

Research Article
Malnutrition in Hospitalized Pediatric Patients with Bronchiolitis at Santa Clara University Hospital-Prevalence Study 2022
1El Bosque University, Bogotá, Colombia.
2Santa Clara University Hospital, Bogotá, Colombia.
*Corresponding Author: Jonathan Alexander Cutta Moreno, El Bosque University, Bogotá, Colombia.
Citation: J.A.C. Moreno, Laura R. Pelaez, Martha L. Baez. (2024). Malnutrition in Hospitalized Pediatric Patients with Bronchiolitis at Santa Clara University Hospital - Prevalence Study 2022, Scientific Research and Reports BioRes Scientia Publishers. 1(4):1-7. DOI: 10.59657/2996-8550.brs.24.026
Copyright: © 2024 Jonathan Alexander Cutta Moreno, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 25, 2024 | Accepted: August 22, 2024 | Published: September 25, 2024
Abstract
Background: Malnutrition affects millions of children worldwide, despite the Sustainable Development Goals, in the year 2022, Colombia faced serious food shortages and malnutrition, especially among children under 5 years of age. According to the National Institute of Health (INS), during that year 308 children under 5 years of age died due to malnutrition and related problems. Considering this situation, it can be observed that malnutrition increases the risk of suffering from respiratory diseases. Among these diseases is acute bronchiolitis, a viral infection that mainly affects infants and is located in the lower respiratory tract.
The objective of this research is oriented to answer: What is the prevalence of acute malnutrition in patients older than 30 days and equal or younger than two years old hospitalized with bronchiolitis in the hospitalization service of Hospital Universitario Santa Clara in the months between February and July 2022?
Methodology: Cross-sectional study or prevalence study, taking as study population, patients older than 30 days and younger than 2 years of age of both sexes requiring hospital management due to bronchiolitis.
Results: From February to July 2022, a total of 183 patients were admitted to the inpatient unit of Santa Clara University Hospital for acute bronchiolitis.
Of these, only 120 met the inclusion criteria proposed in the present study. It was found that at admission 0.8% of the sample were obese, 10% overweight, 10.8% at risk of overweight, 46.7% were in an age-appropriate weight range, 23.3% at risk of acute malnutrition, 5.0% in moderate acute malnutrition and 3.3% in severe acute malnutrition. There was a significant positive correlation between z-score at admission and discharge (R = 0.7996, p < 0.001).
Conclusions: With the development of this research work and the statistical comparisons, we concluded that those patients admitted to the hospitalization unit for acute bronchiolitis, their nutritional status at admission is very variable compared to their nutritional status at discharge, as evidenced by their z-score calculated from weight and height.
Keywords: acute malnutrition; acute bronchiolitis; z-score; hospitalization’ pediatric
Introduction
Children under 2 years of age with bronchiolitis may experience a worsening of their condition and, in some cases, will need immediate hospitalization. Lack of timely care can put the patient at risk of death. When a patient is admitted to the Pediatric Intensive Care Unit (PICU), there is a risk of contracting hospital-acquired infections caused by resistant bacteria that are part of the same context. Currently, there are factors that are associated with the severity and/or complications of bronchiolitis, as well as with a longer duration of hospitalization: prematurity (less than 37 weeks of gestation), with a risk of up to 7.5 times greater than being admitted in the ICU and up to 4 more days of hospital stay; low birth weight; age less than 12 weeks, which carries up to a 10-fold increased risk of prolonged hospitalization; chronic lung disease (bronchopulmonary dysplasia), which involves up to a 5-fold increased risk of ICU admission and/or prolonged stay, and up to a 10-fold increased risk of requiring mechanical ventilation; congenital heart disease, with up to 10 times the risk of being admitted to the ICU and up to 8 times the risk of prolonged hospitalization; immunodeficiency states (anemia, malnutrition); daycare attendance; seasonality; positive result for flu virus; exposure to passive tobacco smoke; and the male sex, among the main ones. Since malnutrition is one of the causes that increase the risk of contagion and complication of bronchiolitis, it is pertinent to delve into the topic and its relationship. However, addressing child malnutrition is hampered by the lack of detailed information at the departmental and municipal levels, as well as the complexity of measuring and analyzing this phenomenon due to the large number of factors that cause it. It is necessary to implement complex statistical operations and precise standards, taking into account their relationship with the disease. Currently, malnutrition in children is recognized as a public health problem, since 45% of deaths in minors are linked to this condition. The main causes include poverty, inequality, political conflicts, wars between countries and natural disasters, which cause food crises and limit children's access to adequate food, according to reports from the UN Refugee Agency. (UNHCR) in 2020. In Latin America, the Food and Agriculture Organization of the United Nations (FAO) noted in 2022 that the poorest 20% of children suffer high levels of malnutrition, due to changes in patterns. food problems that affect the most marginalized communities. These communities have difficulties accessing healthy foods with high protein and vitamin content, which has led to an increase in the consumption of carbohydrates and fats, since these products are cheaper and more accessible. Understanding the relationship between malnutrition and bronchiolitis is crucial for developing public health prevention and treatment strategies. Identifying children at risk of malnutrition and providing them with appropriate nutritional care can help reduce the incidence and severity of bronchiolitis. Furthermore, addressing malnutrition in children with bronchiolitis can improve their response to treatment and reduce the burden of the disease at both the individual and public health levels.
