

Case Report
Preoperatively Manifestations as Univesicular Mass Like Lesion and Postoperatively as Multivesicular Lesion with Multiple Daughter Cyst: Report A Very Rare Case
- Manouchehr Aghajanzadeh 1*
- Ali Alavi Foumani 2
- Azita Tangestaninejad 2
- Seyed Aliaskhar Fakher Mosavi 2
- Omid Mosaffaee Rad 1
- Zahra Sadin 3
- Mohaya Farzin 4
1Department of Thoracic Surgery, Guilan University of Medical Sciences, Rasht, Iran. 2Department of Pulmonology, Guilan University of Medical Sciences, Rasht, Iran. 3Inflammatory Lung Diseases Research Center, Department of Internal Medicine, Razi Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran. 4Department of physiology, Razi Clinical Research Development Center, Guilan University of Medical Sciences, Rasht, Iran.
*Corresponding Author: Manouchehr Aghajanzadeh.1Department of Thoracic Surgery, Guilan University of Medical Sciences, Rasht, Iran.
Citation: Aghajanzadeh M, Ali A. Foumani, Tangestaninejad A, S.A.F. Mosavi, Omid M. Rad, et al. (2024). Preoperatively Manifestations as Univesicular Mass Like Lesion and Postoperatively as Multivesicular Lesion with Multiple Daughter Cyst: Report A Very Rare Case. International Clinical and Medical Case Reports, BioRes Scientia Publishers 3(2):1-6. DOI: 10.59657/2837-5998.brs.24.047
Copyright: © 2024 Manouchehr Aghajanzadeh, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 30, 2024 | Accepted: October 10, 2024 | Published: October 30, 2024
Abstract
Pulmonary univesicular hydatid cyst and uncomplicated cysts with Echinococcosis granulose and daughter cysts are very rare. A 58-year-old man presented to our center with cough, hemoptysis and right-side chest wall pain. Chest x-ray and computerized tomography scan revealed a cystic like appearance mass in the hill of right lung. FOB and BAL was normal. With right side PL- thoracotomy cystic mass of lung was removed. Hundreds of 1to3 cm size daughter cysts and laminated membrane was discovered after opened the cystic mass. Pathologic examinations revealed the hydatid cysts with daughter cysts on the lung cystic mass. To best of our knowledge probably this is rare presentation of lung hydatid cyst as mass like and univesiculr cyst which full of daughter cyst.
Keywords: daughter cyst; lungs; univesicular hydatid cyst; cystic mass
Introduction
Hydatid disease is caused by an infection with the cestode Echinococcus granulosus. Cystic echinococcosis is seen in some countries in words and is public health problems in endemic areas, such as South and Central America, the Middle East, Africa, Russia, China, Australia and New Zealand. and is endemic in Iran [1-3]. Adult worms mature in the intestine of dog (definitive host) and the eggs are released in the stool [4-6]. Adult worms mature in the intestine of dog (definitive host) and the eggs are released in the stool [3-5]. Animals like sheep get this disease by via ingestion of contaminated vegetables. Humans are accidental host, oncospheres hatch in the duodenum, penetrate the intestines and are carried via the bloodstream to various organs [3-5].it most often affects the liver and the lungs tissue [1,34,5]. Hydatid disease mostly affects the liver (75%) and the lungs tissue (15%), and occurs only 10% in others organ [2-8]. Pulmonary hydatid disease may be accompanied by complications including cyst rupture into the pleural space, lung mass, hemoptysis, suppuration [9-13]. Patients may develop sudden onset of chest pain, cough, fever, and hemoptysis after a cyst ruptures, urticaria wheezing and anaphylaxis secondary bacterial infection. Infection resulting in difficulty in differentiation disease [2-4,7-9,13].
