

Research Article
Spatial Analysis of The Occurrence of Malnutrition Among Under-Five Children in Egbelubi Ndashi Clan, Etche Local Government Area, Rivers State
1Department of Environmental Management, Faculty of Environmental Sciences, Rivers State University, Nkpolu-Oroworukwo, Port Harcourt, Nigeria.
2Surgical Out- Patient (SOP) Department, Rivers State University Teaching Hospital, Port Harcourt, Nigeria.
3Department of Geography and Environmental Management, Faculty of Social Sciences, University of Port Harcourt, Choba, Nigeria.
*Corresponding Author: MeeluBari Barinua Tsaro Kpang, Department of Geography and Environmental Management, Faculty of Social Sciences, University of Port Harcourt, Choba, Nigeria.
Citation: Imiete G., Umeh K.C., Kpang M.B.T. (2025). Spatial Analysis of The Occurrence of Malnutrition Among Under-Five Children in Egbelubi Ndashi Clan, Etche Local Government Area, Rivers State, International Journal of Clinical and Surgical Pathology, BioRes Scientia Publishers. 1(1):1-10. DOI: 10.59657/3067-0462.brs.25.010
Copyright: © 2025 MeeluBari Barinua Tsaro Kpang, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 16, 2024 | Accepted: February 20, 2025 | Published: March 12, 2025
Abstract
Malnutrition is one of the major issues confronting children below the age of five in Nigeria. It is directly or indirectly responsible for 45 per cent of all fatalities in children under the age of five with other significant long term developmental, economic, social, and medical effects for people, families, communities, and governments. Its occurrence among children under the age of five vary intensely across rural and urban locations. The aim of this study was to examine the occurrence of malnutrition among under-five children in Egbelubi-Ndashi, in Etche Local Government Area of Rivers State. A total of 316 mothers of under-five children spanning across 4320 households participated in the study after been screened in line with WHO criteria of body mass index (BMI) to affirm malnourishment, underweight or wasting and using a mean prevalence of 29.0% for underweight in under-five children as provided by National Population Commission. The data was imported into the ARCGIS 10.7.1 environment where it was manipulated through standard procedures to produce the Inverse Distance Weighted (IDW) spatial interpolation map of occurrence of malnutrition in the area. ANOVA was employed to test the variation in the occurrence of malnutrition among under-five age children in the sampled compounds in the area. The results revealed the presence of malnutrition among children of under five in all the sampled compounds with significant variation across the area (F= 9.104505; P= 3.7690; Fcrit = 2.641465). The spatial distribution of malnutrition in the area indicates Umuorashi (35%), Umueke (23%), Umuodemene (18%), Umuisiguzor (14%) and Umuokoro (10%). Arising from the findings, increased knowledge and display of hygiene and nutrition practices by mothers, adequate household food security by household heads, increased women education and constant enlightenment of women/mothers and reduction in family size were strongly recommended.
Keywords: malnutrition; under-five; enlightenment; prevalence; women
Introduction
Nutrition is the systematic building and organization of the knowledge that interprets the interaction of nutrients and other food substances that relates to growth, maintenance, reproduction, health and disease of an organism, which encompasses food intake, absorption, assimilation, biosynthesis, catabolism and excretion (Joint Collection Development Policy, 2014). The food eaten by an individual depends on availability within the environment and palatability of the food in itself. Therefore, it is the totality of the outcome of what is taken as food, how the body responds to it and how this affects the body. On account of the essential role nutrition plays in the overall development of an individual, it forms a critical component of health policies in most countries and recognized as a fundamental target to be achieved in the 2030 agenda for sustainable development to supports the immediate need to advance actions in mainstreaming disaster risk reduction in alignment with the fact that a healthy nutrition is considered to guarantee a healthy individual, and by extension, a successful economy and nation. Malnutrition is the outcome of an eaten food, in which the nutrients are either too low, low, high or too high, such that it results in health problems (United Nations Children Fund, 2010). When the nutrients are inadequate, under-nutrition occurs, while over-nutrition results from too much nutrient intake. It is defined by Etim, Ejemor-Nwadiaro & Kalu (2017) as the intake of dietary nutrients by an individual or organism either insufficiently or exclusively. However, most principles of malnutrition are founded on the concept of under-nutrition (Young, 2012).