Methodology
Study Type
A cross-sectional or prevalence study was carried out.
Malnutrition in Hospitalized Pediatric Patients with Bronchiolitis at Santa Clara University Hospital.
Reference Population and Sample
Reference Population
Patients older than 30 days and younger than 2 years of age of both sexes who require hospital management due to bronchiolitis.
Sample Size
Convenience sampling, since all patients with a diagnosis of bronchiolitis who have been hospitalized and who have a complete medical record in the clinical history will be included.
Inclusion and Exclusion Criteria
Inclusion Criteria
Patients older than 30 days and younger than 2 years of age of both sexes with a diagnosis of bronchiolitis.
Patients requiring hospital management due to respiratory pathology.
Exclusion criteria
Patients who meet the following criteria will be excluded. Patients with underlying gastrointestinal diseases (cystic fibrosis with gastrointestinal manifestations, short bowel syndrome, celiac disease, inflammatory bowel disease, metabolic diseases). Patients with underlying neurological diseases (cerebral palsy, structural epilepsy, sequelae of hypoxic ischemic encephalopathy, neurodevelopmental disorders such as autism spectrum disorder). Patients with pulmonary malformation.
Genetic syndrome
Chronic pulmonary pathologies such as CF. Pathologies that have a chronic underlying pathology with underlying malnutrition, such as: Short bowel syndrome Prematurity.
Biases and bias control
Information bias: Collection by persons other than the researchers.
Evaluate the profile of the person who takes the measurements and collects the information, thus making it possible to determine the suitability and veracity of the information.
Selection Bias: Difference between participants and non-participants
To avoid selective data collection, consciously or unconsciously, anthropometric measurements and data collection will be performed on 3 random days spaced 10 days apart, and this will be subject to the number of patients hospitalized in the unit at the time the measurement is taken.
Observer: The researchers themselves will collect the information, fill out the forms, and feed/analyze the database through the designed instrument.
Each week, the methodological tutor will verify the quality of the data.
Instrument: A format will be created in EXCEL to facilitate the collection and verify the quality of the data. This format will include all the variables and will adequately explain how to collect each one of them.
Data/information collection techniques
The medical records of the target population hospitalized at the Santa Clara University Hospital were used to systematize the information and create the corresponding databases.
Procedure for information collection
After selecting the research topic, the research question was developed. A literature search was conducted in order to construct the research protocol so that it could be submitted to the research committee and the research ethics committee. Once approval is obtained from the ethics committee, we will proceed to collect the information from the Clinical Nutrition program of the Hospital Universitario Santa Clara, available in the form of a database. This information will be filtered by ICD 10 diagnosis. Based on the initial filters, the available clinical history will be reviewed depending on the place of care and will be classified according to the origin of the patients attended. Subsequently, the classification of the data in the clinical history will begin according to the variable’s manual. The data will be entered in a self-authored form created in Microsoft Excel with pre-digitized options, so that a spreadsheet with pre-validated data can be downloaded at the end of data collection. This database will be anonymized and sent to the methodological advisor, who will be in charge of performing the statistical analysis in the Stata software. Once the data have been analyzed, the final technical report and scientific article will be prepared for subsequent submission.
