

Case Report
Successful Twin Pregnancy in A Unicornuate Uterus with Non-Communicating Rudimentary Horn
- Nassima Ouguerzi 1*
- Moad Belouad 1
- Othmane Echerfaoui 1
- Saad Benali 1
- Moulay Mahdi Elhassani 1
- Jaouad Kouach 1
Department of Gynecology and Obstetrics, Military Hospital of Instruction Mohamed V Rabat, Rabat, Morocco.
*Corresponding Author: Nassima Ouguerzi
Citation: Ouguerzi N, Moad B, Echerfaoui O, Benali S, Moulay M. Elhassani, et al. (2024). Successful Twin Pregnancy in a Unicornuate Uterus with Non-Communicating Rudimentary Horn. Clinical Obstetrics and Gynecology Research. BioRes Scientia Publishers. 3(3): 1-4. DOI: 10.59657/2992-9725.brs.24.018
Copyright: © 2024 Nassima Ouguerzi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 11, 2024 | Accepted: August 25, 2024 | Published: September 05, 2024
Abstract
Congenital abnormalities of the uterus, such as unicornuate uterus with a non-communicating rudimentary horn, present unique challenges in pregnancy. This case report describes a successful twin pregnancy in a 26-year-old primiparous woman with this rare uterine anomaly. The diagnosis was confirmed by ultrasound and MRI, and the pregnancy was closely monitored due to the increased risk of complications. Despite concerns of abortion and premature delivery, the patient delivered healthy twins at 37 weeks via cesarean section. This case highlights the importance of early detection, close monitoring, and appropriate management in achieving a positive outcome in pregnancies complicated by uterine malformations.
Keywords: unicornuate uterus rudimentary horn; twin pregnancy
Introduction
Abnormal Mullerian duct development, fusion, or reabsorption during fetal life causes congenital abnormalities of the uterus. These abnormalities affect 1–10% of the general population, 2–8% of infertile women, and 5–30% of women who had previous pregnancy loss[1]. Additionally, these congenital defects are linked to unfavorable outcomes at the end of pregnancy, including early births and unusual presentations [2]. The incidence of twin pregnancy filling the unicornuate uterus and its associated rudimentary horn is believed to be one in every 10 million gestations [3]. A rudimentary horn with unicornuate uterus is caused by inadequate development of one Müllerian duct and partial fusion of the contralateral one. The rudimentary horn is non-communicative and typically linked to ectopic pregnancy [4]. We present a case report of a successful pregnancy in a unicornuate uterus.
Case report
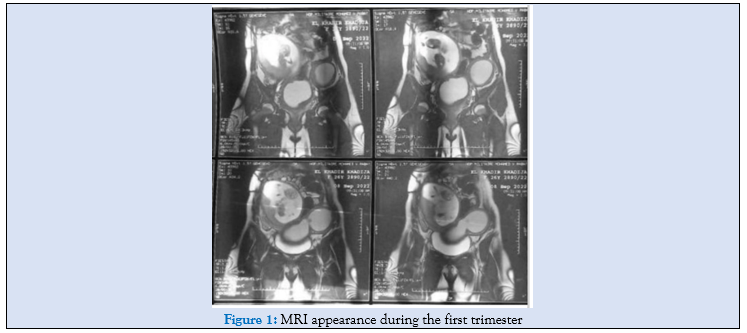
26-year-old primiparous parturient, the diagnosis of uterine malformation of the type of unicornuate uterus with a rudimentary cavity was suspected during the pregnancy confirmation ultrasound at 7 weeks and then confirmed by MRI. the patient was initially admitted to hospital for a risk of abortion at 14 weeks, which progressed well, and then at 33 weeks for a risk of premature delivery, which progressed well under tocolysis and lung maturation.
