

Case Report
Rare Case of Atypical, Unilateral Methotrexate-induced PRES mimicking Stroke Symptoms: Case Report
Department of Radiology and Neurology, Nanavati Max Superspecialty Hospital, India.
*Corresponding Author: Sanzgiri, Sanjana, A/12, Udyan Prabha, Tejpal Scheme Road No. 3, Vile Parle East, Mumbai, Maharashtra – 400057.
Citation: Sanzgiri, Sanjana U, Thakrar, Oak, Dr. Pradyumna J, Salunkhe, Dr. Manish,Patkar, Dr. Deepak P. et al. (2024). Rare Case of Atypical, Unilateral Methotrexate-induced PRES Mimicking Stroke Symptoms: Case Report. International Clinical and Medical Case Reports, BioRes Scientia Publishers 3(3); DOI: 10.59657/2837-5998.brs.24.045
Copyright: © 2024 Sanzgiri, Sanjana U, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 23, 2024 | Accepted: August 31, 2024 | Published: November 09, 2024
Abstract
Posterior reversible encephalopathy syndrome (PRES) is a reversible neurotoxic state which illustrates typical symmetric features on brain MRI scans. However, the uncommon atypical radiological presentations of PRES may lead to misdiagnosis as the clinical and radiological findings are similar to other neurological conditions. Although the pathophysiology of this syndrome is not fully understood, PRES represents a radiographic feature of vasogenic edema in areas of the brain supplied by the posterior circulation. Methotrexate-induced neurotoxicity is a common therapeutic complication in the pediatric population but has been uncommon in adults. A 76-year-old female presented with symptoms similar to stroke, but on further investigation was diagnosed with atypical, unilateral methotrexate-induced PRES. Both clinical condition and radiological abnormalities were resolved after cessation of methotrexate. This case report demonstrates an atypical presentation of unilateral vasogenic edema from an underlying cause of methotrexate which suggests clinicians to consider the prognosis of PRES.
Keywords: posterior reversible encephalopathy syndrome, pres, atypical, unilateral vasogenic edema, methotrexate-induced
Introduction
Posterior reversible encephalopathy syndrome (PRES) is an acute neurological disorder primarily represented with vasogenic edema affecting the parieto-occipital regions [1]. The incidence rate of unilateral involvement in PRES cases is 2.6% [2]. The T2-weighted and fluid attenuated inversion recovery (FLAIR) sequences of magnetic resonance imaging (MRI) aid in visualizing the vasogenic edema to confirm the diagnosis of PRES. Arterial spin labelling (ASL) allows in differential diagnosis of PRES from ischemic stroke. ASL assesses the perfusion by visualizing the cerebral blood flow to detect PRES. MRI diffusion-weighted imaging (DWI) confirms vasogenic edema and at times shows restriction in certain cases [3].
Case Report
History of Presentation
A 76-year-old woman presented in the emergency department with chief complaints of right-sided weakness and slurring of speech, along with staring gaze to the right which was followed by disorientation. She was vitally stable, with her blood pressure measuring 130/70 mmHg, SpO2 98% on room air and pulse rate of 90/min. On CNS examination, GCS score was 13/15, E4V3M6, power in right upper and lower limb was 2/5, plantars bilateral withdrawal and disorientation. No other abnormality was detected in the systemic examination. Upon her examination, code white was activated, and an MRI examination of the brain was performed; findings of which are explained in detail further.
Footnote
CNS: Central Nervous System; GCS: Glasgow Coma Scale; E: Eye opening; V: Verbal response; M: Motor response.
Past Medical History
The patient has a medical history of rheumatoid arthritis for which she received treatment, chronic venous insufficiency of both lower limbs and hypothyroidism.
Investigations
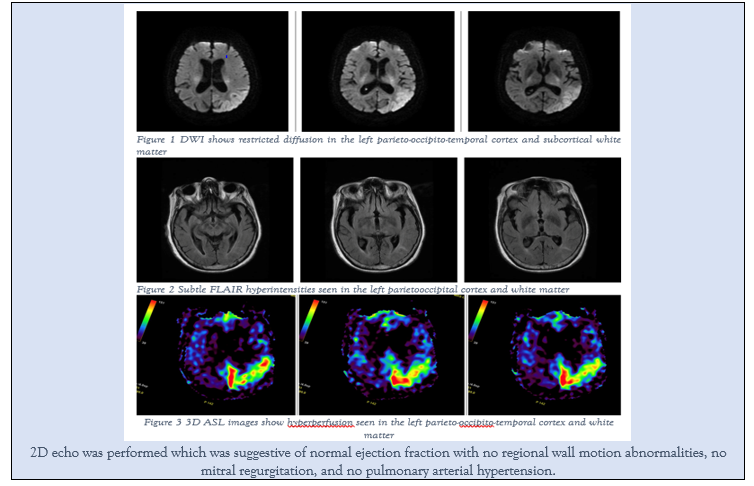
An MRI (3 Tesla) scan of the brain was performed using T1 and T2-weighted sequences in multiple planes, using a multiple array head coil. The scan revealed large area of mild diffusion restriction involving the left parieto-occipitotemporal cortex and subcortical white matter (Figure 1), with subtle FLAIR hyperintensity (Figure 2). On 3D ASL, there is relative hyper perfusion in the same region (Figure 3).
