

Research article
Neurophysiological Grading of Ulnar Nerve Entrapment Across Wrist and Across Elbow
- Salim Hirani 1*
Department of Neurophysiology, Chief Clinical Physiologist, Ysbyty Gwynedd Hospital, Bangor, North Wales.
*Corresponding Author: Salim Hirani, Department of Neurophysiology, Chief Clinical Physiologist, Ysbyty Gwynedd Hospital, Bangor, North Wales.
Citation: H. Salim. (2023). Neurophysiological Grading of Ulnar Nerve Entrapment Across Wrist and Across Elbow, Journal of Brain Research and Neurology, BioRes Scientia Publishers. 2(1):1-5. DOI: 10.59657/2992-9768.brs.23.007
Copyright: © 2023 Salim Hirani, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 04, 2023 | Accepted: September 18, 2023 | Published: October 14, 2023
Abstract
Introduction: Ulnar nerve entrapment across the elbow (UNEAE) and across the wrist (UNEAW) is the second most common entrapment of the hand after carpal tunnel syndrome. There are few grading available for UNEAE and fewer in UNEAW. None of those gradings compares the involvements of both (wrist and elbow). None of the literature looks at the involvement of sensory axonal neuropathy in different stages.
Aim: To see the relation of sensory nerve involvement across the wrist with the entrapment across the elbow and to evaluate its effectiveness in each level without going for any invasive tests like needle EMG examination. To identify the lesion below and across the wrist in terms of support, the clinical Physiologist (CP) grades them properly and helps the consultant decide to treat with conservative or surgical treatment. To compare the recording from the first dorsal interosseous (FDI) muscles with the abductor digiti minimi (ADM) muscle to see which muscle is more sensitive and shows early changes in ulnar nerve entrapment. To differentiate the grading of Guyon’s canal with sensory entrapment below the wrist. To analyse the severity of entrapment in both areas (below/across wrist and elbow). The proposed revised grading system is based on more nuanced, descriptive categories, ranging from "early”, "mild”, "moderate” and "severe”. To create a full grading system of UNEAW and UNEAE some additional clinical grading is proposed.
Method: Data was collected based on the extensive and detailed grading system previously described by Padua. The tests were performed by a qualified clinical physiologist (neurophysiology) using a Key Point 9033A07 machine, used in line with the departmental protocol (peripheral protocol 1, 2022). The Association of Neurophysiological Scientists (ANS) and British Society of Clinical Neurophysiology (BSCN) (2014) guidelines and minimum standards for the practice of clinical neurophysiology in the United Kingdom were followed. All data was recorded numerically to ensure methodological reliability.
Result: The data was collected over one year six months from January 2022 till June 2023. A total of 313 abnormal hands and 200 normal hands were included in this study. Martin Gruber which is a normal variant is not included in this study. Out of 313 abnormal hands, 149 hands were right hand and 164 were left hand included in this study. 46 hand shows lesion below the wrist and 56 hands shows lesion around Guyon’s canal. Across the elbow shows more mild cases as compared to early, moderate, and severe cases. Moderate ulnar nerve across the elbow more associated with sensory axonal and double crush cases were seen more in mild and moderate cases as compared to early and severe.
Conclusion: Findings show that FDI is more sensitive in comparison to ADM to record early changes in ulnar nerve entrapment across the elbow. In addition, the result shows that sensory axonal and double crush need to be included in the grading system which is not included in any present researcher in their published research work.
Keywords: carpal tunnel syndrome; cubital tunnel syndrome; nerve compression; nerve entrapment; radial tunnel syndrome
Introduction
The ulnar nerve is the second most common compressed nerve at the elbow in the region of the cubital tunnel and less frequently at the wrist in Guyon’s canal or below [5]. With the compression of the ulnar nerve, patient complaints can include paranesthesia, numbness, or both, in the small or the ring finger, or in both. In more severe cases, ulnar nerve motor dysfunction will lead to weakness, atrophy, pain across the elbow, and hand clumsiness [6]. Using crutches or walking sticks or plyer-type tools or riding a bicycle on a mountain could cause compression below the wrist which was neglected by most of the researchers.
