

Case report
Single Coronary Presenting with Acute Coronary Syndrome-Ptca through Trans-Radial Route
- Rajeev Bhardwaj *
- Sivaji Patibandla
- Gaurav Aggrawal
- Mehroj Mirza
Department of cardiology, MM Institute of Medical Sciences and Research, Mullana, Ambala, India.
*Corresponding Author: Rajeev Bhardwaj, Department of cardiology, MM Institute of Medical Sciences and Research, Mullana, Ambala, India.
Citation: R Bhardwaj, S Patibandla, G Aggrawal, M Mirza. (2023). Single Coronary Presenting with Acute Coronary Syndrome- Ptca through Trans-Radial Route. Clinical and Medical Images. 1(1); DOI: https://www.doi.org/brs/2023/cmi/0001
Copyright: © 2023 Rajeev Bhardwaj, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 05, 2022 | Accepted: December 26, 2022 | Published: January 06, 2023
Abstract
Isolated single coronary artery is a rare congenital anomaly occurring in approximately 0.024% of the population. It is usually diagnosed incidentally during coronary artery angiograms or on postmortem evaluations. The single coronary artery anomaly is usually asymptomatic, but may present as myocardial ischemia, syncope or sudden cardiac death depending on its course and the presence and severity of atherosclerosis.
Keywords: coronary single coronary anomalies; artery; PTCA
Introduction
Case: 62 years male patient was admitted in internal medicine department with acute inferior wall myocardial infarction (MI) around one month back. He was treated on medical therapy. He remained admitted for five days. There was no complication. He was not offered invasive therapy. He was discharged on 6th day with advice to follow up in cardiology out patient department (OPD) after one month. After two weeks, he started having angina on routine activities. Severity of pain increased over next two days, when he had episodes of rest pain, lasting few minutes. He was admitted in Cardiology. His ECG showed T wave inversion in leads II, III and AVF. Echocardiography showed hypokinetic inferior with ejection fraction of 55%. He was taken up for coronary angiography through trans radial route. We were not able to hook left coronary artery (LCA). After struggling for around 2-3 minutes, we gave sinus injection, but still LCA was not visible. We then did right coronary angiography. We found single coronary artery arising from right coronary sinus, which showed total occlusion after giving rise to left main coronary artery, which then devided into left anterior descending (LAD) and left circumflex (LCx) arteries (Fig 1). There was retrograde filling of distal right coronary artery (RCA) form LCA. Patient was taken up for percutaneous transluminal coronary angioplasty (PTCA).

Figure 1: Single coronary artery of RCA type, showing total occlusion after giving rise to left main coronary artery
Judkinn’s right could not properly hook the coronary artery, and so Amplatzer right (AR) guiding catheter was used. Lesion crossed with balanced middle weight miracle 3 wire (Fig. 2). Tandom dilatations were done with 2.0X10 mm balloon (Fig 3). There was good flow (Fig 3,4) 3.0X15 mm stent was deployed. there was some narrowing proximal to the stent. 3.0X12 mm stent was deployed proximal to the first stent. (Fig 5). There was no residual stenosis, with TIMI 3 flow (Fig. 6).
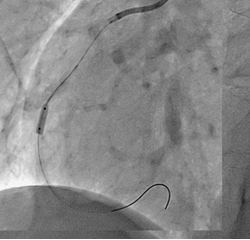
Figure 2: Balloon dilatation after crossing the lesion with Miracle 23 guide wire.

Figure 3: Good flow after balloon dilatation.
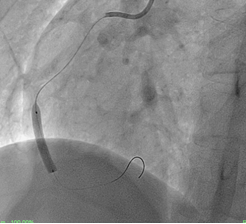
Figure 4: Final result after implanting two stents, showing no residual stenosis.
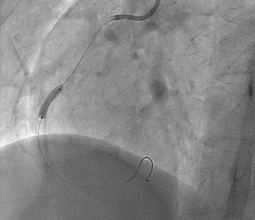
Figure 5
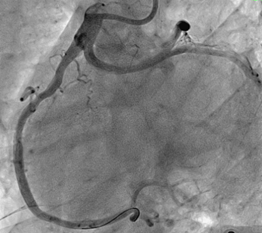
Figure 6
Discussion
Most coronary artery anomalies are asymptomatic and are usually encountered as coincidental findings during coronary angiography or autopsy [1]. Coronary arteries originating from a single coronary ostium in the aorta are rare, occurring in less than 0.03% of the general population [2]. The first report of a single coronary artery was by Hyrtl in 1841 [3]. Anomalies are classified according to the relation of the coronary anomaly to the aorta and pulmonary artery-that is, anterior, between, septal, posterior, and combined. Previous investigation of coronary anomalies and analysis of the causes of sudden cardiac death has identified the course of the left main coronary artery between the aorta and pulmonary artery as a potential cause of significant coronary ischaemia [1,2]. This anomaly can present with exertional angina, dyspnoea, and palpitations, as well as sudden death. There are several proposed potential mechanisms for the clinical manifestation of this anomaly, such as compression of the left coronary artery between the aorta and pulmonary artery during exercise when the vessels become enlarged; and compromise of the lumen of the left coronary artery due to the acute angle formed at its origin from the right aortic sinus resulting in a slit-like orifice. Horan et al reported SCA in father and daughter, raising the possibility of genetic link [4].
Lipton et al. [5] originally proposed the angiographic classification of SCA, which was later modified by Yamanaka et al. [6]. This classification takes into account the origin of the ostium from the sinus of Valsalva, anatomical course of the vessel, and the course of the transverse trunk. Alphabets R or L are used to identify the ostial origin of the vessel, roman numerals I, II, or III are used to represent the anatomical distribution of the vessel, and letters A, B, P, S, and C are used to delineate the course of the vessel with respect to the pulmonary artery and the aorta [6].
| Originating from right cusp | Description | Originating from left cusp |
|---|---|---|
| RI | Solitary vessel arising from either the left or right coronary cusp, following the course of either a normal right or left coronary artery | LI |
| RIIA | Divided into 3 types depending on the relationship of the aberrant vessel to the great vessels. Type A courses anterior to the pulmonary trunk. Type B travels between the aorta and pulmonary trunk. Type P travels posterior to the aorta | LIIA |
| RIIIB | LIIB | |
| RIIP | LIIP | |
| RIII | Absent left coronary artery with the left anterior descending and circumflex arteries arising from the common trunk originating from right coronary cusp |
Our patient had SCA arising from right coronary sinus and presented with acute coronary syndrome and was of R III type. He had successful PTCA from radial approach. Very few cases of SCA have been subjected to PTCA from radial approach.
References
- Yamanaka O, Hobbs RE. (1990) Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 21:28-40.
Publisher | Google Scholor - Roberts WC. Major anomalies of coronary arterial origin seen in adulthood. Am Heart J. 111:941-963.
Publisher | Google Scholor - Hyrtl J. Einige in chirurgischer Hinsicht wichtige Gefässvarietäten. Med Jahrb Österr Staats. 33:17-38.
Publisher | Google Scholor - Horan PG, Murtagh G, Mckeown PP. Single coronary artery-a familial clustering. Heart;12: 27.
Publisher | Google Scholor - Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. (1979) Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 130:39-47.
Publisher | Google Scholor - Yamanaka O, Hobbs RE. (1990) Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Catheter Cardiovasc Interv. 21:28-40
Publisher | Google Scholor




