Medical Management
The methotrexate medication was discontinued, and the patient was conservatively managed. Anti-epileptic medicines were administered.
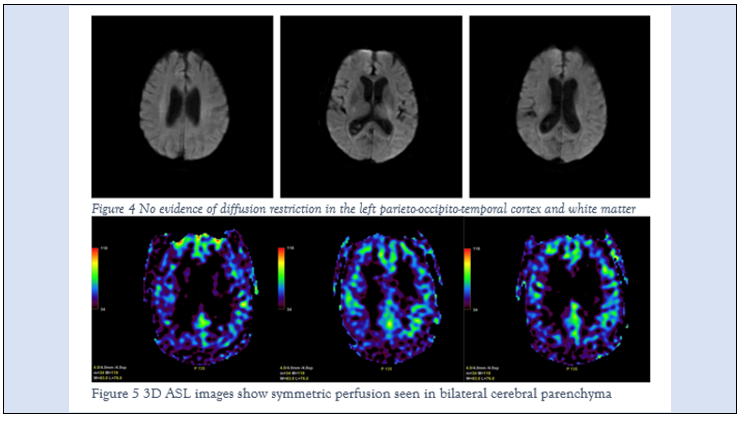
To evaluate the treatment response and clinical changes in the brain, another MRI scan was performed before discharge. The DWI scan (Figure 4) showed resolution of diffusion restriction in the left parieto-occipito-temporal cortex and subcortical white matter. On 3D ASL images, there was symmetrical perfusion seen in bilateral cerebral parenchyma (Figure 5) which confirmed improvement in patient’s condition.
Follow-Up
At discharge, the patient was hemodynamically and vitally stable.
Differential Diagnosis
PRES may be misdiagnosed for progressive multifocal leukoencephalopathy (PML), posterior circulation infarct, inflammatory cerebral amyloid angiopathy or reversible cerebral vasoconstriction syndrome (RCVS) since they illustrate resemblance in radiological findings coupled with similar clinical representation. [4] PML is a viral disease affecting the brain’s white matter characterized by destruction of myelin. [5] Posterior circulation infarct is a neurological deficit caused by infarction within the vertebrobasilar arterial system affecting the posterior circulation of the brain. [6] Cerebral amyloid angiopathy is a rare encephalopathy characterized by inflammatory response from amyloid-b deposition in the small and medium-sized arteries of the leptomeninges and cerebral cortex. [7] RCVS is a group of disorders characterized by vasogenic edema, watershed infarcts and reversible vasoconstriction of the cerebral arteries. [8] Table 1 represents the clinical representations and MRI findings of PRES and its differentials.
Table 1: Clinical profile and MRI findings of PRES and its differentials
| Conditions | PRES | Progressive Multifocal Leukoencephalopathy (PML) | Posterior Circulation Infarct | Inflammatory Cerebral Amyloid Angiopathy | Reversible Cerebral Vasoconstriction Syndrome |
| Clinical Profile | Headache; Seizures; Altered; consciousness; Visualdisturbance; Focalneurological; deficits | Loss of coordination; Difficulty in walking; Facial drooping; Memory loss; Loss of vision | Gait ataxia; Vertigo Nausea; Vomiting Slurred speech; Dysarthria; Diplopia | Headache; Seizures Decrease in consciousness; Cognitive changes; Focal neurological deficits | Sudden and severe thunderclap headaches Seizure; Changes in vision |
| MRI findings | Bilateral vasogenic edema with in occipital and parietal regions Affected areas illustrate vasogenic edema; T2-hyperintense Increased diffusion on ADC images; Both cortical and subcortical areas are affected | DWI– diffusion restriction involving bilateral but asymmetrical supratentorial white matter and thalamic involvement T2- hyperintense | DWI restriction more pronounced than T2/FLAIR hyperintensity T1-weighted images show high signal changes in globus pallidus | White matter hyperintensity represents vasogenic edema T2-FLAIR –white matter hyperintensity that are asymmetric and extend to the subcortical white matter | Cortical edema and/or vascular FLAIR hyperintensities may precede vasoconstriction; PRES-like reversible cerebral edema seen on FLAIR sequence |
Discussion and Conclusions
There are many underlying causes, medical treatments or medical conditions that may result in PRES. The pathophysiological mechanism underlying the development of PRES is not well understood. PRES is a neurological entity characterized by reversible vasogenic edema affecting the occipital and parietal lobes.[3] The typical MRI findings of PRES show symmetric hyperintensity with bilateral vasogenic edema in parieto-occipital cortical and subcortical locations in the white matter on FLAIR images whereas <5>Table 2 represents the conditions associated with the development of PRES [3].
