

Case Report
Palpitations Due to Atrial Flutter Revealing an Uncommon Association: Non-Compaction of the Left Ventricle, Coronary Sinus Communication and Peri Membranous Communication in a Moroccan Woman at the Age of 57
1Department of Cardiology B, Ibn Sina University Hospital, Mohammed V University, Faculty of Medicine and Pharmacy in Rabat, Morocco.
2 Mohammed V University, Faculty of Medicine and Pharmacy in Rabat, Morocco.
*Corresponding Author: N. Lahmouch, Department of Cardiology B, Ibn Sina University Hospital, Mohammed V University, Faculty of Medicine and Pharmacy in Rabat, Morocco.
Citation: Lahmouch N, Ouacha M, Haidoudi A E, Massri E, Bahri L. (2024). Palpitations Due to Atrial Flutter Revealing an Uncommon Association: Non-Compaction of The Left Ventricle, Coronary Sinus Communication and Peri Membranous Communication in A Moroccan Woman at The Age Of 57, International Clinical Case Reports and Reviews, BioRes Scientia Publishers. 2(3):1-5. DOI: 10.59657/2993-0855.brs.24.021
Copyright: © 2024 Lahmouch Nouhaila, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 28, 2024 | Accepted: September 23, 2024 | Published: September 30, 2024
Abstract
Left ventricular non-compaction (LVNC), also known as hypertrabeculation syndrome, is a rare cardiomyopathy that can occur sporadically or be inherited. LVNC is characterized by a thickened myocardium with prominent trabeculations and deep intertrabecular recesses. While the prevalence of LVNC is not well defined, advancements in diagnostic imaging have improved its detection. This case report presents a rare combination of LVNC with coronary sinus atrial septal defect (ASD) and perimembranous ventricular septal defect (VSD) in a 57-year-old woman who presented with palpitations and dyspnea. Diagnostic evaluations, including echocardiography and cardiac MRI, confirmed the presence of these anomalies. The patient was managed medically, and surgical closure of the coronary sinus ASD was planned. The discussion emphasizes the importance of recognizing LVNC, especially in patients with other congenital heart defects, and highlights the potential role of echocardiography and cardiac MRI in its diagnosis. The report also considers the surgical and transcatheter management options for coronary sinus ASD. Given the potential association between LVNC and congenital heart defects, screening may be beneficial for disease management and long-term follow-up. Future research should focus on large cohort studies to better understand the clinical implications of LVNC and its management.
Keywords: congenital heart defects; left ventricular non compaction; atrial septal defects; flutter
Introduction: Background
Left ventricular non-compaction (LVNC), also known as hypertrabeculation syndrome or spongy myocardium, is a rare condition classified as a primary genetic cardiomyopathy. LVNC can occur sporadically or be inherited within families. While the exact prevalence of LVNC in the general population is unknown, a Swiss review estimated it at 0.014% of echocardiographic studies [1]. However, this figure may be an underestimate due to advancements in echocardiographic imaging and the use of other diagnostic tools like cardiac MRI.
LVNC is not commonly associated with other congenital cardiac anomalies, such as atrial septal defects (ASDs). Coronary sinus ASDs are not true defects; they are characterized by the absence of at least a portion of the common wall between the coronary sinus and the left atrium, resulting in a shunt that is continuous with the coronary sinus opening on the right atrial side of the septum [2]. The perimembranous ventricular septal defect (VSD) is the most common type of ventricular defect. Located in the membranous septum below the crista supraventricularis, it often extends into the muscular septum, where it is commonly referred to as perimembranous. In some cases, the septal leaflet of the tricuspid valve or the membranous septum forms a "pouch" that reduces the shunt and can lead to spontaneous closure [2].
Since congenital heart defects also arise during heart development, there may be potential connections between them and LVNC due to shared genetic abnormalities [3]. Exploring this association could inform clinical practice, as well as research in anatomy, embryology, and genetics aimed at understanding LVNC development.
This case report describes a very rare clinical entity that combines these three conditions, highlighting the importance of echocardiographic recognition.
Here, we present what we believe to be the first case involving a woman who presented a very rare clinical entity that combines these three conditions, highlighting the importance of echocardiographic recognition.
