

Case Report
Ruptured Tubal Stump Ectopic Pregnancy After Previous Ipsilateral Salpingectomy: A Case Report and Literature Review
- Asfaw Kibret 1*
- Ayalew Adisu 2
- Zerfnesh Zekarias 2
- Dagmawit Tesema 3
- Hagos Alemayehu 3
- Abate Alemu 4
1Department of Emergency Surgery, Leku General Hospital, Ethiopia.
2Department of Anesthesia, Leku General Hospital, Ethiopia.
3Department of Midwifery, Leku General Hospital, Ethiopia.
4Department of Emergency Surgery, Wacha Primary Hospital, Ethiopia.
*Corresponding Author: Asfaw Kibret, Department of Emergency Surgery, Leku General Hospital, Ethiopia.
Citation: Kibret A., Adisu A., Zekarias Z., Tesema D., Alemayehu H., et al. (2024). Ruptured Tubal Stump Ectopic Pregnancy After Previous Ipsilateral Salpingectomy: A Case Report and Literature Review, Clinical Case Reports and Studies, BioRes Scientia Publishers. 7(5):1-3. DOI: 10.59657/2837-2565.brs.24.201
Copyright: © 2024 Asfaw Kibret, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 05, 2024 | Accepted: November 19, 2024 | Published: November 29, 2024
Abstract
Ectopic pregnancy is life threatening condition occurring due to the implantation of fertilized ovum outside the uterine endometrial cavity. Its common site is fallopian tube. Stump ectopic pregnancy after previous salpingectomy on ipsilateral tube is the rare occurrence. We present a 26yrs old female patient with tubal stump ectopic pregnancy who was undergone salpingectomy on ipsilateral tube one year back. This is the first report from ethiopia.
Keywords: ectopic pregnancy, stump tubal ectopic, salpingectomy
Introduction
Ectopic pregnancy occurs when a fertilized ovum implants and grows outside the main cavity of the uterus. This mainly occurs in a fallopian tube, which carries eggs from the ovary to the uterus. Beside the tubes sometimes Ectopic pregnancy occurs in other areas of the body, such as ovary, abdominal cavity or cervix [1]. Epidemiologically ectopic pregnancy occurs in around 1-2% of all pregnancies. The incidence of recurrent ectopic pregnancy is approximately 15
Case Presentation
This is 26yrs old para 1 and who had 1 history of ectopic pregnancy 1yr back for which she underwent salpingectomy. Currently she presented with history of sudden lower abdominal pain and 1 episode of vomiting. She was amenorrheic for last 5weeks and she used to see her menses regularly before she missed it lastly. She doesn’t use any contraceptives. Upon presentation to the emergency room, she was in shock with initial vital signs of BP=70/50mmhg, PR=120bpm, RR=22br/min, Pso2=96%. She was in pain, she has generalized lower abdominal tenderness, there was also cervical motion tenderness and cervix closed. Catching up this she was kept at emergency room with concomitant resuscitation and started to be investigated. Urine HCG comes with positive result, hgb=9.7gm/dl, PLT=153,000, WBC=15000 (Figure 1A). Bedside ultrasound imaging done and revealed empty uterus with free fluid massively in the culde sac and Morison’s pouch and there is extra ovarian hyperechoic collection adjacent to the uterine cornea (Figure 2A). After initial emergency resuscitation she is prepared for exploratory laparotomy for impression of ruptured ectopic pregnancy. Then patient taken to operation room. Intraoperatively there was massive clot and 1200ml hemoperitoneum which is sucked out. There was rt side contained tissues of abortus from the previously salpingectomies stump and the infero-posteriorly the stump was oozing blood trickling to culde-sac. The contra lateral side tube and ovary were quite healthy looking. The uterus was also intact and healthy looking (Figure 2B). The salpingectomy done on the stump and suture ligated. Post operatively she took one unit of cross-matched blood and her hemoglobin was 8.7g/dl with HCT of 22.7% (Figure 1B). Her postoperative condition was smooth and discharged to home after 72hrs of hospital admission.
