

Review Article
Physical Exercise, Psychological and Neurological Health: Reviewing the Anxiety and Depression Variables
- Jonatas Deivyson Reis da Silva Duarte *
Federal University of Mato Grosso and Power Fit Gym, Mato Grosso, Brazil.
*Corresponding Author: Jonatas Deivyson Reis da Silva Duarte, Federal University of Mato Grosso and Power Fit Gym, Mato Grosso, Brazil.
Citation: : Jonatas D R Duarte (2023). Physical exercise, psychological and neurological health: reviewing the anxiety and depression variables. Journal of Clinical Psychology and Mental Health, BRS Publishers. 2(1); DOI: https://www.doi.org/brs/2023/jcpmh/0004
Copyright: © 2023 Jonatas Deivyson Reis da Silva Duarte, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 06, 2023 | Accepted: March 14, 2023 | Published: March 24, 2023
Abstract
Anxiety and depression are the most commonly affected psychopathologies in the world, and it is estimated that the diagnosis and the sale of medication will increase more and more. They can affect children and elderly people of both sexes (but more prevalent in women) and from all social classes. From a physiological point of view, it is the dysregulation in the production, transference, and uptake of monoaminergic neurotransmitters (dopamine, norepinephrine, and serotonin). Antidepressant drugs act mainly on the production and non-degradation of these neurotransmitters. Studies show that exercise has the effect of producing these neurotransmitters mainly after sessions, and also improves neural health. In this review article these aspects will be discussed.
Keywords: sport psychology; neurophysiology; psychiatry; mental health; physical education
Introduction
Psychopathological illnesses such as anxiety and depression have been increasing over the years. They are more prevalent than other psychopathological illnesses such as schizophrenia, panic syndrome, phobias, post-traumatic stress, etc. [1]. As a definition, anxiety is seen as a subjective emotional state of uneasiness or distress, arising from an anticipated situation of real or imagined threat [2]. Depression, on the other hand, is a state of deep sadness [3]. These psychopathologies can affect children, adolescents, college students, adults and the elderly [4–8]. Its prevalence appears to be higher in women [9]. A possible physiological explanation for this phenomenon is the hormonal fluctuations that occur in women, which influence the modulation of various neurotransmitters [10].
The main causes of anxiety can be other health problems, genetics, traumatic events, use of licit and illicit drugs, it is even believed that some medications can cause anxiety [11]. In this context, fear is something normal when faced with some danger, however, when this fear is overwhelming and persistent, being accompanied by worry all the time, feeling tired, being irritable, having difficulty concentrating and sleeping poorly is already considered pathological [11]). Depression can also be due to several factors such as the loss of a loved one, genetics, trauma, social aspects (bullying, abuse or loneliness), molecular and neurochemical factors, among others [12]. It can include negative events in childhood that can be the cause of anxiety and depression in adulthood [4]. However, people react differently to a stressful event, due to the difference in perceived stress [13].
In some cases major depressive disorder can even lead to suicidal behavior, thus becoming a public health concern in several countries [14]. In this sense, for an individual to be considered healthy not only his body has to be free of pathologies [diabetes, obesity, osteoporosis, hypertension, cancer, among others], but also the psychological. The main means of treatment are medication, psychotherapy, and regular exercise [15]. Other non-pharmacological means can also lead to a reduction of anxiety and depression symptoms, such as social and family support, relaxation techniques, spirituality and religiosity [16].
In this context, the main focus of this review is the alternative treatment related to regular physical exercise, specifically in the variables of anxiety and depression, and the neurochemical response associated with these psychopathologies. This may bring relevant information to physicians, physical education professionals, psychologists, and individuals interested in the subject. For this, the keywords "exercise and psychological health", "exercise and serotonin", "exercise and depression", "exercise and anxiety" and "exercise, anxiety and depression", "exercise and BDNF", "exercise and brain" and "exercise and dopanin" were searched in the google scholar, pubmed and scopus indexing bases.
Evidence for physical exercise in improving mental health
There are several studies with different modalities, the main methods being the use of questionnaires. There are specific questionnaires to analyze mood, anxiety, and depression. Most of these studies show a positive association between individuals who practice physical exercises and psychological health. There is evidence that aerobic exercises of 20 to 30 minutes have a calming effect after the session and may last for hours [17]. A review study found that strength training can improve age-related conditions of insomnia, anxiety, depression, and cognitive decline [18]. As well as martial arts also having evidence with jiu-jitsu, kickboxing [19], tai chi [20] and taekwondo [21–23].