Malnutrition is defined by Saunders, Smith & Stroud (2011) as the deficiency, imbalance or excess of nutrition, which subsequently results in measurable adverse effects in body composition, function and clinical outcome. The severity determines the kind of adverse effect manifested. In prolonged malnutrition, the consequences impact on the physical wellbeing and health of the child, and can present as delayed physical growth and motor development, low intelligence quotient, increase in behavioural problems, susceptibility to microbial infections and deficient social skills (Food and Agricultural Organization, 2012; Black, Morris & Jennifer, 2013). In interaction with infections, malnutrition is reported to be the major cause of infant mortality in most countries (Black et al., 2008). Malnutrition can also occur, if the adequate and appropriate nutrients, calories and protein are taken by an individual, but the body fails to utilize (assimilate) it, thus leading to a condition referred to as under-nutrition (Rahman, Alli & Ahmed, 2017). The condition is mostly linked to poverty and hunger, and is also commonly associated with infections, due to suppression of the immune system. There are about 925 million hungry people globally (John et al., 2012), while a good number of people are also living below the poverty line, and all these contribute to malnutrition. Malnutrition is reported to be associated with immunosuppression. It also exposes children to a greater risk of contracting common infections, increased susceptibility to other infections and delays recovery from infections and other illnesses (Charles, Didia & Okerengwo., 2016). It has been reported by the UNICEF/WHO/World Bank (2016) that in the first 1,000 days of a child’s life, poor nutrition (malnutrition) can cause stunting of growth, which cannot be reversed, in addition to other physical and mental impairments like poor cognitive function and reduced physical, social and mental productivity.
There are indications that one out of every thirteen children in the world is stunted in growth, while about sixteen (16) million children are wasting respectively, worldwide whereas in specific terms 60% of under-five children mortality rates in sub-Saharan Africa (SSA) are attributed to malnutrition in children with poor school performance, increased school absenteeism, reduced intellectual achievement, delayed cognitive development and increased disease morbidity and mortality as common effects of the this debilitating condition in children younger than five years old (Glewwe et al., 2001; Kandala et al., 2011; UNICEF/WHO/World Bank, 2015).
Malnutrition can be mild, moderate or severe, in pregnancy and early life, malnutrition may result in permanent impairment of physical and mental development, while the extreme condition (starvation) can result in short stature, thin body, low energy levels, swollen legs, susceptibility to infections and cold, and swollen abdomen (UNICEF, 2010). Black et al., (2008) posits that severe malnutrition in children leads to an impaired cognitive growth and development, with an attendant effect on the general wellbeing of the individual as age progresses. Malnutrition is often associated with poverty and is responsible for about a third of all infant and child mortality, particularly, in developing countries such as Nigeria ((Bryce et al., 2005; Muller & Krawinkel, 2005). Malnutrition is an epidemic common in different regions of the world, but more prevalent in some than others. On the other hand, Africa and Asia are two regions of the world with high burden of malnutrition, especially, among children that are younger than five years old (Kalu & Etim, 2018). The World Health Organization (1999) as cited in Alemu (2013) posits that malnutrition remains one of the commonest causes of morbidity and mortality, especially, among children globally. The disease condition is also reported to be responsible for one-third of the 7.6 million child deaths that occur yearly in under five children (Alemu, 2013), with two-thirds of these deaths occurring in children before their first birthday and due to improper feeding practices (WHO, 2002). Investigative report shows that there are about 162 million children that are malnourished globally, thus resulting in stunted growth, of which Africa has 36% while Asia has 56% (UNICEF/World Bank, 2012).
Malnutrition according to Saunders, Smith & Stroud (2011) is the deficiency, imbalance or excess of nutrition, which subsequently results in measurable adverse effects in body composition, function and clinical outcome. The severity determines the kind of adverse effect manifested. In prolonged malnutrition, the consequences impact on the physical wellbeing and health of the child, and can manifest its presence as delayed physical growth and motor development, low intelligence quotient, increase in behavioural problems, susceptibility to microbial infections and deficient social skills (Food and Agricultural Organization, 2012; Black, Morris & Jennifer, 2013). On a global scale, malnutrition and poor sanitation accounts for about half of all deaths in under-five children (UNICEF, 2012) and it is reported by Black et al. (2008) as the major cause of infant mortality in most countries. Malnutrition can also occur, if the adequate and appropriate nutrients, calories and protein are taken by an individual, but the body fails to utilize (assimilate) it, thus leading to a condition referred to as under-nutrition (Rahman, Alli & Ahmed, 2017). The condition is mostly linked to poverty and hunger, and is also commonly associated with infections, due to suppression