Reason
The aim of this research is to establish, to see the relation of sensory nerve involvement across the wrist with the entrapment across the elbow and to evaluate its effectiveness in each level without going for invasive tests like needle EMG examination. To identify the lesion below and across the wrist in terms of support, the clinical Physiologist (CP) grades them properly and also helps the consultant in deciding to treat with conservative or surgical treatment.
To compare the recording from the first dorsal interosseous (FDI) muscles with the abductor digiti minimi (ADM) muscle to see which muscle is more sensitive and shows early changes in ulnar nerve entrapment. To differentiate the grading of Guyon’s canal with sensory entrapment below the wrist. To analyze the severity of entrapment in both areas (below/across wrist and elbow). This could support the Surgeon to ascertain the level of severity and decide on a conservative or surgical approach to treatment. Surgeons have to make their own decision about the treatment if they want to consider the treatment on the basis of a Nerve conduction study. There are several primary grading tests mentioned in the literature, such as placing paper between digits IV-V, Tinel sign at wrist or elbow, flexion elbow at 90 ͦ, supinate the forearm, and extending the wrist. These are subjective tests based on the patient’s clinical response. Other tests like Ultrasound, Nerve conduction study (NCS) and Electromyogram (EMG) needle examination are objective tests that have been used for Ulnar nerve entrapment (UNE) which are reliable, evidence-based and objective, and not dependent on the patient’s clinical response [8].
Electrodiagnostic is proving to be an important tool in identifying ulnar nerve lesions across the wrist while or between digits V to mid palm including cubital tunnel syndrome, compression across elbow, and correlation of entrapment in both areas at the same time (double crush syndrome) in different levels and excluding other disorders in the differential diagnosis such as brachial lower trunk plexopathy and C8–T1 radiculopathy [11]. To ascertain the severity and level of entrapment of the ulnar nerve, specific neurophysiological testing is required. There are several investigations specifically related to UNE; [Karvelas [11], Daniele Coraci [6], Solange G. Garibaldi [13], Magdalena Lewanska [12], Laboratoire d’e´lectromyographie p [10], Anthony Chiodo [2], and Carisa Pearce [2]. Most of the grading studies are subjective. Some lack a neurophysiological focus on objectivity during the collection of the data. My previous research paper was associated with lesions across the elbow and other research paper shows the level of ulnar nerve entrapment across the wrist with insufficient clarification in grading[9]. There is no clear guidance to diagnose the ulnar nerve at or below the wrist and in relation to across the elbow published by the British Society for Clinical Neurophysiology (BSCN) or (the Association of the Neurophysiological Scientists (ANS) which are professional bodies in the UK. No clinical assessments will be conducted during the Neurophysiological test so as to eliminate bias of the patient’s condition.
Method
The test will be performed by a qualified Clinical Physiologist (Neurophysiology) using Key Point 9033A07 (Skovlunde, Denmark) machine, on the basis of departmental protocol (Ulnar nerve screening protocol1.2, 2022). A quantitative method will be used for collecting data, to ensure accuracy and to avoid bias. The sample size of patients in the study will be used for all those tested for NCS over a period of one year six months from January 2022 to June 2023, across the population of North Wales. The data will be collected from patients who would be referred to the Neurophysiology department from the Orthopedics and Neurology departments within the local Health Board, as well as General Practices (GPs) in North Wales. No individual patient will be recruited in this research. The inclusion criteria would be considered only on the basis of the referral diagnosis. No clinical assessment will be conducted prior to the study in the department. Referral will be considered based on paranesthesia, pain, and swelling in the ulnar distribution area or digits IV-V or in all fingers. Data will be analyzed on certain widely accepted assumptions of sensory amplitude and CV and distal motor latency (DML), amplitude, and CV [1,3].
Cervical radiculopathy, polyneuropathy or other clinical significance other than ulnar nerve entrapment would be excluded from this research. The procedure began by carrying out the sensory testing, by placing the stimulating ring electrodes on digit III for the median nerve and digit V for the ulnar nerve [4] and the recording electrode on the surface of the wrist to the allocated nerve. The orthodromic technique was used for both sensory and motor NCS tests. A maximal current is applied to record the full response of the nerve, at the digits III for median sensory and digit V for ulnar sensory recording [1]. A maximal current was applied to stimulate median nerve pathways at the wrist and at the elbow for motor recording from abductor pollicis brevis (APB), ulnar nerve pathways from First dorsal interosseous (FDI), and Abductor digiti minimi (ADM) from the wrist, below the elbow and above the elbow. The recording was made from the wrist by stimulating the mid-palm of the ulnar side at a distance of 8cm from the recording electrode, to test if the response from digit V was less than 5µV or absent. The response was recorded from the dorsal ulnar cutaneous nerve (DUCN) if amplitude was less than 5µV or absent between palms to the wrist and digit V to the wrist. Amplitude was recorded from peak to peak for sensory responses, and base to peak for motor responses.