Other sports may also be viable options such as cycling [24], swimming [25], o high intensity interval training [26], intense training programs (Crossfit) [27], among others. The aforementioned evidence shows such benefits from children to the elderly.
Additionally, people who would acquire some type of disability [paraplegia, blindness, deafness, etc.] are more likely to acquire psychological problems due to disability and loss of independence [28]. The adapted sports arose so that these people could practice them [29], there are several possibilities depending on the degree and type of the individual's disability, such as sled field hockey, wheelchair basketball, goalball, sitting volleyball, among others [30]. The practice of sports by these people seems to be a good option to improve life satisfaction and quality of life, consequently decreasing the perception of anxiety and depression [31]. Perhaps, competitive participation is a potentiator of these benefits in this population [31].
Furthermore, as regular physical exercise is related to body aesthetics, it can change the person's belief about himself, consequently improving self-esteem and quality of life. Other health benefits can be observed in research such as: prevention and treatment of hypertension [mainly aerobic exercises] [32], sarcopenia [exacerbated decrease in muscle mass, one of the most interesting exercises being strength training] [33], osteoporosis [decreased bone density] [34], Alzheimer's disease and other dementias [35]. In summary, the improvement in physical conditioning resulting from exercise positively impacts health status [36]. Figure 1 shows the various benefits of regular physical exercise.
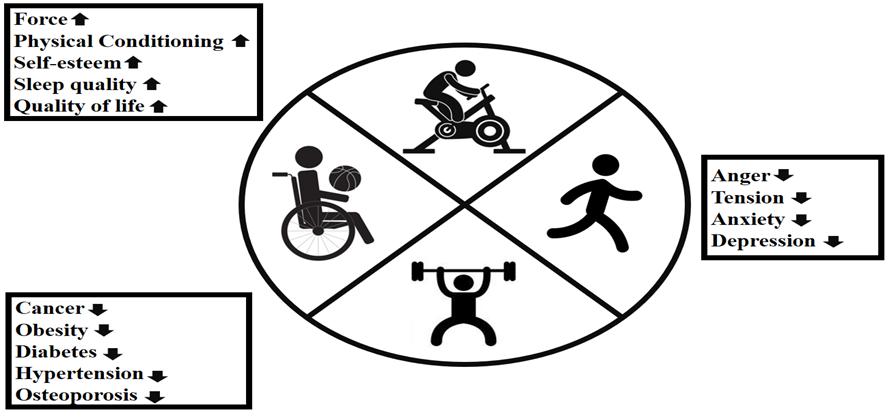
Figure 1: The benefits of regular aerobic and anaerobic exercise.
Regarding exercise recommendations for adults, 150 to 300 minutes of moderate intensity exercise, or 75 to 150 minutes of rigorous intensity exercise or a combination of moderate and vigorous intensity exercise is suggested [37]. The physical education professional who is working with this public should have knowledge of the reasons that motivate them to practice, so that strategies can be made to increase the chance of permanence [38]. Additionally, the motivation of men and women appear to be similar for these practices [39] and in an appropriate and adapted way can be practiced from children to the elderly [40,41].
Neurotransmitters and physical exercise
Neurotransmitters are an important class of messenger molecules that govern chemical communications in the brain [42]. There are several neurotransmitters with different functions such as mood regulation, voluntary and involuntary movements [organ function], and other functions. The neurotransmitters responsible for mood regulation are serotonin, dopamine, and norepinephrine [43]. These neurotransmitters most likely exert an effect on the brain regions responsible for emotions such as: insula lobe, amygdala, cingulate gyrus, prefrontal cortex, and anterior cingulate cortex [44]. Psychopathologies such as anxiety and depression are physiologically associated with disturbances in the synthesis, release, transport and reuptake of these neurotransmitters [43].
The production of these neurotransmitters is done via signaling in which specific genes are responsible for their production [45]. Antidepressant drugs increase the signaling of serotonin, norepinephrine, and dopamine production [46], in addition to inhibiting an enzyme called monoamine oxidase (which degrades these neurotransmitters), thus increasing their availability in neurons [47]. Unfortunately, antidepressant drugs [which are used in the treatment of anxiety and depression] take several weeks to take effect inducing adaptive changes in the brain structures affected by these psychopathologies [48]. There are even people who do not respond well to drug treatment [49]. The commercialization of these neurotropic drugs began in the 1950s [50] and contemporarily many are the factors that can influence the type of drug that will be prescribed such as local practices, knowledge of the literature, clinical guidelines and even pharmaceutical sponsorships [51].