of the immune system. There are about 925 million hungry people globally (John et al., 2012), while a good number of people are also living below the poverty line, and all these contribute to malnutrition. According to Charles, Didia & Okerengwo (2016), malnutrition is associated with immune suppression. It also exposes children to a greater risk of contracting common infections, increased susceptibility to other infections and delays recovery from infections and other illnesses. Similarly, it is reported by Victoria et al. (2008) that about 60 million children are stunted in growth due to malnutrition, globally, of which 11 million are Nigerians. This report highlights the magnitude of malnutrition in Nigeria, as it contributes approximately 12% of the global prevalence of the condition. A similar finding on nutritional status reveals that as at 2012, an estimated 165 million children are stunted, while 99 million are underweight and 51 million are wasting (Endris et al., 2017). This has brought about several forms of impairment in the life and activities of children including poor school performance, increased school absenteeism, reduced intellectual achievement, delayed cognitive development and increased disease morbidity and mortality and specifically responsible for about 3.1 million deaths of under-five children annually (Glewwe et al., 2001; Black et al., 2013). Malnutrition is a global health burden affecting a significant number of the world’s population but more prevalent in developing countries and particularly common among children of less than five years of age. Several investigators have attempted to explore the cause of this burden, with explanations regarding poor nutrition and other factors such as income and environment. This study was therefore initiated since there is no known work with specific interest in the knowledge of the burden in the area coupled with the fact that several activities of miscreants, militancy and crisis, which encourages the occurrence of malnutrition, is a common feature of Egbelubi Ndashi clan of Etche community in River’s state. Meanwhile, the principal objectives of the study include to identify the factors responsible for malnutrition among under-five age children in the locality; examine the effect of malnutrition on the children, map the occurrence of malnutrition among under-five children in the area and statistically verify if there is variation in occurrence of malnutrition across the study area.
Methodology
The study was conducted in Egbelubi Ndashi community in Etche local government area of Rivers state. It is a typical farming community that speaks Etche dialect (a fusion of Ikwerre and Ibo dialects). Other than farming, some members of the community are civil servants (working either at the local government council or state ministries) and traders (mainly dealing on farm produce, household items, clothing and tools for agriculture). It is located in the north-western part of Rivers state, south-south Nigeria, and is bounded on the north by Imo state, west by Omoku community in Ogba/Egbema/Ndoni local government area and on the south-east by Ikwerre local government. The community has good network of roads, power supply from the national grid, water supply for consumption and other uses from streams and underground water sources like borehole and mono-pumps. The community is made up of sixteen compounds (Umueke, Umunwachukwu, Umuodemene, Umuokwu, Umuorashi, Umuiwezor, Umuisiguzor, Umunwaugha, Umuonyegbule, Umunwankom, Umuokoro, Nwaorgu, Nkwocha, Eke, Umulor, Nwakopi), with an estimated total of 13,480 households. The population for this study comprised mainly of mothers of children under-five years of age in every household selected. The children were first examined and certified to fulfill the WHO criteria of body mass index (BMI) to affirm malnourishment, underweight or wasting before their mothers were considered eligible and allowed to participate in this study. Meanwhile, the sample size for this study was determined by using a mean prevalence of 29.0% for underweight under-five children as provided by National Population Commission (NPC, 2013) and applying the formular adapted from ((Kirkwood & Sterne, 2006).

n= sample size, z= standard (1.96), p= prevalence, q= 1- prevalence, d= degree of accuracy (0.05).


N= 316.40 = 316
The balloting method was used to randomly select five compounds representing 30% of the total compounds in the clan. Furthermore, the population of each of the sampled compounds was divided by six (6) which is standard household size approved by the National population commission in order to determine the number of households. The number of households in each of the selected compounds was further divided by the total number of households and multiplied by the 316 obtained by applying the formula adapted from ((Kirkwood & Sterne, 2006) to proportionally derive the sample size. Thus, a total of Three Hundred and Sixteen copies of structured and validated questionnaires were designed and administered to only mothers of under-five aged children in the sampled compounds in order to generate valid information for the study. Meanwhile, ANOVA was employed to test variation in the occurrence of malnutrition among under-five age children in the sampled compounds in the area. On the other hand, the acquired data was imported into the ARCGIS10.7.1 environment and appropriately manipulated following the steps listed in figure 2 to produce the Inverse Distance Weighted (IDW) spatial interpolation map showing the spatial distribution and pattern of occurrence of malnutrition in the area.