All patient data was collected by fulfilling the criteria mentioned in the above paragraph depending on the severity. The reason for using the above criteria is to describe the full range of severity which was not fully covered by other researchers mentioned earlier in this paper except my previous research paper. The criteria mentioned in the above paragraph are intended to be more reliable from a Clinical Physiologist prospect. Data was collected from the elbow lesion in ulnar nerve pathways and shows signs of Martin Gruber anastomosis, was not included in this research.
Results
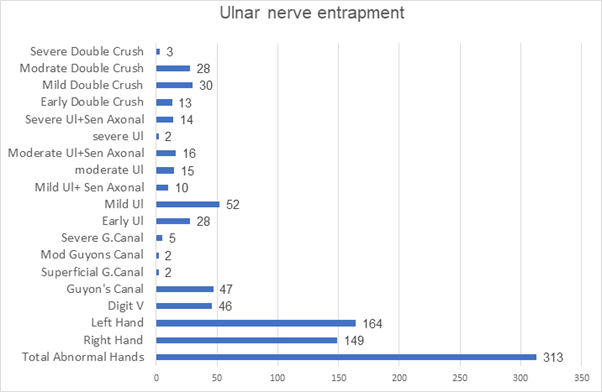
The data will be collected for a period of one year six months from January 2022 to June 2023. A total of 200 normal hands and 313 abnormal hands were included in this study. Out of 313 abnormal hands, 149 were right and 164 were left. 46 hands found a lesion between digit V to mid-palm, 56 hands showed lesions around Guyon’s canal at different levels i.e. 47 hands showed lesions at Guyon’s canal with low amplitude between palm to wrist and digit V to wrist with normal CV, 2 hands shows involvements of superficial area of Guyon’s canal, where CV was slow and normal amplitude, 2 hands shows moderate Guyon’s canal lesion, where slow CV, low amplitude potentials in digit V to mid-palm and digit V to wrist and normal amplitude and CV in dorsal ulnar cutaneous nerve and normal CV across elbow, 5 hands shows absent amplitude and CV between digit V to wrist including mid palm and normal amplitude and CV in dorsal ulnar cutaneous nerve.28 hand falls into early entrapment across elbow where amplitude and CV between digit V to the wrist are normal and also normal CV and amplitude across elbow while recording made from ADM muscles and shows slow conduction velocity with normal amplitude across elbow while recording from FDI muscles. 52 hands fall into the mild category where normal amplitude and CV in sensory nerve and slow conduction between 49-41m/s from FDI and ADM both with normal amplitude. 10 hands show mild ulnar nerve entrapment across the elbow in both FDI and ADM muscles with absent sensory potential including digit to wrist, palm to digit V, and dorsal ulnar cutaneous nerve. 15 hands fall into moderate grading where sensory studies are normal including CV and amplitude and slow CV between 40-31m/s across elbow with normal amplitude. 16 hands show moderate ulnar category with sensory axonal involvements in digit v-wrist including dorsal ulnar cutaneous nerve. 2 hands show severe ulnar nerve entrapment across the elbow with CV below 30 m/s and normal sensory potentials. 14 hands show severe ulnar nerve entrapment with absent sensory potentials, and 74 hands were found who have double crash syndrome where the patient gets legion below and across the wrist and across the elbow in different levels i.e. 13 hands fall into early double crush where sensory nerve shows low amplitude either only between digit V to mid-palm or / as well as low amplitude between mid-palm to wrist with only FDI across elbow show slow CV and normal CV with ADM. 30 hands fall into the category of mild double crush where low amplitude either between digit V to mid palm or digit V to wrist with normal DUC and slow CV in FDI as well ADM across elbow. 28 hands fall into moderate double crush syndrome where either low amplitude and normal or slow sensory CV between digit V-to mid-palm or digit V to the wrist and normal DUC with slow motor CV (30-39 m/s) between both FDI and ADM muscles. Only 3 hands fall into the severe category where sensory potentials show either low amplitude potentials between digit V to mid-palm or digit V to wrist and/or slow CV in that area with severe slow CV (less than 30m/s) across elbow in both FDI and ADM muscles. One case appears to moderate sensory motor Guyon’s Canal with a moderately slow CV across the elbow. I saw only 2-3 cases in the last 20 years of that type. I consider as a rear case and give title type I sensory-motor Guyon’s canal.