Physical exercise has the non-pharmacological effect on serotonin, norepinephrine and dopamine signaling [52]. Studies in several countries have shown higher production of these neurotransmitters during high intensity interval training [53], aerobic training [54], pilates [55], taekwondo [56] and the combination of strength and aerobic training [57]. Increases in serotonin concentration is related to physical and mental fatigue during exercise [58]. Thus, a possible potentiator of the drug's effect [19].
The amino acid tryptophan is an obligate substrate for the production of serotonin in the brain, intestine, and pineal gland [59]. the physical exercise has the effect of increasing circulating tryptophan by up to 102% and is thus related to the antidepressant effect of exercise [60]. It has been speculated that in the long term regular physical exercise can replace medication [61], but this needs to be tested in the scientific literature. This habit may be important for three reasons: 1) prevention of possible relapses [62]; 2) for patients with renal problems [decreased glomerular filtration rate] the medications are associated with proteins that are removed by renal route, and in this case may leave an accumulation of toxic metabolites in circulation [63] and 3] such medications may be expensive [64].
Brain-derived neurotrophic factor and physical exercise
In 1982 it was discovered that a protein produced in the hippocampal region called Brain-Derived Neurtrophic Factor [BDNF] exerts neural benefits in pigs [65]. Since then, a number of studies have been done both with animals and humans [65]. The serotonin is modulated by BDNF [66], that is, its low levels are associated with anxiety and depression [67]. The BDNF is related to the following neurological benefits: it increases neuroplasticity and neogenesis, aids in mood regulation, improves memory and synaptic quality, increases neuron survival, and consequently is a protective factor against the development of Parkinson's, Alzheimer's, anxiety, and depression [68]. Due to these neural benefits, it may even be a factor in improving school performance [69].
Exercise is known to increase the production of BDNF, thus serving to protect against the onset of Alzheimer's disease and depression [70]. The intensity of physical exercise seems to be linked with higher production of BDNF [71]. The activities with evidences registered in literature are Crossfit [71], judô [72,73], tai chi [74], boxing, tawkwondo, a running [75], resistance training [76], combined training [aerobic + strength training] [70], basketball [77], a dance [78], yoga and meditation [79]. An interesting study found that intensity in resistance training did not appear to increase production, however, individuals trained longer than 7 weeks produced more BDNF [76].
Due to this mechanism, there are benefits in brain structure. One study when comparing the gray matter structure of competitive level judokas and healthy individuals who do not exercise, greater gray area was observed in judo practitioners (p<0>
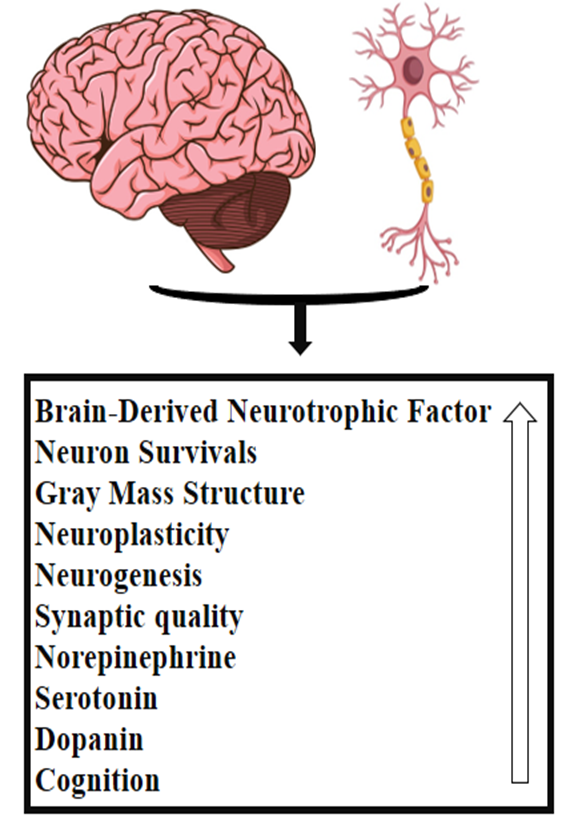
Figure 2: The neural benefits of regular physical exercise.
Some considerations
The studies analyzing the production of serotonin, dopamine, norepinephrine, and BDNF were done via blood collection. In this sense, some of these substances are able to pass the blood-brain barrier and fall into the bloodstream [85]. Alternatively, serotonin also enters the circulation by passing through the intestinal wall to be distributed to the tissues [including the brain] [86]. Studies analyzing brain structure, on the other hand, have used magnetic resonance or diffusion tensor [80–82].