Case Presentation
We report a case of 57-year-old women, followed for hypertension and type 2 diabetes under well-balanced treatment. She previously gaved birth 5 times without resorting to a cesarean section. Her family history was negative for coronary artery disease, heart failure and sudden cardiac death. who presented in our department for palpitations, and dyspnea which had progressed and a paroxysmal nocturnal dyspnea for last 2 months. On examination, bilateral crackles were audible at the lung bases but no cyanosis or clubbing was present without other associated signs of congestive heart failure. Electracardiogram (figure 1) showed a supraventricular tachycardia related to a variable conduction atrial flutter poorly tolerated hemodynamically requiring cardioversion by external electric shock with a return to sinus rythm. On further work-up echocardiogram showed non-compaction of the left ventricle with moderate left ventricular systolic dysfunction LVEF = 45% and the presence of a coronary sinus atrial septal defect measuring 15 mm shunting left-right atrium with an impact on the right cavities with were dilated (RA and RV) associated to a perimembranous interventricular communication closed by an aneurysm of the membranous septum with aligned atrioventricular valves without any LV-RA shunt. All findings, particularly the defect of the interatrial septum, were confirmed by transoesophageal echocardiography TEE (figure 2) without detectable abnormality of pulmonary or systemic venous return. An additional cardiac MRI (figure 3) was carried out confirming an aspect of non-compaction of the left ventricle, involving the different walls of the left ventricle, with respect for the inter-ventricular septum, a dilated left ventricle with mildly reduced EF, a dilated right chamber with a right ventricle with mildly reduced systolic function. The patient was put under medical treatment including diuretic, antiarrhythmic, beta blocker and treatment of heart failure including ACE inhibitor and spironolactone with good clinical evolution.
In a multidisciplinary staff, the discussion of the indication of surgical or percutaneous closure of the communication was discussed with conclusion to a decision of surgical closure by fenestrated patch of the communication in order to prevent a possibility of left decompensation given the field of non-LV compaction in case of complete closure.
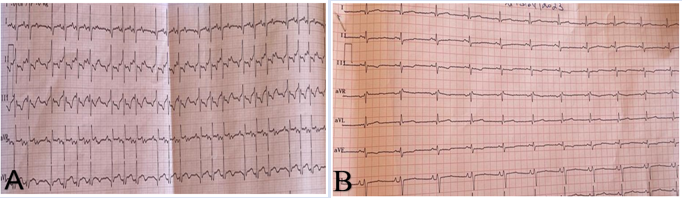
Figure 1: Electrocardiogram (A) showing a variable conduction atrial flutter, (B) showing a return to sinus rythm after external electric shock
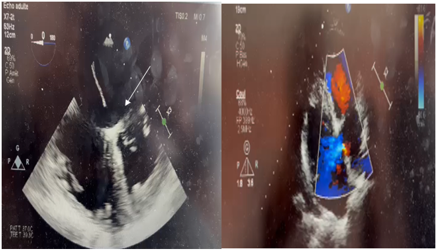
Figure 2: TEE images showing coronary sinus septal defect measuring 15mm (arrow)
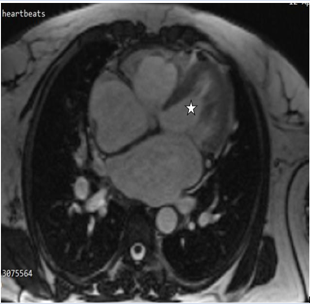
Figure 3: MRI image showing a filled and spongiform left ventricle (star)
Discussion
LVNC is a rare cardiac disorder, classified by the ESC as an unclassified cardiomyopathy [4], characterized by an abnormal ventricular myocardium that contains trabeculae and deep intertrabecular recesses, leading to a thickened myocardium composed of both non-compacted and compacted layers. There is also a direct communication between the left ventricular (LV) cavity and the deep intratrabecular recesses, which fill with blood from the LV cavity without any connection to the epicardial coronary arteries. Although it is rare, non-compacted myocardium has been associated with atrial and ventricular septal defects, as observed in our patient. The primary clinical manifestations of LVNC include congestive heart failure, atrial and ventricular arrhythmias, and thromboembolic events, including stroke [5]. While the Electrocardiogram is typically abnormal, there are no specific characteristic changes associated with LVNC. Echocardiography is commonly the first non-invasive tool. The diagnosis is typically confirmed by identifying prominent trabeculations with a non-compacted to compacted myocardium ratio greater than 2.0 in the short-axis view during end-systole. Transthoracic echocardiography is also effective in detecting related conditions such as muscular ventricular septal defects or other congenital heart diseases [6]. In patients with poor acoustic windows, like those with obesity, contrast echocardiography can enhance diagnostic accuracy by improving the contrast between the myocardium and blood pool.
Cardiac Magnetic Resonance (CMR) imaging, using a steady-state free precession sequence, is often employed to confirm the diagnosis of LVNC when echocardiography results are inconclusive. CMR offers a clearer view of the myocardium and requires a higher non-compacted to compacted ratio, greater than 2.3 at end-diastole, for diagnosis. It also provides better detection of ventricular thrombi and myocardial fibrosis, which are risk factors for arrhythmia [7]. Additionally, CT scans can define increased trabeculations quickly and at a lower cost, though with less detail.