Figure
Table
| Hirani Ulnar Grading | Findings |
| Normal | Motor conduction velocity (MCV) ≥50 m/s in FDI and ADM, distal motor latency ≤4.2 ms, amplitude ≥ 5 mV, sensory amplitude ≥ 5µv, and sensory conduction velocity (SCV) ≥ 50 m/s. |
| Type 1- rare case Sensory-motor Guyon’s canal | Distal motor latency >4.5ms, Sensory amplitude >5µv, SCV less than 45m/s, Normal motor amplitude and conduction velocity. |
| Type II Superficial branch of ulnar nerve entrapment | SCV less than 45m/s between palm-wrist and digit V to wrist with normal amplitude. Normal DUC amplitude and CV. Normal DML, amplitude, and MCV. |
| Grade 1, Ulnar Sensory Nerve Entrapment (USNE) between digit V - palm | Ulnar Sensory Nerve Entrapment (USNE) between digit V - palm; Low amplitude sensory potential (less than 4µV), normal amplitude between palm and wrist; normal SCV (greater than 50/sec) across wrist; and normal motor distal latency, amplitude, and MCV across elbow. |
| Grade 2, USNE at Guyon’s canal | USNE at Guyon’s canal; Low amplitude sensory potentials (less than 4µV) between palm to wrist and palm to digit V with normal SCV between palm to wrist and between digit V to palm and normal motor response at wrist and elbow with normal Dorsal Ulnar Cutaneous nerve amplitude and SCV |
| Grade 3, UNEAE - early stage | UNEAE - early stage; MCV across elbow 41-45m/s in FDI or more than 20% drop of CV across elbow and normal in ADM. Normal distal latency, amplitude in ADM and FDI with normal sensory potentials from V and SCV. |
| Grade 4, UNEAE mild motor stage | UNEAE mild motor stage; MCV across elbow 41-49m/s in both FDI and ADM or more than 20% drop of CV across elbow, normal distal motor latency with normal sensory potentials form digit V and normal SCV. |
| Grade 5, UNEAE in a moderate sensory-motor stage | UNEAE in a moderate sensory-motor stage; MCV across the elbow of 30–40 m/s in both FDI and ADM; normal distal motor latency. Sensory potentials shows low amplitude between digit V and mid-palm, palm to wrist. Dorsal ulnar cutaneous nerve may show normal or slow SCV. |
| Grade 6, UNEAE in severe sensory-motor stage | UNEAE in severe sensory-motor stage; MCV across elbow less than 30m/s, normal distal motor latency with absent sensory nerve potentials from digit V, palm to wrist and dorsal ulnar cutaneous nerve. |
Conclusion
Despite the relatively small region of involvements of ulnar nerve entrapment at or below the wrist in moderate to severe levels either across or below the wrist and across the elbow, it has a wide range of clinical presentation that may result in frequent misdiagnosis. The reason is that it is anatomically difficult to differentiate the lesion due to the presence of other nerves in the region of the ulnar nerve. Furthermore, alternative etiology needs to be considered in case of ulnar neuropathy at or below the wrist including double crush involvements. Accurate clinical examination, knowledge of ulnar nerve, and wrist anatomy, and familiarity with possible clinical patterns are essential to making the diagnosis which then can be confirmed with neurophysiology tests and Neuro-imaging. By keeping all the above information, I grade them into 6 grading i.e., Type 1-rare case sensory motor Guyon’s Canal, Type II – Superficial branch of ulnar nerve entrapment, Grade 1- Ulnar sensory nerve entrapment (USNE) between digit V to mid-palm, Grade 2 USEN at Guyon’s Canal, Grade 3 -UNEAE – early stage, Grade 4- UNEAE mild motor stage, Grade 5- UNEAE in moderate sensory-motor stage and Grade 6- UNEAE in severe sensory-motor stage. Below grading with their explanation was given in chart form for understanding. I also added a value chart as well.