In a cheaper way the studies that propose to investigate the psychological profile of a population use questionnaires. Although Behnke et al. [87] affirm that the use of questionnaires is a valid and reliable method for providing information. It is even a form of use for the diagnosis of psychopathologies in psychiatric clinics (besides the patient report in this case) [88].The limitation is the possibility of volunteers/patients lying due to discomfort and shame. It is up to the doctors and researchers to explain the importance of trust and sincerity in filling out these questionnaires.
Conclusion
There is consensus in the scientific literature of the psychological and neurological benefits of regular exercise, serving to prevent the development of dementia, anxiety, and depression. Exercises predominantly aerobic, anaerobic, or mixed may be viable options. Specifically in this case, it would be interesting to practice the sport to which you feel most motivated so that there is a greater chance of adherence to the practice. Finally, we recommend the practice of physical exercise from childhood to old age (if possible), for which there should be campaigns/strategies to motivate these practices, in addition to access for people of low socioeconomic level.
References
- Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. Available from: http://dx.doi.org/10.1016/S0140-6736(13)61611-61616
Publisher | Google Scholor - Machado T do A, Paes MJ, Alquiere SM, Osiecki ACV, Lirani L da S, Stefanello JMF. Ansiedade estado pré-competitiva em atletas de voleibol infanto-juvenis. Rev Bras Educ Física e Esporte. 2016;30(4):1061–1067.
Publisher | Google Scholor - Durà-Vilà G, Littlewood R, Leavey G. Depression and the medicalization of sadness: Conceptualization and recommended help-seeking. Int J Soc Psychiatry. 2013;59(2):165–175.
Publisher | Google Scholor - LeMoult J, Humphreys KL, Tracy A, Hoffmeister JA, Ip E, Gotlib IH. Meta-analysis: Exposure to Early Life Stress and Risk for Depression in Childhood and Adolescence. J Am Acad Child Adolesc Psychiatry. 2020;59(7):842–855. Available from: https://doi.org/10.1016/j.jaac.2019.10.011
Publisher | Google Scholor - Agumasie M, Dagne B. Prevalence and Factors Associated to Depression among Debre Birhan University Students : A Cross-Sectional Study. J Clin Psychol Ment Heal. 2022;1(1):1–10.
Publisher | Google Scholor - Da Silva Mattos Leite T, Fett CA, Stoppiglia LF, Neves T, Figueiredo KRFV, Rodrigues RAS, et al. Prevalence and factors associated with depression in the elderly: A cross-sectional study. Med. 2020;53(3):205–214.
Publisher | Google Scholor - Twenge JM. Why increases in adolescent depression may be linked to the technological environment. Curr Opin Psychol. 2020;32:89–94. Available from: https://doi.org/10.1016/j.copsyc.2019.06.036
Publisher | Google Scholor - Hawes MT, Szenczy AK, Klein DN, Hajcak G, Nelson BD. Increases in Depression and Anxiety Symptoms in Adolescents and Young Adults during the COVID-19 Pandemic. Psychol Med. 2021;52(14):3222–3230.
Publisher | Google Scholor - Solomou I, Constantinidou F. Prevalence-and-predictors-of-anxiety-and-depression-symptoms-during-the-COVID19-pandemic-and-compliance-with-precautionary-measures-Age-and-sex-matterInternational-Journal-of-Environmental-Research-and-Public-Health.pdf. Int J Environ Res Public Health. 2020;17(14):1–19.
Publisher | Google Scholor - Kuehner C. Why is depression more common among women than among men? The Lancet Psychiatry. 2017;4(2):146–158.
Publisher | Google Scholor - Dean E. Anxiety. Nurs Stand. 2016;30(46):15.
Publisher | Google Scholor - Hammen C. Risk Factors for Depression: An Autobiographical Review. Annu Rev Clin Psychol. 2018;14:1–28.
Publisher | Google Scholor - Chauvet-Gelinier JC, Bonin B. Stress, anxiety and depression in heart disease patients: A major challenge for cardiac rehabilitation. Ann Phys Rehabil Med. 2017;60(1):6–12. Available from: http://dx.doi.org/10.1016/j.rehab.2016.09.002
Publisher | Google Scholor - Zhao R, Yao X. The Relationship between Bullying Victimization and Suicidal Ideation among Chinese Adolescents: The Role of Depressive Symptoms and Gender Differences. J Sch Violence. 2022;21(1):60–80. Available from: https://doi.org/10.1080/15388220.2021.1985327
Publisher | Google Scholor - Kvam S, Kleppe CL, Nordhus IH, Hovland A. Exercise as a treatment for depression: A meta-analysis. J Affect Disord. 2016;202:67–86.