Table 1: Selected Compounds in the Clan.
| Compounds | Population (P) | Households (P:6) | Sample Size |
| Umueke | 1000 | 167 | 73 |
| Umuodemene | 800 | 133 | 58 |
| Umuorashi | 1500 | 250 | 110 |
| Umuisiguzor | 600 | 100 | 44 |
| Umuokoro | 420 | 70 | 31 |
| Total | 4320 | 720 | 316 |
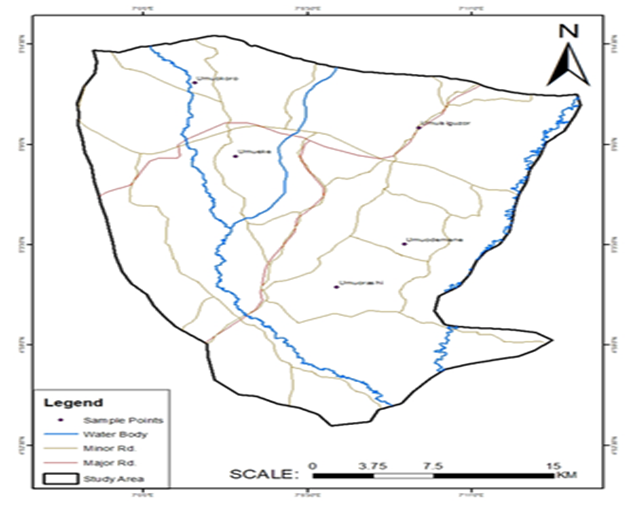
Figure 1: Sampled Compounds in the study area.
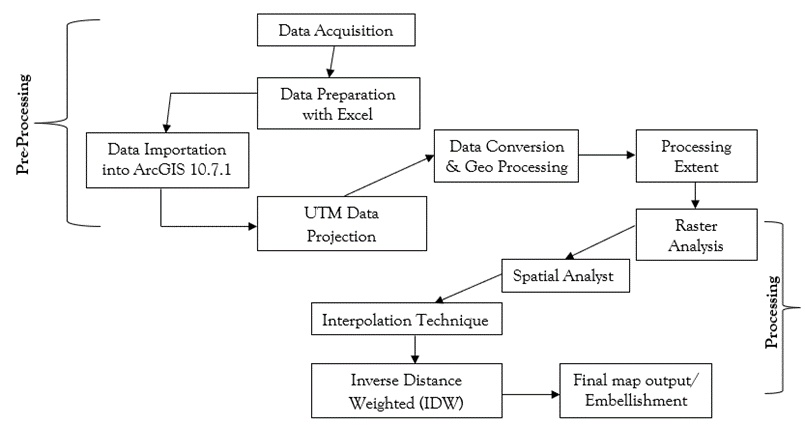
Figure 2: Flow chart for interpolation using inverse distance weighted.
Table 2: Socio-demographic characteristics of the respondents.
| Age | |||||
| Compounds | lessthan 30 | 31-40 | 41-50 | >50 | Total |
| Umueke | 17 | 27 | 17 | 12 | 73 |
| Umuodemene | 15 | 18 | 20 | 5 | 58 |
| Umuorashi | 18 | 49 | 32 | 10 | 110 |
| Umuisiguzor | 12 | 22 | 7 | 4 | 44 |
| Umuokoro | 5 | 11 | 8 | 7 | 31 |
| Total | 67 | 127 | 84 | 38 | 316 |
| Percentage (%) | 21 | 40 | 27 | 11 | 100 |
| Education | |||||
| Compounds | None | Primary | Secondary | Tertiary | Total |
| Umueke | 25 | 19 | 17 | 12 | 73 |
| Umuodemene | 23 | 18 | 13 | 4 | 58 |
| Umuorashi | 44 | 32 | 24 | 10 | 110 |
| Umuisiguzor | 12 | 14 | 8 | 10 | 44 |
| Umuokoro | 6 | 9 | 9 | 7 | 31 |
| Total | 110 | 92 | 71 | 43 | 316 |
| Percentage (%) | 35 | 29 | 22 | 14 | 100 |
| Occupation | |||||
| Compounds | Student | Petty Trading | Employed | Skilled Worker | None |
| Umueke | 6 | 28 | 11 | 18 | 10 |
| Umuodemene | 1 | 32 | 4 | 17 | 4 |
| Umuorashi | 5 | 52 | 10 | 28 | 15 |
| Umuisiguzor | 1 | 23 | 8 | 10 | 2 |
| Umuokoro | 2 | 10 | 3 | 12 | 4 |
| Total | 15 | 145 | 36 | 85 | 35 |
| Percentage (%) | 5 | 46 | 11 | 27 | 11 |
| Marital Status | |||||
| Compounds | Single | Married | Separated | Co-habiting | Total |
| Umueke | 32 | 17 | 15 | 9 | 73 |
| Umuodemene | 25 | 20 | 4 | 9 | 58 |
| Umuorashi | 48 | 28 | 21 | 13 | 110 |
| Umuisiguzor | 15 | 9 | 13 | 7 | 44 |
| Umuokoro | 10 | 8 | 8 | 5 | 31 |
| Total | 130 | 82 | 61 | 43 | 316 |
| Percentage (%) | 41 | 26 | 19 | 14 | 100 |
| No of Children | |||||
| Compounds | None | 1 | 2-5 | >5 | Total |
| Umueke | - | 18 | 42 | 7 | 73 |
| Umuodemene | - | 21 | 38 | 4 | 58 |
| Umuorashi | - | 20 | 48 | 12 | 110 |
| Umuisiguzor | - | 17 | 44 | 7 | 44 |
| Umuokoro | - | 13 | 20 | 5 | 31 |
| Total | - | 89 | 192 | 35 | 316 |
| Percentage (%) | - | 28 | 61 | 11 | 100 |
The Socio-demographic characteristics of the respondents in the area is presented in Table 2 and it reveals that 21% of the mothers of under-five aged children in the area are less than 30 years of age, 40% are within the ages of 31-40 whereas 27% are in the age bracket of 41-50 while 11percentage fall in the group above 50 years. The table also revealed the ages of the respondents as follows: those who had no formal education constituted 35% of the population while 29% had primary education, 22% had secondary education and 14% of the mothers of under-five children involved in the study had post-secondary education. The marital status of the respondents was not left out of the picture. Thus, it is evidently shown in Table 2 amongst other socio-demographic characteristics that a total of 41% of the respondents were singles whereas 26% of them were married. Similarly, it was also revealed that 19% of the populations were already separated while those who were co-habiting constituted exactly 14% of the population. On the other hand, it was clearly observed that 5% of the mothers of under-five children in the area under investigation were students while 46% of the entire populations were involved in petty trading. From the table, it is obviously noted that only 11% of the women considered in this study in the area were gainfully employed, 27% were skilled workers and another 11% had no identifiable occupation as a means of livelihood. In terms of the number of children per household, it was observed that 28% of the respondents had only 1 child while majority of the participants were noted to be in the category of 2-5 children as these recorded 61% of the total respondents while those who had above 5 children formed only 11%.