Coronary sinus atrial septal defect (ASD) is a rare congenital anomaly that arises during the development of the sinoatrial region of the heart. Diagnosing this anomaly can often be challenging. Some cases of coronary sinus atrial septal defect (ASD) have been discovered preoperatively, while others were accidentally identified during surgery [8]. The methods for closing coronary sinus ASDs depend on the defect's location and structure. Transcatheter device occlusion has generally been deemed unfeasible for these ASDs due to their proximity to the tricuspid valve and the cardiac conduction system, as well as the insufficient tissue rims needed for device placement. However, Klijima et al. reported successful closures in two patients with coronary sinus ASD without a persistent left superior vena cava. Another study also documented the successful closure of a small coronary sinus ASD [9]. While the specific surgical techniques varied depending on individual anatomical differences, the general approaches included either patch-roofing the coronary sinus within the left atrium to redirect coronary venous and/or left superior vena cava blood to the right atrium or closing the ostium secundum of the coronary sinus to direct blood flow to the left atrium.
Therefore, patients with ventricular or septal defects are at high-risk condition for LVNC, screening might be advantageous for disease management and could influence long-term follow-up after surgery. The recent inclusion of LVNC in the MOGE(S) nosology system highlights that LVNC may contribute to left ventricular dysfunction in conjunction with other morpho functional disorders, such as congenital heart defects.
Conclusion
LVNC is a rare cardiomyopathy that can occur sporadically or be inherited. Its clinical manifestations are diverse, including heart failure, chest pain, thromboembolic events, and atrial and ventricular arrhythmias. Coronary sinus atrial septal defects are typically treated through surgical repair. However, recent advancements in transcatheter techniques indicate that percutaneous device closure might also be a viable option for certain subtypes of coronary sinus atrial septal defects.
Future follow-up studies should be conducted in large groups of living patients, both pediatric and adult, and should incorporate clinical data, including symptoms and examination findings.
Declarations
Competing interests
The authors declare that they have no competing interests.
Funding
This study had no funding from any resource
Acknowledgements
We thank all the people who contributed to the realization of this work.
Authors’ contributions
All authors have contributed to this work and have read and approved the final version
Availability of data and materials
All relevant data generated and analyzed during this study are included in this published article. If it needs any additional information, it is available from the corresponding author on reasonable request.
References
- Jenni R, Oechslin E, Schneider J, et al. (2001). Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart, 86:666.
Publisher | Google Scholor - Houyel, Lucile and Sigolène M Meilhac. (2021). “Heart Development and Congenital Structural Heart Defects.” Annual review of genomics and human genetics, 22:257-284.
Publisher | Google Scholor - Laghari A.H, Tai J.M, Saleem S. (2012). Non-compaction of the left ventricle and associated ventricular septal defect. BMJ Case Rep.
Publisher | Google Scholor - Elliott P, Andersson B, Arbustini E, et al. (2008). Classification of the cardiomyopathies: a position statement from the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J, 29:270.
Publisher | Google Scholor - Oechslin EN, Attenhofer Jost CH, Rojas JR, et al. (2000). Long-term follow-up of 34 adults with isolated left ventricular noncompaction: a distinct cardiomyopathy with poor prognosis. J Am Coll Cardiol, 36:493.
Publisher | Google Scholor - Petersen SE, Jensen B, Aung N, Friedrich MG, McMahon CJ, Mohiddin SA, Pignatelli RH, Ricci F, Anderson RH, Bluemke DA. (2023). Excessive Trabeculation of the Left Ventricle: JACC: Cardiovascular Imaging Expert Panel Paper. JACC Cardiovasc Imaging, 16(3):408-425.
Publisher | Google Scholor - Rao K, Bhaskaran A, Choudhary P, Tan TC. (2020). The role of multimodality imaging in the diagnosis of left ventricular noncompaction. Eur J Clin Invest, 50(9):e13254.
Publisher | Google Scholor - Ootaki Y, Yamaguchi M, Yoshimura N, Oka S, Yoshida M, Hasegawa T. (2003). Unroofed coronary sinus syndrome: diagnosis, classification, and surgical treatment. J Thorac Cardiovasc Surg, 126:1655-1656.
Publisher | Google Scholor - Attenhofer-Jost CH, Connolly HM, Danielson GK, Dearani JA, Warnes CA, Jamil Tajik A. (2007). Clinical features and surgical outcome in 25 patients with fenestrations of the coronary sinus. Cardiol Young, 17:592-600.
Publisher | Google Scholor - Arbustini E, Favalli V, Narula N, Serio A, Grasso M. (2016). Left Ventricular Noncompaction. J. Am. Coll. Cardiol, 68:949-966.
Publisher | Google Scholor