Publisher | Google Scholor - Gerogianni G, Babatsikou F, Polikandrioti M, Grapsa E. Management of anxiety and depression in haemodialysis patients: the role of non-pharmacological methods. Int Urol Nephrol. 2019;51(1):113–118. Available from: http://dx.doi.org/10.1007/s11255-018-2022-7
Publisher | Google Scholor - Jackson EM. Stress Relief: The Role of Exercise in Stress Management. ACSM’s Heal Fittness J. 2013;17(3):14–9.
Publisher | Google Scholor - O’connor PJ, Herring MP, Caravalho A. Mental Health Benefits of Strength Training in Adults. Am J Lifestyle Med. 2010;4(5):377–396.
Publisher | Google Scholor - Duarte JDR da S, Pasa C, Kommers MJ, Ferraz A de F, Hongyu K, Fett WCR, et al. Mood profile of regular combat sports practitioners : a cross-sectional study. J Phys Educ Sport. 2022;22(5):1206–1213.
Publisher | Google Scholor - Wang F, Lee EKO, Wu T, Benson H, Fricchione G, Wang W, et al. The effects of tai chi on depression, anxiety, and psychological well-being: A systematic review and meta-analysis. Int J Behav Med. 2014;21(4):605–617.
Publisher | Google Scholor - Yang JS, Ko JM, Roh HT. Effects of regular Taekwondo exercise on mood changes in children from multicultural families in South Korea: a pilot study. J Phys Ther Sci. 2018;30(4):496–9.
Publisher | Google Scholor - Toskovic NN. Alterations in selected measures of mood with a single bout of dynamic taekwondo exercise in college-age students. Percept Mot Skills. 2001;92:1031–1038.
Publisher | Google Scholor - Roh HT, Cho SY, So WY. Taekwondo training improves mood and sociability in children from multicultural families in South Korea: A randomized controlled pilot study. Int J Environ Res Public Health. 2018;15(4):1–11.
Publisher | Google Scholor - Leyland LA, Spencer B, Beale N, Jones T, van Reekum CM. The effect of cycling on cognitive function and well-being in older adults. PLoS One. 2019;14(2):1–17.
Publisher | Google Scholor - Massey H, Kandala N, Davis C, Harper M, Gorczynski P, Denton H. Mood and well‐being of novice open water swimmers and controls during an introductory outdoor swimming programme: A feasibility study. Lifestyle Med. 2020;1(2):1–12.
Publisher | Google Scholor - Martland R, Korman N, Firth J, Vancampfort D, Thompson T, Stubbs B. Can high-intensity interval training improve mental health outcomes in the general population and those with physical illnesses? A systematic review and meta-analysis. Br J Sports Med. 2022;56(5):279–291.
Publisher | Google Scholor - Tibana RA, Frade De Sousa NM. Are extreme conditioning programmes effective and safe? A narrative review of high-intensity functional training methods research paradigms and findings. BMJ Open Sport Exerc Med. 2018;4(1):1–10.
Publisher | Google Scholor - Rotarou ES, Sakellariou D. Depressive symptoms in people with disabilities ; secondary analysis of cross-sectional data from the United Kingdom and Greece. Disabil Health J. 2018;11(3):367–373. Available from: https://doi.org/10.1016/j.dhjo.2017.12.001
Publisher | Google Scholor - Nixon HL. Constructing diverse sports opportunities for people with disabilities. J Sport Soc Issues. 2007;31(4):417–433.
Publisher | Google Scholor - Grenier M, Kearns C, Grenier M. The benefits of implementing disability sports in physical education: A model for success. J Phys Educ Recreat Danc. 2012;83(4):23–27.
Publisher | Google Scholor - Nemček D. Quality of life of people with disabilities from sport participation point of view. Acta Fac Educ Phys Univ Comenianae. 2016;56(2):77–92.
Publisher | Google Scholor - Wallace JP. Exercise in hypertension: a clinical review. Sport Med. 2003;33(8):585–595.
Publisher | Google Scholor - Musumeci G. Sarcopenia and exercise “the state of the art.” J Funct Morphol Kinesiol. 2017;2(4):1–11.
Publisher | Google Scholor - Daly RM, Dalla Via J, Duckham RL, Fraser SF, Helge EW. Exercise for the prevention of osteoporosis in postmenopausal women: an evidence-based guide to the optimal prescription. Brazilian J Phys Ther. 2019;23(2):170–180.