Table 3: Occurrence/Factors associated with malnutrition in under-five children.
| Compounds | Umueke | Umuodemene | Umuorashi | Umuisiguzor | Umuokoro | Total |
| Causal Factors | ||||||
| Child Factors | 8 | 10 | 19 | 6 | 4 | 47 |
| Maternal Factors | 10 | 11 | 17 | 8 | 3 | 49 |
| Family size | 12 | 7 | 22 | 11 | 4 | 56 |
| Household Income & Expenditure | 11 | 3 | 15 | 6 | 5 | 40 |
| Poverty | 10 | 8 | 17 | 5 | 6 | 46 |
| Household Food Security | 7 | 5 | 9 | 3 | 3 | 27 |
| Socio- Demographic Factors | 10 | 6 | 8 | 2 | 4 | 30 |
| Educational Status | 5 | 8 | 3 | 3 | 2 | 21 |
| Total | 73 | 58 | 110 | 44 | 31 | 316 |
In Table 3, the factors responsible for malnutrition are listed and it is revealed that child factors which include the position of a child in the family, sex, age and diseases is responsible for 15% of malnutrition in the study area while another 15% was caused by maternal factors. Again, the study unveils that 18% of malnutrition observed among under–five aged children in the area is actually caused by family size whereas household income and expenditure cause 13% of malnutrition in the area. Poverty is another major causative factor of malnutrition in the area and it is responsible for 14% of the problem under investigation. Other factors identified include household food security (9%), socio-demographic (9%) and educational status (8%). Conversely, the study also shows that 23% of the problem under investigation was observed in Umueke and 18% in Umuodemene. Notably, the study revealed that 35% of malnutrition among under-five aged children in the area was domiciled in Umuorashi. The lowest percentage of malnutrition recorded in the area was 14% and 10% in Umuisiguzor and Umuokoro respectively. Following the report of United Nation’s Children Fund (UNICEF) (2017), the factors responsible for the occurrence of malnutrition in infancy and childhood include poor psychological care, neglect of the child, child abuse, trauma and stress which are normally grouped as follows: educational status, socio-demographic factors, poverty, household food security, household income and expenditure, Family size, maternal factors and child factors. Nutrition embodies the entirety of food consumed and the nutrient made available by it for the proper functioning of the body. For the body to function optimally, the nutrition must be balanced and healthy. For children, this is more important due to the development of certain physiological processes that will determine the cause of their life, such as the proper development of the brain and other body organs. The effect of this on the child, according to the Food and Agricultural Organization (2008) and Akinyele (2009) is poor academic performance, physical and mental ii-health, psychosocial problems and anaemia, resulting from deficiency of iron in the body. Similarly, Reutlinger & Selowsky (1976), as cited in Kalu & Etim (2018) posits that family income has an effect on the caloric and protein intake of a house, infants and children inclusive. This can determine the child’s nutritional status.