Hydatid disease should be in the differential diagnosis when a cystic lesion detected in an endemic area as bronchogenic cyst, lung carcinoma, sarcoma of the lung, metastasis, hematoma, mesothelioma, granulomatouse lesions andpulmonary abscess [2-4,7-9,13-15]. Daughter cysts and calcifications are rarely seen in pulmonary hydatid cysts. [14,15]. Chest imaging is the principal investigational modality for pulmonary hydatid cyst. computed tomography (CT), and magnetic resonance imaging (MRI) of the lungs are the various useful modalities in the diagnosis of thoracic hydatid cyst [7-13]. The treatment is surgery [1,6,10,12,13]. The goal of surgical intervention includes removal of the entire cyst while preserving the lung parenchyma as much as possible and without allowing intra operative spillage [1,9-12]. The aim of this case report is for three interested causes, first is the unusual presentation as univesicular cyst in imaging preoperative and with multiple daughter cysts postoperative, second is the location of cyst which in the hill of lung and third is present as cystic mass lesion.
Case Report
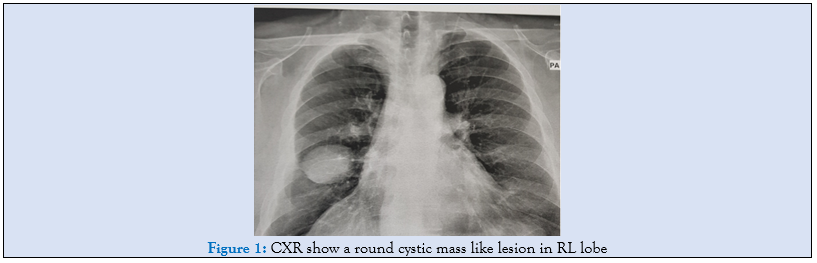
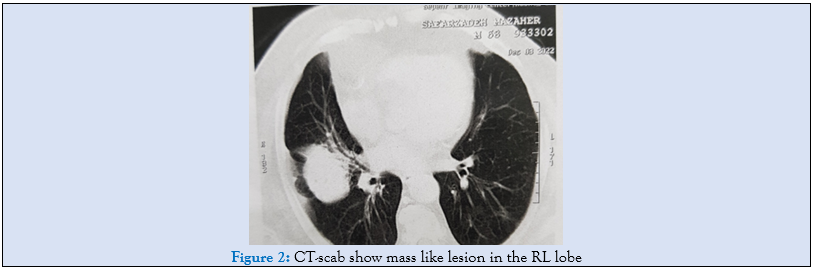
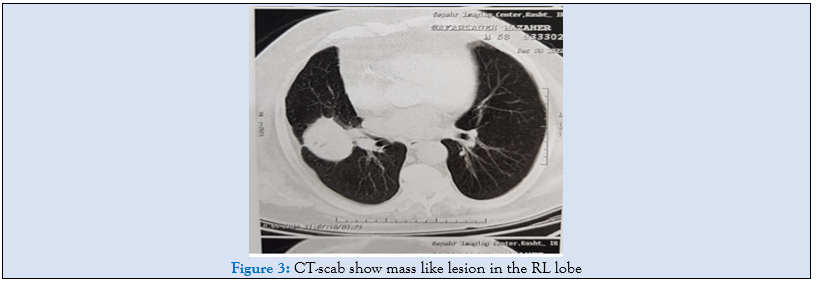
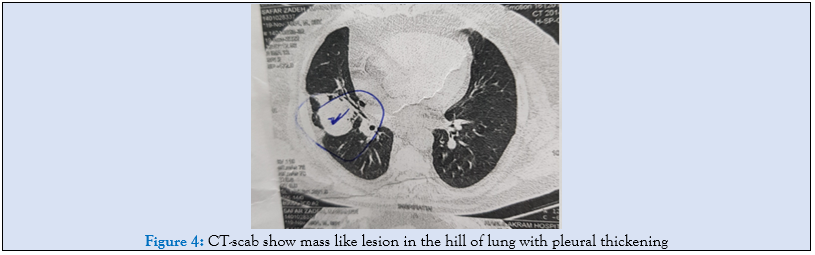
A 58-year-old man was admitted to our referral hospital in pulmonology department with complaint of dry cough, milled hemoptysis, right side chest pain, night sweeting and Lowe grade fever for three months. The symptoms in recent two weeks were sudden expectoration mild sputum with mixed with blood. In examination the respiratory sounds were normal but crackles were present in right hemi thoraces. Chest roentgenogram and computed tomography (CT scan) demonstrated cystic mass like lesion in the right hill of lung (14 × 12 × 11 cm), (Fif 1,2,3,4).