Abbreviations
Ulnar nerve entrapment (UNE), Ulnar nerve entrapment across wrist (UNEAW), Dorsal Ulnar cutaneous (DUC), Nerve Conduction Studies -NCS, Betsi Cadwaladr University Health Board -BCUHB, General Practices -GPs, Association of Neurophysiological Scientists - ANS, abductor polices braves - APB, First dorsal interosseous (FDI), sensory conduction velocity - SCV, conduction velocity -CV, Distal Motor Latency - DML, normal sensory amplitude - NSA, Sensory nerve action potentials -SNAP, normal motor amplitude - NMA, Motor nerve action potentials -MNAP, motor conduction velocity – MCV, Normal (N), Palm to wrist (P-W), across elbow (AC/Elbow), Abductor digital minim (ADM).
Declarations
Competing Interests
The authors declare that he has no competing interests.
Author’s Contribution
The Author will contribute by the collection, analysis, and interpretation of data and in writing the manuscript.
Special Thanks
I would like to thank my team who helped and supported me in different ways in completing this research. I would like to say special thanks to Dr. Basheer Kassam and Dr. Gareth Payne for correcting my grammar and boosting my thoughts in relation to finishing this research.
References
- Alfonso C, Jann S, Massa R, Torreggiani A. (2010). Diagnosis, treatment and follow-up of th carpal tunnel syndrome: a review. Neurological Sciences, 31(3):243-252.
Publisher | Google Scholor - Anthony Chiod. (2007). Ulnar Neuropathy at or Distal to the Wrist: Traumatic Versus Cumulative Stress Cases, 88:504-512.
Publisher | Google Scholor - Bland, J. (2000). A neurophysiological grading scale for carpal tunnel syndrome. Muscle Nerve, 23(1):1280-1283.
Publisher | Google Scholor - Carisa Pearce, Joseph Feinberg, Scott W. (2009). Wolfe. HSS journal. 5:180-183.
Publisher | Google Scholor - Dupont C, Cloutier GE, Prevost Y, Dion MA. (1965). Ulnar-tunnel syndrome at the wrist. J Bone Joint Surg Am, 47:757-761
Publisher | Google Scholor - Daniele Coraci, Claudia Loreti & Giulia Piccinini & Pietro E. (1985). Doneddu & Silvia Biscotti & Luca Padua., Ulnar neuropathy at wrist: entrapment at a very “congested” site. Springer Neurological Sciences, 10072: 3446-3447.
Publisher | Google Scholor - Gross MS, Gelberman RH. (1985). and the anatomy of the distal ulnar tunnel. Clin Orthop Relat Res, 196:238-247.
Publisher | Google Scholor - Hirani S, (2023). Neurophysiological grading tool of ulnar nerve entrapment across the elbow. Journal of Neurology, Neurological Sciences and Disorders, 9(1):009-013
Publisher | Google Scholor - Laboratoire d’e´lectromyographie. (2015). Annals of Physical and Rehabilitation Medicine, 58:104-109.
Publisher | Google Scholor - Karvelas and Walker. (2019). Clinical and Ultrasonographic Features of Distal Ulnar Neuropathy: A Review.
Publisher | Google Scholor - Magdalena Lewnska, Jolanta Walusiak-Skorupa. (2017). Is ulnar nerve entrapment at wrist frequent among patients with carpal tunnel syndrome occupationally exposed tomonotype wrist movements? 30(6):861-874
Publisher | Google Scholor - Solange G. Garibaldi, Anamarli Nucci. (2007). Dorsal ulnar cutaneous nerve conduction Reference values. 60(2):349-352.
Publisher | Google Scholor - Shea JD, McClain EJ. (1969). Ulnar-nerve compression syndromes at and below the wrist. J Bone Joint Surg Am,51(6):1095-1103.
Publisher | Google Scholor - Seror P. (2013). Electrophysiological pattern of 53 cases of ulnar nerve lesion at the wrist. Clin Neurophysiol.
Publisher | Google Scholor