Table 4: The effects of malnutrition in under-five children.
| Effects | Umueke | Umuodemene | Umuorashi | Umuisiguzor | Umuokoro | Total |
| Stunted growth / Small stature | 18 | 12 | 32 | 8 | 7 | 77 |
| Poor sight | 13 | 9 | 15 | 10 | 8 | 55 |
| Fluffy/yellowish hair | 12 | 8 | 12 | 2 | 2 | 36 |
| Reduced intelligence quotient | 8 | 10 | 13 | 11 | 4 | 46 |
| Loss of memory | 10 | 6 | 16 | 6 | 2 | 40 |
| Poor communication skills | 5 | 4 | 12 | 5 | 6 | 32 |
| Poor physical development | 7 | 9 | 10 | 2 | 2 | 30 |
| Total | 73 | 58 | 110 | 44 | 31 | 316 |
The effect of malnutrition in the area is presented in Table 4 and 24% of the respondents confirmed that stunted growth/small stature is a major effect of malnutrition among children of under-five in the area whereas 17% of the people opted for poor sight as a fundamental effect of this health burden in the area. On the other hand, 11% of them said fluffy/yellowish hair is the principal effect associated with this health problem while 15% opted for reduced intelligent quotient. The opinion of the respondents varied greatly across the area as another 13% of the people believed that loss of memory is a visible effect of malnutrition among children of under-five in the area while poor communication skills and poor physical development was identified by 10% and 9% of the respondents respectively as the evidence of malnutrition in the area. Malnutrition prevents children from attaining their full potential, mental and physical (Kandala, Madungu, Emina, Nzita & Cappuccio, 2011), with a visible dysfunction in health (Victoria, Adair, Fall, Hallal, Martorell, Richter & Sachdev, 2008). Reports from investigations are that malnutrition in early age can result in decreased educational achievement, decreased labour productivity and increased risk of being susceptible to chronic infections later in life (Black et al., 2013). Malnutrition can result in diseases like marasmus, kwashiorkor, anaemia, goiter, hypernatremia, hypokalemia and deficiency of some important vitamins (Grover & Eels, 2009). The effects of malnutrition are mostly not immediate. The condition may have been managed but the effect persists into later life, and the nature and severity of the effect is determined by the severity and magnitude of the disease condition. The effects of malnutrition among under-five children, however, as reported by Babatunde (2011) include poor school performance, absenteeism from school, reduced intellectual achievement, poor physical development (stunting) delayed cognitive development morbidity and mortality. According to UNICEF (2017) poor physical development is identified as a major effect of malnutrition following the fact that poor development is all-encompassing and affects every body region for which the brain is an integral part. If the brain does not develop properly due to malnutrition, it is expected that mental capacity will also be reduced, which may also impair communication skills and sight. It is common science-based knowledge that the brain is the coordinator of almost all functions of the body, especially, those that have to do with the senses.
Table 5: Variation in Malnutrition Occurrence in the area.
| ANOVA | ||||||
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 464.85 | 4 | 116.2125 | 9.104505 | 3.7690 | 2.641465 |
| Within Groups | 446.75 | 35 | 12.76429 | |||
| Total | 911.6 | 39 |
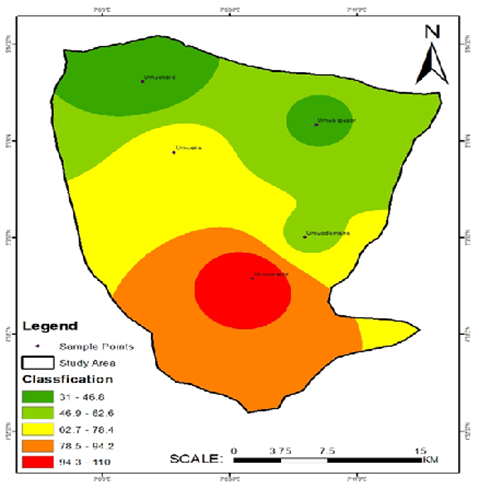
Figure 3: Spatial Distribution and Pattern of Occurrence of Malnutrition in the area.
