

Case Report
Myopericarditis Due to Cannabis Consumption Mimicking Acute Coronary Syndrome: A Case Report and Literature Review
- Nouhaila Lahmouch *
- Nawal Doghmi
- Latifa Oukerraj
- Mohamed Cherti
Department of Cardiology B, Ibn Sina University Hospital, Mohammed V University, Faculty of Medicine and Pharmacy in Rabat, Morocco.
*Corresponding Author: Nouhaila Lahmouch, Department of Cardiology B, Ibn Sina University Hospital, Mohammed V University, Faculty of Medicine and Pharmacy in Rabat, Morocco.
Citation: Lahmouch N., Doghmi N., Oukerraj L., Cherti M. (2025). Myopericarditis Due to Cannabis Consumption Mimicking Acute Coronary Syndrome: A Case Report and Literature Review, Journal of Clinical Cardiology and Cardiology Research, BioRes Scientia Publishers. 4(1):1-4. DOI: 10.59657/2837-4673.brs.25.041
Copyright: © 2025 Lahmouch Nouhaila, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 04, 2024 | Accepted: December 26, 2024 | Published: January 02, 2025
Abstract
Cannabis consumption is increasing globally, and while its psychotropic effects are well-known, its potential cardiovascular complications are less understood. This case report describes a 30-year-old male with no significant medical history who presented with acute chest pain mimicking acute coronary syndrome. Despite normal coronary angiography, elevated cardiac biomarkers, and imaging findings confirmed a diagnosis of myopericarditis, likely triggered by chronic cannabis use. The patient was treated with aspirin, colchicine, and omeprazole, with good clinical outcomes. This case highlights the importance of considering cannabis use as a potential cause of myopericarditis, especially in young adults presenting with chest pain. Early diagnosis and prompt anti-inflammatory treatment are crucial in managing this condition. Further research is needed to explore the mechanisms behind cannabis-induced myopericarditis and develop targeted therapies.
Keywords: cannabis, myopericarditis, acute coronary syndrome, cardiac MRI
Introduction
Cannabis is the most illegal substance commonly used worldwide. It is consumed in various forms, including smoking, vaporizing, edibles, and concentrates. It is estimated that over 192 million people worldwide use marijuana, making it one of the most commonly used drugs globally [1]. Cannabis contains over 100 different chemical compounds known as cannabinoids. The two most abundant cannabinoids in marijuana are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) [2]. THC is the primary psychoactive compound responsible for the euphoric and mind-altering effects. In order to increase its psychotropic effect, various substances are being added constantly which might hold toxic effects to different organs including the heart and lead to complications such as myopericarditis. The diagnosis of acute myopericarditis is difficult especially when the clinical presentation mimics an acute coronary syndrome.
Case Presentation
A 30-year-old male with no significant past medical history presented to our emergency department with chest pain. The chest pain had started that morning when he woke up. He described it as pressure-like, located on the left side and radiating to the left shoulder. The intensity of the pain was constant. The pain was not positional or reproducible with palpation. The patient denied a recent upper respiratory infection and chest trauma or vaccination. He had no significant medical or surgical history or family history of cardiovascular diseases. However, he endorsed smoking cigarettes and cannabis abuse since the age of 20. He denied any use of other illicit drugs or alcohol. Upon arrival, the patient’s vital signs were within normal limits. Physical examination revealed a regular heart rhythm with no murmurs or rubs. An electrocardiogram showed normal sinus rhythm, slight ST elevation on infero-lateral leads (DII, DIII, AVF, V5 and V6) without image of mirror (Figure 1).
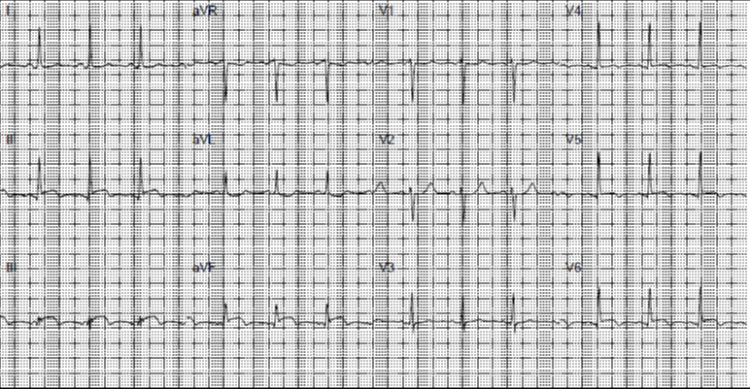
Figure 1: Electrocardiogram showing slight ST segment elevation on inferolateral leads.
Laboratory tests revealed an elevated white blood cell count and cardiac biomarkers, including troponin and creatine kinase. The patient’s initial troponin level was 1500 ng/L. The C-reactive protein (CRP) level of 100mg/l indicating inflammation in the body. The D-dimer was normal in this case, ruling out the presence of a thromboembolic event. An echocardiogram revealed concentric hypertrophy with 55 % LV dysfunction with segmental kinetics disorders and circumferential pericardial effusion. An emergency coronary angiography showed an angiographically healthy coronary network (Figure 2).

Figure 2: Coronary angiography showing normal coronary artery trunk.
Based on the patient’s clinical presentation and laboratory findings, acute myopericarditis was diagnosed. The patient was then admitted to telemetry and evaluated by the cardiology team. Cardiac Magnetic Resonance Imaging (MRI) realized, confirmed the diagnosis of myopericarditis (Figure 3). The patient was started on Aspirin 1g three times a day for 14 days, Colchicine 0.5 mg twice daily for three months, and omeprazole 20mg daily. The patient was advised to follow up with cardiology regularly and to avoid using cannabis and other illicit substances to prevent future episodes of myopericarditis.