Publisher | Google Scholor - Alty J, Farrow M, Lawler K. Exercise and dementia prevention. Pract Neurol. 2020;20(3):234–240.
Publisher | Google Scholor - Duarte JDR da S, Ferraz ADF. Studies on martial arts, fights and sports combat with police: a systematic review. Sci Electron Arch. 2022;15(3):77–83.
Publisher | Google Scholor - U.S. Department of Health and Human Services. Physical activity guidelines for Americans. 2nd ed. Vol. 53, US Dept of Health and Human Services. Wasington; 2018. 25 p. 118
Publisher | Google Scholor - Da Silva Duarte JDR, Pasa C, Kommers MJ, De França Ferraz A, Fett WCR, De Oliveira RG, et al. Aspectos motivacionais para a prática do Jiu-Jitsu brasileiro e o Kickboxing em individuos do sexo masculino. Brazilian J Heal Rev. 2021;4(3):12247–12256.
Publisher | Google Scholor - da Silva SM, Duarte JDR da S, Claudino TX, Kommers MJ, Fett WCR, Fett CA. Motivação para a prática do treinamento resistido durante a pandemia. Brazilian Appl Sci Rev. 2022;6(1):107–115.
Publisher | Google Scholor - Duarte JDRDS, Rodrigues HHNP, Cunha MG, De Macedo AF, Salinas JAR, Claudino TX, et al. Dietary intake in kickboxing fighters. Brazilian J Dev. 2021;7(4):42409–42424.
Publisher | Google Scholor - Duarte JDRDS, Oliveira SRDL, Salinas JAR, Tobar KDL, Bueno JCA. The teaching and learning of kickboxing : pedagogical recommendations. Sci Electron Arch. 2023;16(1):55–67.
Publisher | Google Scholor - Polo E, Kruss S. Nanosensors for neurotransmitters Young Investigators in analytical and bioanalytical science. Anal Bioanal Chem. 2016;408(11):2727–2741.
Publisher | Google Scholor - Liu Y, Zhao J, Guo W. Emotional roles of mono-aminergic neurotransmitters in major depressive disorder and anxiety disorders. Front Psychol. 2018;9(NOV):1–8.
Publisher | Google Scholor - Deak A. Brain and emotion: Cognitive neuroscience of emotions. Rev Psychol. 2011;18(2):71–80.
Publisher | Google Scholor - Holloway T, González-Maeso J. Epigenetic mechanisms of serotonin signaling. ACS Chem Neurosci. 2015;15(6):1099–1109.
Publisher | Google Scholor - Nibuya M, Nestler EJ, Duman RS. Chronic antidepressant administration increases the expression of cAMP response element binding protein (CREB) in rat hippocampus. J Neurosci. 1996;16(7):2365–2372.
Publisher | Google Scholor - Dell’Osso B, Palazzo MC, Oldani L, Altamura AC. The noradrenergic action in antidepressant treatments: Pharmacological and clinical aspects. CNS Neurosci Ther. 2011;17(6):723–732.
Publisher | Google Scholor - Taylor C, Fricker AD, Devi LA, Gomes I. Mechanisms of action of antidepressants: From neurotransmitter systems to signaling pathways. Cell Signal. 2005;17(5):549–557.
Publisher | Google Scholor - Sabella D. Antidepressant medications. AJN Am J Nurs. 2018;118(9):1–8.
Publisher | Google Scholor - Domino EF. History of modern psychopharmacology: A personal view with an emphasis on antidepressants. Psychosom Med. 1999;61(5):591–598.
Publisher | Google Scholor - Bayes A, Parker G. How to choose an antidepressant medication. Acta Psychiatr Scand. 2019;139(3):280–291.
Publisher | Google Scholor - Chiang HH, Livneh H, Yen ML, Li TC, Tsai TY. Prevalence and correlates of depression among chronic kidney disease patients in Taiwan. BMC Nephrol. 2013;14(1):1–8.
Publisher | Google Scholor - Irandoust K, Taheri M. Effect of a High Intensity Interval Training (HIIT) on Serotonin and Cortisol Levels in Obese Women With Sleep Disorders. Women’s Heal Bull. 2018;6(1):1–5.
Publisher | Google Scholor - Hamedinia M, Sharifi M, Hosseini-Kakhak A. The effect of eight weeks of aerobic, anaerobic and resistance training on some factor of endocannabinoid system, serotonin, beta-endorphin and BDNF in young men. Biosci Biotechnol Res Asia. 2017;14(3):1201–1210.