Prevalence of Malnutrition in Under-Five Age Children in The Area
Malnourishment is a global issue with complications which include susceptibility to infections and results in significant number of deaths among children especially in developing countries such as Nigeria. It is reported by the National Population Commission (2013) that the pattern of malnutrition in the country has steadily increased over the last decade and half with increase in the severity of childhood malnutrition from 11% in 2003 to 18% in 2013 for wasting; 4% in 2003 to 29% in 2013 for underweight, while there was a decline from 42% in 2003 to 37% in 2013 for children who were stunted. The occurrence and prevalence of malnutrition in the area under investigation is reported in Figure 2 and it is evident from that malnutrition was observed among under five children in all the selected compounds where this study was conducted. According to report by Yanusa et al., (2012) approximately 49% of absenteeism from school in children less than five years is reported to affect about 42% of the children. This huge loss to the society, even though this age group may not be considered to contribute directly to the economic output of the country, has its toll indirectly by affecting the caregivers that cater for these children. The factors identified which accounts for the occurrence and prevalence of malnutrition in the area aligns with the claims of Babatunde et al. (2007), Aliyu et al. (2012), Ejemot et al. (2015) and Hernel et al. (2015) which posits that the factors that affect nutritional status in under-five children include poverty, failure to breastfeed infants exclusively, poor nutrition and lack of appropriate weight gain during pregnancy, illnesses like diarrhoea and acute respiratory infections, inadequate vitamins supplement or fortified food consumption, poor sanitation, large family size, lack of information and education about proper or adequate nutrition, and food security and safety. Therefore, it is pertinent to address these issues to avert the dire consequences associated with this health burden in the area since it is common science-based knowledge that the brain is the coordinator of almost all functions of the body, especially, those that have to do with the senses. If the brain does not develop properly due to malnutrition, it is expected that mental capacity will also be reduced, which may also impair communication skills and sight as poor development is all-encompassing and affects every body region, to which the brain is a part. Meanwhile, the occurrence of malnutrition among children of under five in the area is very obvious in all the compounds whereas its distribution and prevalence are reported in Umuorashi (35%), Umueke (23%), Umuodemene (18%), Umuisiguzor (14%) and Umuokoro (10%) indicating that the problem varies significant across the study area with (F= 9.104505; P= 3.7690; Fcrit = 2.641465) as displayed in table 5.
Conclusion and Recommendations
This study examined the occurrence of malnutrition in under-five children and clearly establishes the manifestation of pockets of malnutrition in under-five aged children in the area with stunted/small stature, poor sight, fluffy/yellowish hair, reduced intelligence quotient, loss of memory, poor communication and physical development as common effects of this debilitating condition. Arising from the findings of this study, increased knowledge and display of hygiene and nutrition practices by mothers, adequate household food security by household heads, increased women education should be encouraged, constant enlightenment of women/mothers on the effect of this health burden and reduction in family size were recommended as ways of overcoming this devastating health problem in our localities.
References
- Akinyele, O. (2009). Ensuring Food and Nutrition Security in Rural Nigeria: An Assessment of The Challenges, Information Needs, and Analytical Capacity. IFPRI-NSSP.
Publisher | Google Scholor - Alemu, F. (2013). Assessment of the Impact of Malnutrition on Children at Dilla Referral Hospital and Unity Pediatric Clinic, Ethiopia. Internal Journal of Nutrition and Metabolism. 5(6):105-113.
Publisher | Google Scholor - Aliyu, A., Oguntunde, O., Dahiru, T., Raji, T. (2012). Prevalent and Determinants of Malnutrition Among Pre-School Children in Northern Nigeria. Pakistan Journal of Nutrition.11(11):1092-1095.
Publisher | Google Scholor - Babatunde, O., Omotesho, A., Sholotan, S. (2007). Socio-Economic Characteristics and Food Security Status of Farming Households in Kwara State, North-Central Nigeria. Pakistan Journal of Nutrition. 6:49-58.
Publisher | Google Scholor - Babatunde, R., Olagunju, F., Fakayo, S., Sola-Ojo, E. (2011). Prevalence and Determinants of Malnutrition Among Under-Five Children of Farming Households in Kwara State, Nigeria. Journal of Agricultural Science. 3(3):176-181.
Publisher | Google Scholor - Baranwal, K., Gupta, M., Mishra, N., Prakashs, N., Pandey, N. (2010). Factors Influencing the Nutritional Status of Under-Five (1-5years) Children in Urban-Slum Area of Varanasi. Indian Association of Preventive and Social Medicine. Uttar Predesh and Uttarakhand State Chapter.
Publisher | Google Scholor - Black, R., Morris, S., Jennifer, B. (2013). Where and why are 10 million Children Dying Every Year? The Lancet. 361:2226-2234.
Publisher | Google Scholor - Black, R., Allen, H., Bhutta, Z., Caulfield, E., De Onis, M., et al. (2008). Maternal And Child Under Nutrition: Global and Regional Exposures and Health Consequences. Lancet. 371(9608):243-260.
Publisher | Google Scholor - Bryce, J., Boschi-Pinto, C., Shinbuya, K. And Black, E. (2005). WHO Estimates of The Causes of Death in Children? Lancet. 365(9465):1147-1152.