Table 2: Conditions associated with the development of PRES
| Common General Conditions | Common Autoimmune Disorders | Toxins | Common Immunosuppressive medications | Other medications |
| Hypertension Renal Failure Eclampsia and pre-eclampsia Sepsis Solid Organ Transplantation | Rheumatoid arthritis Vasculitis Crohn’s disease | Cocaine Alcohol intoxication | Methotrexate Corticosteroids | Intravenous contrast Lithium |
MRI is the gold standard for diagnosing PRES as it assists with confirming the syndrome and shows its extent. The symmetric vasogenic edema affecting the subcortical and cortical location is best seen on MRI with FLAIR sequence while DWI allows in confirming vasogenic edema with absence of restricted diffusion. [3] ASL, a non-contrast, noninvasive MR perfusion technique is commonly used to accurately detect stroke mimics like PRES. Often, there is symmetric regional hyper perfusion in the bilateral occipital lobes seen on the ASL for the PRES condition, which is the result from breakdown of cerebral autoregulation, caused due to severe hypertension resulting in excessive blood flow, increased capillary pressure and subsequent vasogenic edema. But in this case, there was relative hyper perfusion on the left parieto-occipitotemporal cortex and subcortical white matter which seemed atypical. [10]
Etiological findings revealed methotrexate (as the cause). After discontinuing medication, the patient’s clinical condition significantly improved. This along with the findings of MRI solidified the diagnosis of methotrexate-induced unilateral PRES. This case report suggests that clinicians should consider prognosis of PRES in radiological representation of unilateral vasogenic edema.
References
- Bartynski WS. (2008). Posterior Reversible Encephalopathy Syndrome, Part 1: Fundamental Imaging and Clinical Features. American Journal of Neuroradiology., 29:1036–1042.
Publisher | Google Scholor - Willard N, Honce JM, Kleinschmidt-DeMasters BK. (2018). PRES: Review of Histological Features. J Neuropathol Exp Neurol., 77:100–118.
Publisher | Google Scholor - Triplett JD, Kutlubaev MA, Kermode AG, Hardy T. (2022). Posterior reversible encephalopathy syndrome (PRES): diagnosis and management. Pract Neurol., 22:183–189.
Publisher | Google Scholor - Smith D, Gaillard F. (2008). Posterior reversible encephalopathy syndrome. RadiopaediaOrg.
Publisher | Google Scholor - (2023). Progressive multifocal leukoencephalopathy Information | Mount Sinai - New York n.d.
Publisher | Google Scholor - Hoyer C, Szabo K. (2021). Pitfalls in the Diagnosis of Posterior Circulation Stroke in the Emergency Setting. Front Neurol., 12: 682827.
Publisher | Google Scholor - Moussaddy A, Levy A, Strbian D, Sundararajan S, Berthelet F, Lanthier S. (2015). Inflammatory Cerebral Amyloid Angiopathy, Amyloid-β-Related Angiitis, and Primary Angiitis of the Central Nervous System: Similarities and Differences. Stroke; 46: e210–213.
Publisher | Google Scholor - Kim D, Gaillard F. (2008). Reversible cerebral vasoconstriction syndrome. RadiopaediaOrg.
Publisher | Google Scholor - Çamlıdağ İ, Cho YJ, Park M, Lee SK. (2015). Atypical Unilateral Posterior Reversible Encephalopathy Syndrome Mimicking a Middle Cerebral Artery Infarction. Korean J Radiol., 16:1104.
Publisher | Google Scholor - Weinstein JD, Hamam O, Urrutia VC, Lu H, Luna LP, Tekes-Brady A, et al. (2022). Added Value of Arterial Spin Labeling in Detecting Posterior Reversible Encephalopathy Syndrome as a Stroke Mimic on Baseline Neuroimaging: A Single Center Experience. Front Neurol., 13:831218.
Publisher | Google Scholor