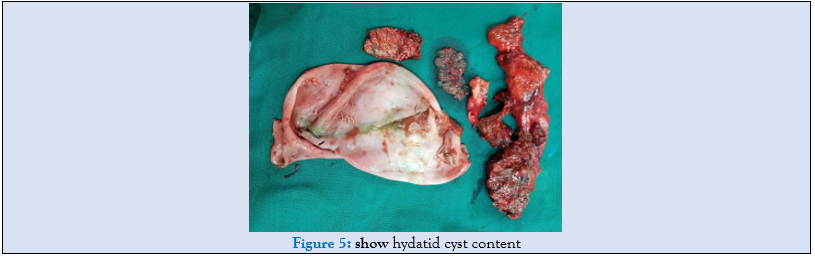
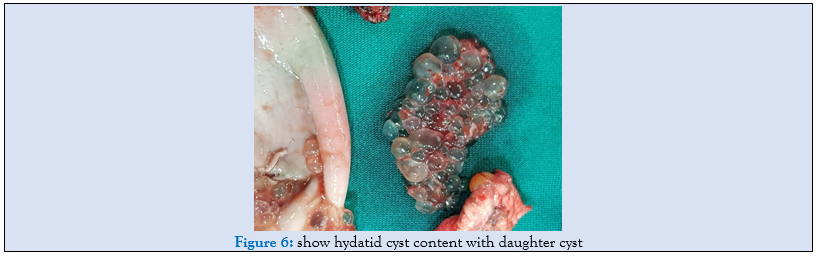
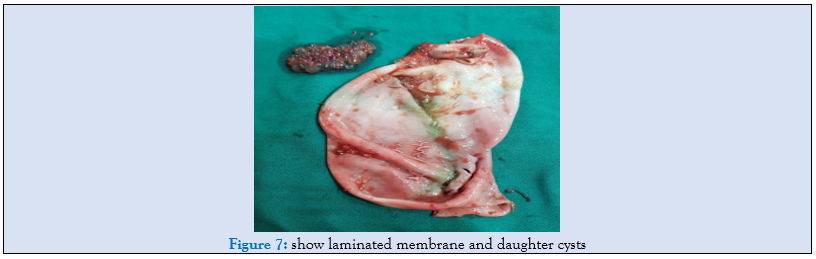
FOB performed show small compression on the right upper lobe, others were normal. BAL was normal in pathology evaluation. Patient refereed to thoracic surgery ward for excision of that lesion. After general anesthesia with one lung ventilation, five intercostal space was opened in right up position with muscle saving procedure. After pneumolysis the cystic mass in the hill of lung was walling of with wet sponge in normal saline for prevention of spillage cyst content of cystic mass when rupture occurs, because in endemic area as Iran all cystic masses should be in diffrencited from hydatid disease. The cystic mass was resected with safe margin as wedge resection. After chest -tube insertion and closed of chest wall the cystic mass was operated. After opened the mass there was ruptured laminated membrane with more than hundreds of 1 to3cm daughter cysts in cavity (Fig 5,6,7).
Ultrasonography of abdomen was normal for cystic or mass lesions. Albendazole 800 mg prescribe for three cores of 28 days with 14-day interwall. The patient discharged on the fifth day postoperatively without any complications. As a result, the pathologic examinations of ruptured laminated membranes and daughter cysts confirmed a hydatid cyst. On 6 and 12 month follow up, patient condition is well.