Publisher | Google Scholor - Hassan EA-H, Amin MA. Pilates exercises influence on the serotonin hormone, some physical variables and the depression degree in battered women. PilatesfisiosIt. 2011;5(2):89–100.
Publisher | Google Scholor - Lee YK, Cho SY, Roh HT. Effects of 16 weeks of taekwondo training on the cerebral blood flow velocity, circulating neurotransmitters, and subjective well-being of obese postmenopausal women. Int J Environ Res Public Health. 2021;18(20):1–11.
Publisher | Google Scholor - Shabani R, Moazzeni M, Mehdizadeh M. The effect of eight weeks combined resistance - endurance exercise training on serum levels of serotonin and sleep quality in menopausal women. Complement Med J. 2017;07(02):1918–1930.
Publisher | Google Scholor - Davis JM, Alderson NL, Welsh RS. Serotonin and central nervous system fatigue: Nutritional considerations. Am J Clin Nutr. 2000;72:573S-578S.
Publisher | Google Scholor - Höglund E, Øverli Ø, Winberg S. Tryptophan metabolic pathways and brain serotonergic activity: A comparative review. Front Endocrinol (Lausanne). 2019;10:1–11.
Publisher | Google Scholor - Melancon MO, Lorrain D, Dionne IJ. Exercise increases tryptophan availability to the brain in older men age 57-70 years. Med Sci Sport Exerc. 2012;44(5):881–887.
Publisher | Google Scholor - Yuan T-F, Paes F, Arias-Carrión O, Ferreira Rocha N, de Sá Filho A, Machado S. Neural Mechanisms of Exercise: Anti-Depression, Neurogenesis, and Serotonin Signaling. CNS Neurol Disord - Drug Targets. 2015;14(10):1307–1311.
Publisher | Google Scholor - Kim SY, Park JH, Lee MY, Oh KS, Shin DW, Shin YC. Physical activity and the prevention of depression: A cohort study. Gen Hosp Psychiatry. 2019;60(April):90–97. Available from: https://doi.org/10.1016/j.genhosppsych.2019.07.010
Publisher | Google Scholor - Hedayati SS, Yalamanchili V, Finkelstein FO. A practical approach to the treatment of depression in patients with chronic kidney disease and end-stage renal disease. Kidney Int [Internet]. 2012;81(3):247–255. Available from: http://dx.doi.org/10.1038/ki.2011.358
Publisher | Google Scholor - Carracedo-Martínez E, Vázquez-Mourelle R, Figueiras A, Piñeiro-Lamas M. Impact on in- and out-of-hospital drug prescriptions of including a more expensive me-too antidepressant in a hospital drug formulary: a controlled longitudinal study. Pharmacoepidemiol Drug Saf. 2022;31(5):556–565.
Publisher | Google Scholor - Binder DK, Scharfman HE. Brain-derived neurotrophic factor. Growth Factors. 2004;22(3):123–131.
Publisher | Google Scholor - Chang WH, Lee IH, Chi MH, Lin SH, Chen KC, Chen PS, et al. Prefrontal cortex modulates the correlations between brain-derived neurotrophic factor level, serotonin, and the autonomic nervous system. Sci Rep. 2018;8(1):1–10. Available from: http://dx.doi.org/10.1038/s41598-018-20923-y
Publisher | Google Scholor - Zhong F, Liu L, Wei JL, Hu ZL, Li L, Wang S, et al. Brain-derived neurotrophic factor precursor in the hippocampus regulates both depressive and anxiety-like behaviors in rats. Front Psychiatry. 2019;10(JAN):1–11.
Publisher | Google Scholor - Numakawa T, Odaka H, Adachi N. Actions of brain-derived neurotrophin factor in the neurogenesis and neuronal function, and its involvement in the pathophysiology of brain diseases. Int J Mol Sci. 2018;19(11):1–23.
Publisher | Google Scholor - Ramos JM, Galdeano DS. Educação física e o fator neurotrófico derivado do cérebro (BDNF) na aprendizagem escolar. Conexões. 2019;17:1–19.
Publisher | Google Scholor - Dos Santos Trombeta JC, Junior RCV, Cavaglieri CR, Bonfante ILP, Prestes J, Tibana RA, et al. Combined Physical Training Increases Plasma Brain-Derived Neurotropic Factor Levels, But Not Irisin in People Living with HIV/AIDS. Int J Exerc Sci. 2021;14(3):1004–1017.