Instruments to be used
The information will be collected in an Excel database in which no data that could identify patients will be included; this database will be protected with passwords that only the researchers will have access to and subsequently this database will be analyzed under the statistical program STATA version 16.
Methods for data quality control
The principal investigator conducted a pilot study to verify the patient inclusion data, obtain the data from the clinical history or from the database provided by the Hospital Universitario Santa Clara, standardizing the procedure in Excel version 2010 and using checkboxes to document each variable of the patients included in the study.
Variables
The variables in this study are divided into 3 large groups: the first are sociodemographic variables of the population diagnosed with malnutrition. The second group refers to clinical characterization variables and the last group are variables related to the episode of malnutrition and possible associated factors (see Table 1).
Table 1: Descriptive analysis of the population Total.
| N=120 |
| Acute malnutrition 10 (8.3%) |
| Female 72 (60.0%) |
| Admission Weight, Kg 6,395 (5.25-8.05) |
| Size upon Admission, Cm 63 (57.5-71) |
| Entry Z Score -.395 (-1.26-.79) |
| Weight for Height Ratio (P/T) Obesity (>+3) 1 (0.8%) |
| Overweight (> +2 A ≤ +3) 12 (10.0%) |
| Risk of Overweight (> +1 to ≤ +2) 13 (10.8%) Appropriate weight for height (≥-1 to ≤+1) 56 (46.7%) |
| Risk of Acute Malnutrition (≥-2 to <-1) 28 (23.3%) |
| Moderate Acute Malnutrition (<-2 to ≥-3) 6 (5.0%) |
Analysis Plan
A descriptive analysis of the information will be performed. Quantitative variables will be summarized by means of measures of central tendency and dispersion, for which the normality assumption will be checked using the Shapiro-Wilk test. Qualitative variables will be summarized using relative and cumulative frequencies represented by percentages.
Results
From February to July 2022, a total of 183 patients were admitted to the inpatient unit of Santa Clara University Hospital due to acute bronchiolitis. Anthropometric stratification based on z- score was performed using weight and height at admission and discharge. After reviewing the medical records, 63 patients who did not meet the inclusion criteria were excluded, leaving a final sample of 120 patients. Of the 120 patients included in the study, 60% were women, corresponding to 72 patients, and the rest were men. Weight at admission ranged between 5.25 and 8.05 kilograms, with a z-score that ranged between -1.26 and 0.79 standard deviations, compared to the z-score at discharge that remained between -1.72 and -4.95 (see Table 2).
In relation to the income nutritional classification according to the World Health Organization, 0.8% of the sample was found to be obese, 10% overweight, 10.8% at risk of overweight, 46.7% in an adequate weight range for age, 23.3% at risk of acute malnutrition, 5.0% in moderate acute malnutrition and 3.3% in severe acute malnutrition (see Table 2).
Only 15% of the patients attended day-care centers on a regular basis. The predominant socioeconomic stratum was stratum 1, with 69.2% of the total sample, equivalent to 102 patients. In addition, 85% of the families were biparental, consisting of mother and father (see Table 2).
A significant positive correlation was found between the z-score at admission and discharge of patients (R = 0.7996, p lessthan 0.001). This indicates that patients who were admitted with a higher or lower z-score in relation to weight and height also showed a correspondingly high or low z-score at discharge. This finding suggests that nutritional status at admission is closely related to nutritional status at discharge, highlighting the importance of the initial evaluation in the clinical evolution of patients (see figure 1). During the period studied, a significant variation in the frequency of cases of acute malnutrition was identified between the different months at the Santa Clara University Hospital. May stood out as the month with the highest number of patients diagnosed with acute malnutrition, registering a total of 38 cases. In comparison, only 1 case of acute malnutrition was detected in January, indicating a clear disparity in incidence throughout the year.