Discussion
Hydatid cysts disease is still a significant health problem in certain countries such as South and Central America, the Middle East, Africa, Russia, China, Australia and New Zealand. and Central Europe occur in immigrants from endemic areas and in this area’s hydatid cysts are endemic [1-3,4,5,9]. In Iran hydatid cysts are endemic [1,14,15].
Hydatid disease mostly affects the liver (75%) and the lungs tissue (15%), and occurs only 10% in others organ [2,4,5-8]. Pulmonary hydatid cysts are usually asymptomatic while symptoms may appear with increasing size over a period of time or in cases that cysts are in the central portion of lung or other complications [3,9-12]. .as our case. Hydatid disease is caused by an infection with the Echinococcus granulosus in endemic area such as Iran [1,3,7,11,12]. The hydatid cysts may remain asymptomatic for a long time. As they enlarge, the cysts may rupture and patients complain of cough, expectoration of membranes, hemoptysis, and thoracic pain in cases of pulmonary cysts [3,7,11,12]. Adult worms mature in the intestine of definitive host as dog and the eggs are defecated with stool [3,4-6]. Animals like sheep get this disease by via ingestion of contaminated vegetables and water. Humans are accidentally infected. Oncospheres hatch in the duodenum mucosa of sheeps and penetrate the intestines and are carried via the bloodstream to various organs as liver, lung and all organs [3-7]. Daughter cysts can also sporadically or very rarely be seen in pulmonary hydatid cysts [3,4,7,9,11,12]. The germinative layer secretes hydatid fluid and generates brood capsule, If the inner layer and the brood capsules spitted up, daughter cysts can be produced. [13]. Due to early presentation of symptoms and treatment, in PHC there in enough time for forming the daughter cystshence the occurrences of daughter cysts in the pulmonary hydatid cysts are uncommon [14]. We present one case with a cystic mass lesion and univesicular on CT-scan in the hill of right lung before surgery with hundreds of daughter cysts with laminated membrane postoperative, like such case rarely reported in the literature [14].
Univesicular cysts may contain no daughter cysts, [14,15] and are called unilocular and cyst with daughter cysts are called multivesicular. in the literature [15] Chest X-ray and CY-scan can show cyst mas lesion as a round opacity in a hemi thorax [14,15]. CT scan can detect pulmonary hydatosis with or without daughter cysts [14,15] but CT-scan cannot show small sizes of daughter cysts as our case before surgery. Repeated mechanical trauma such as heart beats and respiratory motions and separation of some parts of laminated membrane from of pericyst layer into the cyst cavity and formation of daughter cysts, Daughter cysts may develop directly from the end cyst, resulting in multisystem or multivesicular pulmonary hydatid cysts, [13-15,18].In this our case, daughter cysts were present in the mass like cystic lesion . Daughter cysts rarely can be seen in pulmonary hydatid cysts. The hydatid fluid and brood capsule secrete by germinative layer. Daughter cysts can be produced by spitted up germinative and brood capsules [21]. Because of early presentation of symptoms and early treatment of pulmonary hydatid cyst there are no enough time for forming the daughter cysts., hence the occurrences of daughter cysts in the pulmonary hydatid cysts are very uncommon [21]. We present one case of intact lung hydatid cysts of lung in CT-scan without any daughter cysts but postoperative there was more than hundred daughter cysts rarely reported in the literature. cysts without daughter cysts are called univesicular and those with daughter cysts are called multivesicular. CT scan can show pulmonary hydatid cysts with or without daughter cysts [21] but in majority of cysts due to very small sizes of daughter cysts CT -scan not detected before surgery [21] as our case. There are two theories for formation of daughter cysts [21]. Repeated mechanical trauma such of pulsation of heart beats and respiratory motions and opening of bronchioles into the cyst cavity [21]. In our case, daughter cysts were not present in the hydatid cyst but it presents in the mass cystic lesion postoperative with cut the mass.