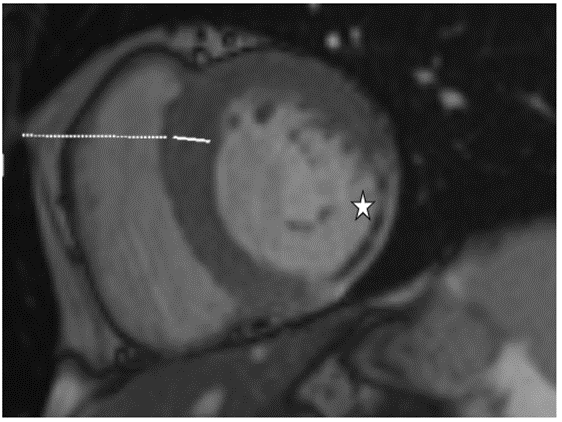
Figure 3: Cardiac Magnetic Resonance Imaging (MRI) showing subepicardial enhancement confirming the diagnoses of myocarditis.
Discussion
Myopericarditis is an inflammatory condition affecting the heart and can present with similar symptoms. The diagnosis of these conditions is based on a combination of clinical presentation, laboratory tests, and imaging studies [3]. The electrocardiogram typically shows widespread ST-segment elevation and PR-segment depression. Echocardiography may reveal pericardial effusion and thickening of the pericardium. Blood tests can show the elevation of markers of inflammation, such as C-reactive protein and erythrocyte sedimentation rate. According to the ESC Guidelines for the Diagnosis and Management of Pericardial Diseases, cardiac MRI should be considered in the diagnosis of acute pericarditis in cases of diagnostic uncertainty, such as when there is no clear evidence of pericardial effusion on echocardiography or when there is suspicion of underlying pericardial disease [4]. However, cardiac MRI is highly routinely recommended in the initial evaluation of acute myocarditis, as echocardiography is usually not sufficient to diagnose and monitor the condition. Coronary angiography, on the other hand, is typically reserved for cases where there is a high suspicion of underlying coronary artery disease or acute coronary syndrome.
In managing myopericarditis induced by marijuana, the choice of medicines depends on the severity of the condition and the individual’s overall health. Treatment aims to reduce inflammation, manage symptoms, and prevent complications. Aspirin is often used to reduce inflammation and relieve pain. In some cases, corticosteroids may be prescribed to reduce inflammation more effectively. Other medications, such as colchicine, may also reduce inflammation and prevent recurrences [5].
The available evidence in the medical literature on managing myopericarditis induced by marijuana is limited. Most of the data comes from case reports and small case series, which makes it difficult to draw definitive conclusions about the best treatment options. Our treatment plan aimed to reduce inflammation, relieve pain, prevent complications, and promote healing of the heart muscle. There are currently no drugs that have been specifically approved for the treatment of myopericarditis. However, several potential new drugs could be beneficial. Future research should focus on understanding the underlying mechanisms of myopericarditis caused by cannabis and identifying new therapeutic targets. It may also be helpful to conduct more extensive clinical trials to evaluate the efficacy and safety of different treatment options. Additionally, more research is needed to understand the long-term cardiovascular risks of cannabis use, particularly in young individuals.
Conclusion
Cannabis use can lead to severe cardiovascular complications, including myopericarditis, even in young adults with no history of heart disease. Healthcare providers should ask about it in chest pain patients, especially young adults, as prompt diagnosis and treatment are crucial in managing myopericarditis. Early administration of anti-inflammatory medications such as aspirin and colchicine can help to reduce inflammation and prevent further damage to the heart muscle.
Declarations
Competing Interests
The authors declare that they have no competing interests.
Funding
This study had no funding from any resource.
Acknowledgements
We thank all the people who contributed to the realization of this work.
Authors’ Contributions
All authors have contributed to this work and have read and approved the final version.
Availability of Data and Materials
All relevant data generated and analyzed during this study are included in this published article. If it needs any additional information, it is available from the corresponding author on reasonable request.
References
- Lafaye G, Karila L, Blecha L, Benyamina A. (2017). Cannabis, Cannabinoids, and Health. Dialogues Clin Neurosci. 19(3):309-316.
Publisher | Google Scholor - ElSohly MA, Radwan MM, Gul W, Chandra S, Galal A. (2017). Phytochemistry of Cannabis Sativa L. Prog Chem Org Nat Prod. 103:1-36.
Publisher | Google Scholor - Goyle KK, Walling AD. (2022). Diagnosing pericarditis. Am Fam Physician. 66(9):1695-702.
Publisher | Google Scholor - Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, et al. (2015). 2015 ESC Guidelines for The Diagnosis and Management of Pericardial Diseases: The Task Force for The Diagnosis and Management of Pericardial Diseases of The European Society of Cardiology Endorsed By: The European Association for Cardio-Thoracic Surgery. Eur Heart J. 36(42):2921-2964.
Publisher | Google Scholor - Algalarrondo V, Boycott H, Eliahou L, Mabille M, Slama MS. (2013). Indications of Anti-Inflammatory Drugs in Cardiac Diseases. Antiinflamm Antiallergy Agents Med Chem. 12(1):3-13.
Publisher | Google Scholor