Publisher | Google Scholor - Tibana RA, de Sousa Neto IV, de Sousa NMF, dos Santos WM, Prestes J, Neto JHF, et al. Time-course effects of functional fitness sessions performed at different intensities on the metabolic, hormonal, and BDNF responses in trained men. BMC Sports Sci Med Rehabil. 2022;14(1):1–11.
Publisher | Google Scholor - Kujach S, Chroboczek M, Jaworska J, Sawicka A, Smaruj M, Winklewski P, et al. Judo training program improves brain and muscle function and elevates the peripheral BDNF concentration among the elderly. Sci Rep. 2022;12(1):1–10. Available from: https://doi.org/10.1038/s41598-022-17719-6
Publisher | Google Scholor - Schor B, da Silva SG, de Almeida AA, Pereira CAB, Arida RM. Plasma brain-derived neurotrophic factor is higher after combat training (Randori) than incremental ramp test in elite judo athletes. Brazilian J Med Biol Res. 2019;52(4):1–8.
Publisher | Google Scholor - Sungkarat S, Boripuntakul S, Kumfu S, Lord SR, Chattipakorn N. Tai Chi Improves Cognition and Plasma BDNF in Older Adults With Mild Cognitive Impairment: A Randomized Controlled Trial. Neurorehabil Neural Repair. 2018;32(2):142–149.
Publisher | Google Scholor - Oztasyonar Y. Interaction between different sports branches such as taekwondo, box, athletes and serum brain derived neurotrophic factor levels. J Sports Med Phys Fitness. 2017;57(4):457–460.
Publisher | Google Scholor - Church DD, Hoffman JR, Mangine GT, Jajtner AR, Townsend JR, Beyer KS, et al. Comparison of high-intensity vs. high-volume resistance training on the BDNF response to exercise. J Appl Physiol. 2016;121(1):123–128.
Publisher | Google Scholor - Moreira A, Aoki MS, De Arruda AFS, Da Silva Machado DG, Elsangedy HM, Okano AH. Salivary BDNF and cortisol responses during high-intensity exercise and official basketball matches in sedentary individuals and elite players. J Hum Kinet. 2018;65(1):139–149.
Publisher | Google Scholor - Rehfeld K, Lüders A, Hökelmann A, Lessmann V, Kaufmann J, Brigadski T, et al. Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS One. 2018;13(7):1–15.
Publisher | Google Scholor - Cahn BR, Goodman MS, Peterson CT, Maturi R, Mills PJ. Yoga, meditation and mind-body health: Increased BDNF, cortisol awakening response, and altered inflammatory marker expression after a 3-month yoga and meditation retreat. Front Hum Neurosci. 2017;11(June):1–13.
Publisher | Google Scholor - Jacini WFS, Cannonieri GC, Fernandes PT, Bonilha L, Cendes F, Li LM. Can exercise shape your brain ? Cortical differences associated with judo practice. J ofScience Med Sport. 2009;12:688–690.
Publisher | Google Scholor - Fontes EB, Augusto C, Gabriela L, Okano AH, Teixeira P, Mara F, et al. Effects of resistance training in gray matter density of elderly. Sport Sci Health. 2017;13(1):233–238.
Publisher | Google Scholor - Teixeira-machado L, Arida RM, Mari JDJ. Neuroscience and Biobehavioral Reviews Dance for neuroplasticity : A descriptive systematic review. Neurosci Biobehav Rev. 2019;96:232–240.
Publisher | Google Scholor - Vivar C, Van Praag H. Running changes the brain: The long and the short of it. Physiology. 2017;32(6):410–424.
Publisher | Google Scholor - Herold F, Törpel A, Schega L, Müller NG. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements – a systematic review. Eur Rev Aging Phys Act. 2019;16(10):1–33.
Publisher | Google Scholor - Brigadski T, Leßmann V. The physiology of regulated BDNF release. Cell Tissue Res. 2020;382(1):15–45.
Publisher | Google Scholor - Yabut JM, Crane JD, Green AE, Keating DJ, Khan WI, Steinberg GR. Emerging Roles for Serotonin in Regulating Metabolism : New Implications for an Ancient Molecule. Endocr Rev. 2018;40(4):1092–1107.
Publisher | Google Scholor - Behnke M, Tomczak M, Kaczmarek LD, Komar M, Gracz J. The Sport Mental Training Questionnaire: Development and Validation. Curr Psychol. 2019;38(2):504–516.
Publisher | Google Scholor - Low DM, Bentley KH, Ghosh SS. Automated assessment of psychiatric disorders using speech : A systematic review. Laryngoscope Investig Otolaryngol. 2020;5(1):196–116.
Publisher | Google Scholor