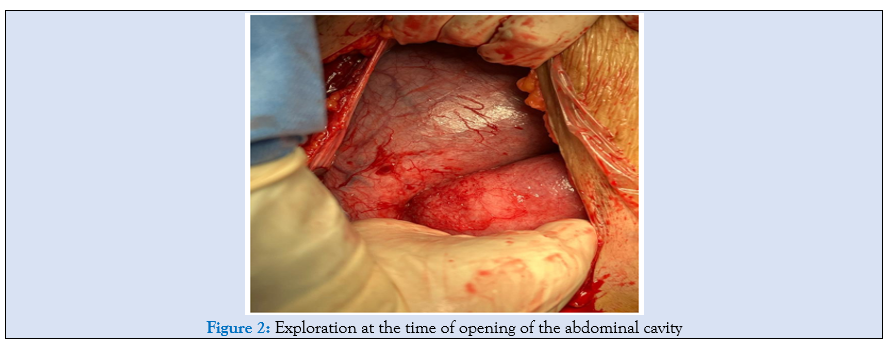
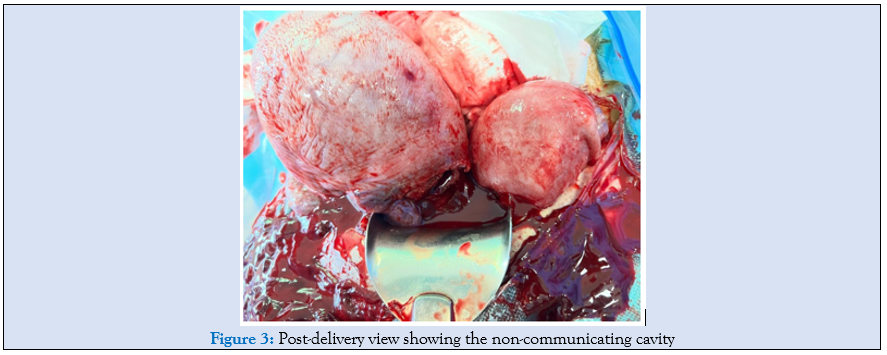
The patient gave birth at 37 weeks to 2 twins weighing 2200 g and 2090 g by cesarean section. exploration confirmed the ESHRE class U4 malformation, i.e., a unicornuate uterus with a rudimentary non-communicating cavity.
Discussion
Congenital abnormalities of the female genital tract are caused by embryological maldevelopment of the Mullerian or paramesonephric ducts. They are a somewhat frequent benign disorder, with a frequency of 4-7% [5]. Class U4 of ESHRE/ESGE classification or hemi-uterus includes all cases of unilaterally formed uterus. This is a failure to form; the need to classify it in a separate class from the aplastic uterus (failure to form) is due to the presence of a fully developed functional uterine hemi-cavity. Class U4 is divided into two sub-classes according to the existence or absence of a functional rudimentary cavity [6]:
- Class U4a or hemi-uterus with a rudimentary (functional) cavity characterised by the presence of a communicating or non-communicating contralateral functional horn.
- Class U4b or hemi-uterus without a rudimentary (functional) cavity.

Patients who have a unicornuate uterus with a rudimentary horn have an increased incidence of gynaecological problems and tend to present, at the time of menarche or later in their lives, with symptoms such as dysmenorrhoea and chronic pelvic pain [7]. While Nanda et al [3]. described a successful twin pregnancy in a unicornuate uterus with a fetus in the rudimentary non-communicating horn, there have been many other cases of rudimentary non-communicating horn rupture [8].
A unicornuate uterus with a rudimentary horn is linked to ectopic pregnancies and rudimentary horn rupture. While it is uncertain whether to remove the rudimentary horn before conception or early in pregnancy, resection improves obstetrical outcomes significantly. Patients with a unicornuate uterus are at a higher risk of obstetrical complications, including first trimester abortion, second trimester abortion, intrauterine growth restriction, preterm delivery, and intrauterine fetal death, even after resection of the rudimentary horn. Only a few of these risks can be reduced through pregnancy follow-up and specific interventions.
Ultrasound weight estimation is less accurate for breech fetuses due to uterine anomalies. Strategies to prevent preterm birth focus on measuring cervical length, which has a high predictive value of 92%. However, interventions aimed at delaying delivery in women for more than 24 to 48 hours have been unsuccessful. Ultrasound measurement of cervical length is a useful tool for assessing the risk of preterm birth. Cervical cerclage is the optimal therapy for women with a short cervix (<25mm>
Conclusion
Although women with unicornuate uterus have a poor reproductive result, they can still have a healthy pregnancy. Routine laparoscopic excision of the rudimentary horn should be performed during non-pregnant states, and such pregnancies should be monitored for the development of intrauterine growth retardation by serial ultrasound assessments of the estimated fetal weight and cervix length.