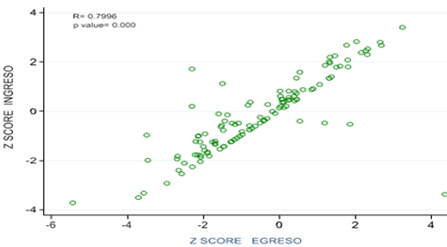
Figure1: Distribution of Z Score entry vs Z Score exit.
The months of June and July also showed a notable prevalence of acute malnutrition, following the pattern observed in May. This descending order of frequency reflects a consistent trend during the study period (see Figure 2).
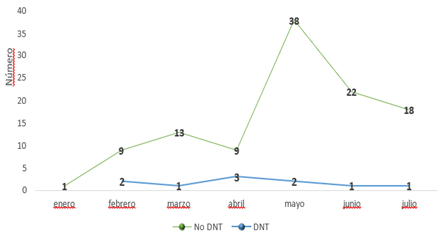
Figure2: Number of patients seen monthly with bronchiolitis according to malnutrition classification yes-no.
Based on the comparison made between the z score at admission and discharge, it was found that 100% of the patients who were obese (> +3) remained the same, with no change in their condition, while those who were overweight (+2 to ≤ +3) remained the same: 58.3% of individuals remained in the same overweight condition while 41.7% of individuals improved, managing to get out of the overweight category. Regarding the risk of Overweight (+1 to ≤ +2): 15.4% of individuals worsened, moving into a more overweight or obese category, while 69.2% of individuals remained the same in the overweight risk category. Weight Adequate for Height (≥ -1 to ≤ +1): 23.2% of individuals worsened, possibly falling into overweight or malnutrition categories and 76.8% of individuals remained at adequate weight for height, risk of acute malnutrition (≥ -2 to < -1): 39.3% of individuals worsened, progressing to acute malnutrition and 60.7% of individuals remained at risk of acute malnutrition.
In moderate acute malnutrition (≤ -2 to ≥ -3): 100% of individuals in this category remained the same, with no change in their moderate malnutrition status, while in severe acute malnutrition (< -3): 100% of individuals in this category remained the same, with no change in their severe malnutrition status. (See Figure 3). The outcome of most individuals in the different nutritional categories remained the same, with notable improvements in the overweight category. However, it is of concern that in the categories of moderate and severe acute malnutrition no improvements were observed.
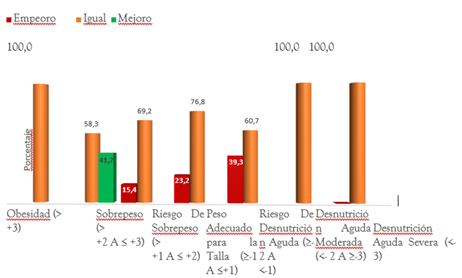
Figure4: Distribution of Z Score entry vs. exit Z score.
Discussion
Nutrition is a fundamental pillar for development in the early stages of life (McDonald, Gross, McLachlan, Jukes, & McGuire, 2006). Several studies have shown that nutrition during the first two years of life significantly influences cognitive development (Calceto-Garavito, Garzón, Bonilla, & Cala-Martínez, 2019; Hernando-Requejo, 2016). The diversity of manifestations of malnutrition is evident in numerous countries (Márquez-González, et al., 2012). Malnutrition is a risk factor for the development of respiratory diseases. One of these diseases is acute bronchiolitis, a viral infection that often affects infants and is located in the lower respiratory tract. The present study evaluated the nutritional status of 120 pediatric patients hospitalized for acute bronchiolitis at the Santa Clara University Hospital from February to July 2022, the evaluation was performed by anthropometric stratification based on the weight-for-height z- score both at admission and discharge. Of the patients admitted for acute bronchiolitis, 0.8% of the sample were obese, 10% were overweight, 10.8% were at risk of overweight, 46.7% were in an adequate weight-for-age range, 23.3% were at risk of acute malnutrition, 5.0% were in moderate acute malnutrition and 3.3% were in severe acute malnutrition. Although there is no specific description of the relationship between nutritional status and acute bronchiolitis in the literature, it was found that those patients who were admitted with bronchiolitis in the weight-for-height range in 23.2% of the patients had a significant decrease in weight-for-height. Of the total of those admitted in the malnutrition range, 39.3percentage decreased their z-score, placing them in moderate and severe acute malnutrition respectively; it should be noted that those who were admitted with moderate or severe acute malnutrition did not change with respect to discharge. In general, the results of the present study show that most of the patients maintained their nutritional status during hospitalization. However, it is of concern that no alterations were observed in the categories of moderate and severe acute malnutrition. These findings highlight the need to implement effective and targeted nutritional interventions to improve these outcomes. In addition, the high correlation between the z-score at admission and discharge suggests that interventions should be initiated as early as possible during hospitalization, and this temporal variation suggests the presence of external factors that can significantly influence the nutritional status of patients. I believe that studies with greater statistical power are needed to really understand what external factors influence nutritional status in patients admitted for acute bronchiolitis. This study is a starting point that allows us to promote research work at the Santa Clara University Hospital, aimed at creating studies that provide scientific evidence that will allow us to create strategic nutritional plans and improve clinical practice in the country.