It is required to Differential diagnosis from lung masses which most commonly present with malaise, weight loss, cough especially in endemic area as Iran [14].
hydatid cysts of lung should be always kept in the differential diagnosis when a cystic lesion is detected in a patient who has come from an endemic area. Differential diagnosis for pulmonary HCs can be listed as bronchogenic cyst, lung carcinoma, sarcoma of the lung, metastasis (when cysts are multiple), hematoma, mesothelioma, granuloma, and lung abscess [16,17]. CT-scan and MRI can help cysts from masses in some patient but not definitive diagnosis not possible [4,5,7,14]. Transthoracic needle biopsy is dangerous or contraindicated in endemic area in such as our case, because can ruptured cyst and produce anaphylaxis and dissemination of cysts content [3,4,7.11].
Surgical treatment. For patients who are cardiovascular stable and able to undergo major operation, Surgery is the treatment of choice because parasite can be excised completely and the patient will be cured [1-3,10,11,14]. Our surgical options for lung cysts include wedge resection, evacuation, bronchial opening closure with precystectomy, rarely lobectomy, and capitonnage for obliteration of remnant cavity [1,3,7,11,12]. During surgery it is important to prevent spillage of cyst contents intraoperative for dissemination, allergic reactions and recurrence [1,3,7,11,12,14]. In our patient we don’t use any sporicidal agents in pulmonary hydatid cysts. Medical therapy with Albendazole is Used in patients which cannot tolerated undergrowing surgery or in disseminated disease and when there is intraoperative spillage of hydatid fluid [17-20], After surgery we priscibe Albendasol 800 mg in three cores of 28 days with 14 days’ interval.
Conclusion
In Conclusion, in endemic area all cystic mass lesion of lung should be differenced from hydatid cysts. MRI and CT -scan help for diagnosis but FOB can help for diagnosis of lung mass or some time ca see the priciest. The only way for definitive diagnosis is surgery as VATS or thoracotomy.
Acknowledgments
The authors would like to thank the Razi Clinical Research Development Unit.
Disclosure of conflict of interest
No conflict of interest to be disclosed.
Statement of ethical approval
This study was approved by ethic comity of arya hospital and Inflammatory Lung Diseases Research Center of Razi hospital, Guilan University of Medical Sciences, Rasht, Iran.
Statement of informed consent
Informed consent was obtained from all individual participants included in the study.
References
- Aghajanzadeh M, Safarpoor F, Amani H, Alavi A. (2008). One-stage procedure for lung and liver hydatid cysts. Asian CardiovascThorac Ann., 16:392-395.
Publisher | Google Scholor - Sarkar M, Pathania R, Jhobta A, Thakur BR, Chopra R. (2016). Cystic pulmonary hydatidosis, Lung India., 33:179-191.
Publisher | Google Scholor - Ehsan Hajipour Jafroudi, Manouchehr Aghajanzadeh, Ali Alavi Foumani, Azita Tangestaninejad, Yousha Pourahmadi, (2022). Mahsa Mousazadeh, Pulmonary hydatid cyst mimicking pneumonia, lung mass, pneumothorax, pleural effusion, pulmonary abscess, and pyopneumothorax International Journal of Life Sciences., 10(4):12-31
Publisher | Google Scholor - Havlucu Y, Ozdemir L, Sahin E. (2010). Multiple cystic echinococcosis mimicking metastatic malignancy. Respiratory Med., 3:132-134.
Publisher | Google Scholor - Kuzucu A, Ulutas H, RehaCelik M, Yekeler E. (2014). Hydatid cysts of the lung: Lesion size in relation to clinical presentation and therapeutic approach. Surg Today., 44:131-136.
Publisher | Google Scholor - Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. (2003). Hydatid disease from head to toe. Radiographics., 23: 475-494.