References
- Reichman DE, Laufer MR. (2010). Congenital uterine anomalies affecting reproduction. Best Practice & Research Clinical Obstetrics & Gynaecology, 24(2):193-208.
Publisher | Google Scholor - Nanda S, Dahiya K, Sharma N, Aggarwal D, Sighal SR, Sangwan N. (2009). Successful twin pregnancy in a unicornuate uterus with one fetus in the non-communicating rudimentary horn. Archives of gynecology and obstetrics, 280:993-995.
Publisher | Google Scholor - Thakur S, Sood A, Sharma C. (2012). Ruptured noncommunicating rudimentary horn pregnancy at 19 weeks with previous cesarean delivery: a case report. Case reports in obstetrics and gynecology, 2012(1):308-476.
Publisher | Google Scholor - Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, Gergolet M, et al. (2013).The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Human reproduction, 28(8):2032-2044.
Publisher | Google Scholor - Fedele L, Bianchi S, Zanconato G, Berlanda N, Bergamini V. (2005). Laparoscopic removal of the cavitated noncommunicating rudimentary uterine horn: surgical aspects in 10 cases. Fertility and sterility, 83(2):432-436.
Publisher | Google Scholor - Khati NJ, Frazier AA, Brindle KA. (2012). The unicornuate uterus and its variants: clinical presentation, imaging findings, and associated complications. Journal of Ultrasound in Medicine, 31(2):319-331.
Publisher | Google Scholor - Amritha B, Sumangali T, Priya B, Deepak S, Sharadha R. (2009). A rare case of term viable secondary abdominal pregnancy following rupture of a rudimentary horn: a case report. Journal of medical case reports, 3:1-3.
Publisher | Google Scholor - Norwitz ER, Caughey AB. (2011). Progesterone supplementation and the prevention of preterm birth. Reviews in obstetrics and gynecology, 4(2):60.
Publisher | Google Scholor - Chan Y, Jayaprakasan K, Tan A, Thornton J, Coomarasamy A, Raine‐Fenning N. (2011). Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound in Obstetrics & Gynecology, 38(4):371-382.
Publisher | Google Scholor - Reichman DE, Laufer MR. (2010). Congenital uterine anomalies affecting reproduction. Best Practice & Research Clinical Obstetrics & Gynaecology, 24(2):193-208.
Publisher | Google Scholor - Nanda S, Dahiya K, Sharma N, Aggarwal D, Sighal SR, Sangwan N. (2009). Successful twin pregnancy in a unicornuate uterus with one fetus in the non-communicating rudimentary horn. Archives of gynecology and obstetrics, 280:993-995.
Publisher | Google Scholor - Thakur S, Sood A, Sharma C. (2012). Ruptured noncommunicating rudimentary horn pregnancy at 19 weeks with previous cesarean delivery: a case report. Case reports in obstetrics and gynecology, 2012(1):308-476.
Publisher | Google Scholor - Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, Gergolet M, et al. (2013).The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Human reproduction, 28(8):2032-2044.
Publisher | Google Scholor - Fedele L, Bianchi S, Zanconato G, Berlanda N, Bergamini V. (2005). Laparoscopic removal of the cavitated noncommunicating rudimentary uterine horn: surgical aspects in 10 cases. Fertility and sterility, 83(2):432-436.
Publisher | Google Scholor - Khati NJ, Frazier AA, Brindle KA. (2012). The unicornuate uterus and its variants: clinical presentation, imaging findings, and associated complications. Journal of Ultrasound in Medicine, 31(2):319-331.
Publisher | Google Scholor - Amritha B, Sumangali T, Priya B, Deepak S, Sharadha R. (2009). A rare case of term viable secondary abdominal pregnancy following rupture of a rudimentary horn: a case report. Journal of medical case reports, 3:1-3.
Publisher | Google Scholor - Norwitz ER, Caughey AB. (2011). Progesterone supplementation and the prevention of preterm birth. Reviews in obstetrics and gynecology, 4(2):60.
Publisher | Google Scholor