Conclusion
With the development of this research work and the statistical comparisons, we concluded that those patients admitted to the hospitalization unit for acute bronchiolitis, their nutritional status at admission is very variable compared to their nutritional status at discharge, as evidenced by their z-score calculated from weight and height. A positive relationship between the z-score at admission and the z-score at discharge was found to be statistically significant. We were able to show that those who were admitted with a classification of adequate weight for height and risk of acute malnutrition decreased their z-score significantly with respect to their admission z-score, while those who were in moderate and severe acute malnutrition did not have any type of variation. This motivates us to carry out research studies with larger sample populations that allow the implementation of nutritional interventions in order to minimize the nutritional alterations that are evidenced in the z-score.
Declarations
Conflict of interest statement
The authors declare no conflict of interest. For the present work, the copyright belongs to Hospital Universitario Santa Clara and Universidad El Bosque.
Ethics statement
Following the basic principles of the Declaration of Helsinki, developed by the World Medical Association, which establishes ethical principles for medical research involving human subjects, and given that this work involves the review of medical records, "the right of individuals to safeguard their integrity is respected, taking necessary precautions to protect the privacy of individuals and minimize the impact of the study on their physical and mental integrity and personality."
The protocol was approved by the ethics committee of Santa Clara University Hospital. It was considered a low‐risk study since no modification or intervention was made in the management received by the patient in clinical practice
Transparency statement
The lead author Jonathan Cutter Moreno affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Consent for Publication
Not applicable
Acknowledgments
I would like to express my gratitude to Universidad el Bosque for allowing us to be part of its community and contributing to the growth of its reputation.
We extend our gratitude to the Hospital Universitario Santa Clara for providing an excellent environment for medical practice and allowing us to work together for the benefit of the patients who attend the institution.
Special thanks to Drs. Laura Rocio Pelaez and Martha Lucia Baez, my mentors and outstanding professionals, for their support and guidance based on their experience for the completion of this work.
Finally, I would like to thank my parents, partner and brother, since they are the people who with their love and patience have accompanied us and provided the strength to persevere and complete our research, overcoming all obstacles and adversities.
Data availability statement
Data supporting the conclusions of this study are available from the corresponding author upon reasonable request and through the supplementary documents. If you need the data, or if you wish to review the protocol.
Funding
The author declares that the research was conducted in the absence of commercial or financial relationships that could be construed as a potential conflict of interest.
Authors' contributions
Jonathan Cutta Moreno: Conceptualization; data curation; formal analysis; investigation; methodology; supervision; validation; writing—original draft; writing—review & editing. Laura Rocio Pelaez: Conceptualization; formal analysis; supervision; visualization. Martha Lucia Baez: Conceptualization; investigation; methodology; project administration; supervision, validation
References
- Bueno, M., & Sarría, A. (2003). Malnutrición del lactante. Madrid.
Publisher | Google Scholor - Calceto-Garavito, L., Garzón, S., Bonilla, J., & Cala-Martínez, D. (2019). Relación del Estado nutricional con el desarrollo cognitivo y psicomotor de los niños en la primera infancia. Revista ecuatoriana de neurologia, 28(2):50-58.