Publisher | Google Scholor - Charles, A., Didia, B., Okerengwo, A. (2016). Immunophenotyping of Human Immunodeficiency Virus-Infected Patients with Mycobacterium Tuberculosis Co-Infection. British Journal of Medicine & Medical Research. 17(6):1-9.
Publisher | Google Scholor - Endris, N., Asefa, H., Dube, L. (2017). Prevalence of Malnutrition and Associated Factors Among Children in Rural Ethiopia. Bio-Medical Research International. 6587853.
Publisher | Google Scholor - Etim, D., Ejemot-Nwadiaro, R., Kalu, E. (2017). A Study of Malnutrition-Dependent Factors Among Under-Five Children in Ekureku Community, Abi Local Government Area of Cross River State, Nigeria. British Journal of Medicine and Medical Research. 21(8):1-10.
Publisher | Google Scholor - Food And Agricultural Organization. (2012). State Of Food Insecurity in The World, Food Security Statistics.
Publisher | Google Scholor - Glewwe, P., Jacoby, G., King, M. (2001). Early Childhood Nutrition and Academic Achievement: A Longitudinal Analysis. Journal of Public Economics. 81(3):345-368.
Publisher | Google Scholor - Grover, L., Eels, C. (2009). Protein Energy Malnutrition, Paediatric Cline, North America., 56(5):1055-1068.
Publisher | Google Scholor - John, H., Rosegrant, M., Torero, M. (2012). Hunger And Malnutrition. 68.
Publisher | Google Scholor - Joint Collection Development Policy. (2014). Human Nutrition and Food. National Library of Medicine. National Institutes of Health.
Publisher | Google Scholor - Kalu, R., Etim, K. (2018). Factors Associated with Malnutrition Among Under-Five Children in Developing Countries: A Review. Global Journal of Pure and Applied Sciences. 24:69-74.
Publisher | Google Scholor - Hernel, C., Enne, J., Omer, K., Ayara, N., Yarima, Y., et al. (2015). Childhood Malnutrition Is Associated with Maternal Care During Pregnancy and Childbirth: A Cross-Sectional Study in Bauchi and Cross River States, Nigeria. Journal of Public Health Research. 4(1):139-148.
Publisher | Google Scholor - Kandala, N., Madungu, T., Emina, J., Nzita, K., Cappuccio, F. (2011). Malnutrition Among Children Under the Age of Five in The Democratic Republic of Congo (DRC): Does Geographic Location Matter? BMC Public Health. 11:261.
Publisher | Google Scholor - Muller, O., Krawinkel, M. (2005). Malnutrition And Health in Developing Countries. Canadian Medical Association Journal. 173(3):279-286.
Publisher | Google Scholor - National Population Commission of Nigeria (2013). Nigerian Demographic and Health Survey, Abuja, Nigeria.
Publisher | Google Scholor - Rahman, M., Ali, M., Ahmed, F. (2017). Contributing Factors to Under-Five Child Malnutrition in Rural Bangladesh. Juniper Online Journal of Case Studies. 4:1.
Publisher | Google Scholor - Saunders, J., Smith, T., Stroud, M, (2011). Malnutrition And Under Nutrition. Medicine. 39(1):45-50.
Publisher | Google Scholor - United Nations Children’s Fund. (2010). Facts of Life, 61-75.
Publisher | Google Scholor - United Nations Children Fund. (2012). Millennium Development Goals, Goal 4: Reduce Child Mortality.
Publisher | Google Scholor - United Nations Children’s Fund/World Health Organization/World Bank Group. (2015). Joint Child Malnutrition Estimates: Levels and Trends in Child Malnutrition.
Publisher | Google Scholor - United Nations Children’s Fund/World Health Organization/World Bank (2017). Joint Child Malnutrition Estimates 2017 Edition.
Publisher | Google Scholor - Victoria, G., Adair, L., Fall, C., Hallal, C., Martorell, R., et al. (2018). Maternal And Child Under Nutrition: Consequences for Adult Health and Human Capital. Lancet. 371(9609):340-357.
Publisher | Google Scholor - World Health Organization (2013). Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition. WHO Document Publications Services, Geneva, Switzerland.
Publisher | Google Scholor - Young, M. (2012). Food And Development. Abingdon, 36-38.
Publisher | Google Scholor - Yunusa, I., Gumel, H., Adegbusi, S. (2012). School Feeding Program in Nigeria: A Vehicle for Nourishment of Pupils. The African Symposium: Online Journal of The African Educational Research Network. 12;2.
Publisher | Google Scholor














