(12):1317-1325.
Publisher | Google Scholor - Xu Y, Kang R, Li M, Li Z, Ma T. et.al. (2022). The Clinical Efficacy of Suture-Button Fixation and Trans-Syndesmotic Screw Fixation in the Treatment of Ankle Fracture Combined with Distal Tibiofibular Syndesmosis Injury: A Retrospective Study. J Footlve Ankle Surg, 61(1):143-148.
Publisher | Google Scholor - Andersen MR, Frihagen F, Hellund JC, Madsen JE, Figved W. (2018). Ensaio Randomizado Comparando o Botão de Sutura com Parafuso Sindesmótico Único para Lesão de Sindesmose. J Surg da articulação óssea Am,100(1):2-12.
Publisher | Google Scholor - Kaftandziev I, Spasov M, Trpeski S, Zafirova-Ivanovska B, Bakota B. (2015). Fate of the syndesmotic screw--Search for a prudent solution. Injury, (46)6:125-129.
Publisher | Google Scholor - Boyle MJ, Gao R, Frampton CM, Coleman B. (2014). Removal of the syndesmotic screw after the surgical treatment of a fracture of the ankle in adult patients does not affect one-year outcomes: a randomised controlled trial. Bone Joint J, 96-(12):1699-1705.
Publisher | Google Scholor - Stiene, Andrew, et al. (2019).
Publisher | Google Scholor - Liu, Jiayong, Daniel Valentine, and Nabil A. Ebraheim. (2022).
Publisher | Google Scholor - Norkus SA, Floyd RT. (2001). The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train, 36:68-73.
Publisher | Google Scholor - Van Heest TJ, Lafferty PM. (2014). Injuries to the ankle syndesmosis. J Bone Joint Surg Am, 96:603-613.
Publisher | Google Scholor - de-Las-Heras Romero J, Alvarez AML, Sanchez FM, et al. (2017). Management of syndesmotic injuries of the ankle. EFORT Open Rev, 2(9):403-409.
Publisher | Google Scholor - Michelson JD, Magid D, McHale K. (2007). Clinical utility of a stability-based ankle fracture classification system. J Orthop Trauma, 21(5):307-315.
Publisher | Google Scholor - Calder JD, Bamford R, Petrie A, McCollum GA. (2016). Stable versus unstable grade II high ankle sprains: a prospective study predicting the need for surgical stabilization and time to return to sports. Arthroscopy, 32(4):634-642.
Publisher | Google Scholor - Porter DA, Jaggers RR, Barnes AF, Rund AM. (2014). Optimal management of ankle syndesmosis injuries. Open Access J Sports Med, 5:173-182.
Publisher | Google Scholor - Peek AC, Fitzgerald CE, Charalambides C. (2014). Syndesmosis screws: how many, what diameter, where and should they be removed? A literature reviews. Injury, 45:1262-1267.
Publisher | Google Scholor - Illinois Bone & Joint Institute. Available.
Publisher | Google Scholor - Huber T, Schmoelz W, Bo ̈lderl A. (2012). Motion of the fibula relative to the tibia and its alterations with syndesmosis screws: a cadaver study. Foot Ankle Surg, 18(3):203-209.
Publisher | Google Scholor - Magan A, Golano P, Maffulli N, Khanduja V. (2014). Evaluation and management of injuries of the tibiofibular syndesmosis. Br Med Bull, 111:101-115.
Publisher | Google Scholor - Walley KC, Hofmann KJ, Velasco BT, Kwon JY. (2017). Removal of hardware after syndesmotic screw fixation: a systematic literature review. Foot Ankle Spec. 10:252-257.
Publisher | Google Scholor - Naumann MG, Sigurdsen U, Utvag SE, Stavem K. (2016). Incidence and risk factors for removal of an internal fixation following surgery for ankle fracture: a retrospective cohort study of 997 patients. Injury, 47:1783-1788.
Publisher | Google Scholor - Schepers T, Van Lieshout EM, de Vries MR, Van der Elst M. (2011). Complications of syndesmotic screw removal. Foot Ankle Int, 32(11):1040-1044.
Publisher | Google Scholor - Latham AJ, Goodwin PC, Stirling B et al: (2017). Ankle syndesmosis repair and re- habilitation in professional rugby league players: A case series report. BMJ Open Sport Exerc Med.
Publisher | Google Scholor - Schnetzke M, Vetter SY, Beisemann N et al: (2016). Management of syndesmotic injuries: What is the evidence? World J Orthop, 7:718-725.
Publisher | Google Scholor - Degroot H, Al-omari AA, El ghazaly SA. (2011). Outcomes of suture button repair of the distal tibiofibular syndesmosis. Foot (Edinb), 32:250-256.
Publisher | Google Scholor - Bafna KR, Jordan R, Yatsonsky D 2nd, Dick S, Liu J. et.al. (2020). Revision of syndesmosis screw fixation. Foot Ankle Spec, 13(2):138-143.
Publisher | Google Scholor - Laflamme M, Belzile EL, Bédard L, Van Den Bekerom MPJ. (2015). A prospective randomized multicenter trial comparing clinical outcomes of patients treated surgically with a static or dynamic implant for acute ankle syndesmosis rupture. J Orthop Trauma, 29(5):216-223.
Publisher | Google Scholor - Fantry AJ, O'Donnell SW, Born CT, Hayda RA. (2017). Deep infections after syndesmotic fixation with a suture button device. Orthopedics, 40:541-545.
Publisher | Google Scholor - Hong CC, Lee WT, Tan KJ. (2015). Osteomyelitis after TightRope(!) fixation of the ankle syn- desmosis: a case report and review of the literature. J Foot Ankle Surg, 54:130-134.
Publisher | Google Scholor - Rigby RB, Cottom JM. (2013). Does the Arthrex TightRope! provide maintenance of the distal tibiofibular syndesmosis? A 2-year follow-up of 64 TightRopes! in 37 patients. J Foot Ankle Surg, 52:563-567.
Publisher | Google Scholor - Neary KC, Mormino MA, Wang H. (2017). Suture button fixation versus syndesmotic screws in supination-external rotation type 4 injuries. Am J Sports Med, 45:210-217.Molloy A, Selvan D. Ligamentous injuries of the foot and ankle. In: Thompson SR, ed. DeLee & Drez’s Orthopaedic Sports Medicine Principles and Practice, 4th ed, Philadel- phia, Elsevier Saunders, 2015.1392.
Publisher | Google Scholor