Publisher | Google Scholor - Coronel-Carvajal, C. (2019). Factores asociados al desarrollo de la bronquiolitis. Revista Archivo Médico de Camagüey, 23(5):639-647.
Publisher | Google Scholor - De la Cuesta, R. M., del Villar Guerra, P., Villanueva, A. M., Alaport, V. M., Norniella, C. M., Albistegui, M. J., & González, V. G. (2020). CPAP vs oxigenoterapia convencional en lactantes trasladados por insuficiencia respiratoria. In Anales de Pediatría, 93(3):L152-L160.
Publisher | Google Scholor - Defensoría Delegada para la Infancia, l. J. (2023). Reporte desnutrición en niños y niñas menores de 5 años de edad en Colombia. Bogotá, Colombia.
Publisher | Google Scholor - Farrugia, P., Petrisor, B. A., Farrokhyar, F., & Bhandari, M. (2010). Research questions, hypotheses and objectives. Canadian journal of surgery, 53(4), 278.
Publisher | Google Scholor - Fuentes, C., Cornejo, G., & Bustos, R. (2016). Actualización en el tratamiento de bronquiolitis aguda: menos es más. Neumología Pediátrica, 11(2):65-70.
Publisher | Google Scholor - Hernando-Requejo, V. (2016). Nutrición y deterioro cognitivo. Nutrición hospitalaria, 33: 49-52.
Publisher | Google Scholor - Lorca Cámara, V. (2020). Efecto del cambio climático en la alimentación de los países en desarrollo.
Publisher | Google Scholor - Márquez-González, H., García-Sámano, V. M., de Lourdes Caltenco-Serrano, M., García-Villegas, E. A., Márquez-Flores, H., & Villa-Romero, A. R. (2012). Clasificación y evaluación de la desnutrición en el paciente pediátrico. El residente, 7(2):59-69.
Publisher | Google Scholor - Martinón-Torres, F., Núñez, A. R., & Sánchez, J. M. (2001). Bronquiolitis aguda: evaluación del tratamiento basada en la evidencia. In Anales de Pediatría, 55(4)345-354.
Publisher | Google Scholor - McDonald, B. H., Gross, L., McLachlan, R., Jukes, M., & McGuire, M. (2006). Nutrición: la base para el desarrollo.
Publisher | Google Scholor - McLaren, D. (1976). Protein Energy Malnutrition (PEM). Textbook of Pediatric Nutrition, 105-117.
Publisher | Google Scholor - Orejón de Luna, G., & Fernández Rodríguez, M. (2012). Bronquiolitis aguda. Pediatría Atención Primaria, 14:45-49.
Publisher | Google Scholor - Oviedo, C. P., & Viteri, J. S. (2015). Pregunta de investigación y estrategia PICOT. Medicina, 19(1):66-69.
Publisher | Google Scholor - Parra, A., Jiménez, C., Hernández, S., García, J. E., & Cardona, Á. M. (2013). Bronquiolitis: artículo de revisión. Neumología pediátrica, 8(2):95-101.
Publisher | Google Scholor - Pérez, P. R., de Tejada, E. O., & Rodríguez, M. J. (2010). Bronquiolitis en pediatría. Información Terapéutica del Sistema Nacional de Salud, 34(1):3-11.
Publisher | Google Scholor - Ramos, G. (1998). Desnutrición. México.
Publisher | Google Scholor - UNICEF; OMS; Banco Mundial. (2023). Levels and trends in child malnutrition: UNICEF / WHO / World Bank Group Joint Child Malnutrition Estimates: Key. Nueva York.
Publisher | Google Scholor - Véliz Barzola, R. A. (2017). Evaluación nutricional en niños menores de 5 años con infecciones del tracto gastrointestinal en el Hospital Universitario de Guayaquil, período 2015-2016. Doctoral dissertation, Universidad de Guayaquil. Facultad de Ciencias.
Publisher | Google Scholor - Zhang, L., Mendoza-Sassi, R. A., Wainwright, C. E., Aregbesola, A., & Klassen, T. P. (2023). Nebulised hypertonic saline solution for acute bronchiolitis in infants. Cochrane database of systematic reviews, (4).
Publisher | Google Scholor