Figure 1(A, B): Preoperative and post operative CBC results.
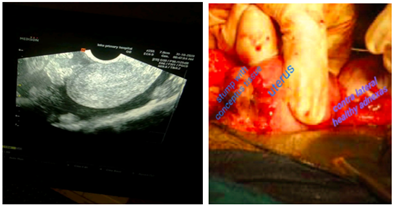
Figure 2: A: Ultrasound image of ruptured ectopic with culde-sac collection and contained clot near the rt side of uterine edge, the uterus clearly seen empty. B: Intra-operative image of the tubal stump ectopic pregnancy rupture.
Discussion
The worldwide incidence of ectopic pregnancy is around 1-2%. In developing nations, it raises with increased prevalence of pelvic inflammatory diseases but in developed nations where assisted reproductive technique is growing technology, ectopic pregnancy incidence may increase over natural conception. In our country Ethiopia systemic review and meta-analysis ectopic pregnancy pooled prevalence was reported as 3.61% [1,2]. More than 90
Conclusion
Stump ectopic is a rare form of ectopic pregnancy and is potentially more dangerous than ampullary tubal ectopic pregnancy. The length of the remnant how much should be left and its association with recurrence needs further case studies.
Declarations
Author’s Contributions: AK is the operating surgeon and compile, organize and write the case report, All the others involved by reading and editing the drafts.
Conflict of Interest: No conflict of interest
Funding: No financial fund taken for this case report
Ethical Approval: The patient information is not revealed and written informed consent is taken from the patient.
Consent: A written consent form was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Data availability-available at reasonable request from corresponding author
References
- Panelli DM, Phillips CH, Brady PC. (2015). Incidence, Diagnosis and Management of Tubal and Non-Tubal Ectopic Pregnancies: A Review. Fertil Res Pract. 1:15.
Publisher | Google Scholor - Ayenew A. (2022). Prevalence and Determinants of Ectopic Pregnancy in Ethiopia: Systematic Review and Meta-Analysis. Journal of Endometriosis and Pelvic Pain Disorders. 14(1):25-42.
Publisher | Google Scholor - Takeda A, Manabe S, Mitsui T, Nakamura H. (2006). Spontaneous Ectopic Pregnancy Occurring in The Isthmic Portion of The Remnant Tube After Ipsilateral Adnexectomy: Report of Two Cases. J Obstetr Gynaecol Res. 32(2):190-194.
Publisher | Google Scholor - Mathew M, Kumari R, Gowri V. (2002). Three Consecutive Ipsilateral Tubal Pregnancies. International Journal of Gynaecology and Obstetrics. 78:163-164.
Publisher | Google Scholor - Boykin T. (2017). Ipsilateral Recurrent Tubal Ectopic Pregnancy Following a Salpingectomy. J Diagn Clin Imaging. 33:114-119.
Publisher | Google Scholor - Samiei‑Sarir B, Diehm C. (2013). Recurrent Ectopic Pregnancy in The Tubal Remnant After Salpingectomy. Case Rep Obstet Gynecol. 753269.
Publisher | Google Scholor - Zuzarte R, Khong CC. (2005). Recurrent Ectopic Pregnancy Following Ipsilateral Partial Salpingectomy. Singapore Med J. 46(9):476.
Publisher | Google Scholor - Mukherjee S, Maheshwari C. (2022). Ruptured Tubal Stump Pregnancy: A Rare Case Report. Int J Repro Contracept Obstet Gynecol. 11:3206-3208.
Publisher | Google Scholor - Gaughran J, Mitchell S, Holland T. (2021). Salpingectomy For Ectopic Pregnancy: Does Length Really Matter? Int J Repro Contracept Obstet Gynecol. 10:333-335.
Publisher | Google Scholor