Publisher | Google Scholor - Asgary MR, Aghajanzadeh M, Hemmati H, Safarpoor F, Alavi A, Amani H. (2016). The clinical finding, diagnosis and outcome of patients with complicated lung hydatid cysts. Int J Med Res Health Sci., 5: 293- 297.
Publisher | Google Scholor - Hasdıraz L, Onal O, Oguzkaya F. (2013). Bilateral staged thoracotomy for multiple lung hydatidosis J Cardiothoracic Surg., 8: 121.
Publisher | Google Scholor - Trilok C, Avdhesh B, Aanchal T. (2016). Hydatid lung disease presented with multiple pulmonary nodules. J Health Res., 3: 137-140.
Publisher | Google Scholor - Saviz Pejhan, Mohammad Reza Lashakri Zadeh, Mojtaba Javaherzadeh, Mohammad Behgam, Shadmehr, Mehrdad Arab, et al. (2007). Treatment of Complicated Pulmonary Hydatid Cyst, Tanaffos., 6(1):19-22
Publisher | Google Scholor - Mohammad Reza Asgary, Manouchehr Aghajanzadeh, Hosein Hemmati1,F.Safarpoor1, Ali Alaviand Hosein Amani, (2016). The clinical finding, diagnosis and outcome of patients with complicated lung hydatid cysts, Int J Med Res Health Sci., 5(8):293-297
Publisher | Google Scholor - Manouchehr Aghajanzadeh1, Ali Alavi, Alirza Jafarnegad, Azita Tangestaninejad, PedramTalebi, Rasool Hassanzadeh, and Mahdi Pursafar, (2022). Multiple and Bilaterally Pulmonary Hydatid Cystic Mimicking Metastatic Lesions, International Journal of Life Sciences., 10(4).
Publisher | Google Scholor - Bonfrate L, Giuliante F, Palasciano G, Lamont JT, Portincasa P. (2013). Unexpected discovery of massive liver echinococcosis.A clinical, morphological, and functional diagnosis. Ann Hepatol. 12:634–641.
Publisher | Google Scholor - Mohsen Sokouti, Babak Sokouti, Behrooz Shokouhi, and Mohammad Hossein Rahimi-Rad Multi- vesicular pulmonary hydatid cyst, (2015). the potent underestimated factor in the formation of daughter cysts of pulmonary hydatid disease. Lung India. 32(4): 375–377.
Publisher | Google Scholor - Saidi F. 1st ed. (1976). Philadelphia: WB Saunders;. Surgery of Hydatid Disease., 156–281.
Publisher | Google Scholor - Pedrosa I, Saiz A, Arrazola J, Ferreiros J, Pedrosa CS, (2000). Hydatid disease: radiologic and pathologic features and complications. Radiographics., 20:795–817
Publisher | Google Scholor - Morar R, Feldman C, (2003). Pulmonary echinococcosis. Eur Respir J., 21:1069–1077
Publisher | Google Scholor - Kilani T, El Hammami S. (2002). Pulmonary hydatid and other lung parasitic infections. Curr Opin Pulm Med., 8: 218–223.
Publisher | Google Scholor - Filice C, Brunetti E. (1997). Use of PAIR in human cystic echinococcosis. Acta Trop., 64: 95–107.
Publisher | Google Scholor - Akhan O, Ozmen MN, Dincer A, Gocmen A, Kalyoncu F. (1994). Percutaneous treatment of pulmonary hydatid cysts. Cardiovasc Intervent Radiol., 17: 271–275.
Publisher | Google Scholor - Mohsen Sokouti, Babak Sokouti,1 Behrooz Shokouhi,2 and Mohammad Hossein Rahimi-Rad3 Multi- vesicular pulmonary hydatid cyst, (2015). the potent underestimated factor in the formation of daughter cysts of pulmonary hydatid disease Lung India., 32(4): 375–377
Publisher | Google Scholor











