

Research Article
Lymphopenia in Patients with Glioblastoma: Literature Review and Case Presentations
- Sofia Sklyar 1
- Darya Sitovskaya 2,3*
- Yulia Mirolyubova 2
- Victoria Kushnirova 1
- Bobir Safarov 4
- Konstantin Samochernykh 1
1Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, Saint-Petersburg, Russia.
2Almazov National Medical Research Centre, Saint-Petersburg, Russia.
3Federal State budgetary Educational Institution of Higher Education St. Petersburg State Pediatric Medical University, Saint-Petersburg, Russia.
4Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan.
*Corresponding Author: Darya Sitovskaya, Almazov National Medical Research Centre, Saint-Petersburg, Russia.
Citation: Sklyar S, Sitovskaya D, Mirolyubova Y, Kushnirova V, Safarov B, et al. (2024). Lymphopenia in Patients with Glioblastoma: Literature Review and Case Presentations. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3(3):1-8. DOI: 10.59657/2992-9989.brs.24.029
Copyright: © 2024 Darya Sitovskaya, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 26, 2024 | Accepted: July 15, 2024 | Published: July 19, 2024
Abstract
Interest in studying the functioning of the adaptive immune system in malignant gliomas has recently emerged. Numerous studies have been conducted to analyze the local immune status. Currently, glioblastoma is considered an immunologically "cold" tumor, characterized by low levels of lymphocyte infiltration and the presence of various local mechanisms that suppress and evade activated immune cells. The study of the systemic component of the immune response in malignant gliomas is still in its early stages. Lymphopenia, a condition characterized by low levels of lymphocytes, has been observed in patients with glioblastomas, not only as a result of medical treatment, but also due to the tumor itself. In this review, we present three clinical cases that assess the lymphocyte subpopulation in the peripheral blood and the infiltration of immune system cells into the tumor. We also discuss potential immunotherapy options for this group of patients, taking into consideration the unique functioning of the immune system in glioblastomas.
Keywords: glioblastoma; lymphopenia; T-lymphocyte
Introduction
There is no denying the fact that the adaptive immune system plays a crucial role in recognizing and eliminating cancer cells [1,2]. However, tumors have developed various mechanisms to evade the activated immune system. Cancer is now recognized as a pathological process characterized by uncontrolled cell proliferation, migration of tumor cells, and suppression of the immune system [3-5]. While it was previously believed that the central nervous system (CNS) was an immunologically privileged environment, recent research has shown otherwise. Studies have revealed the presence of functioning lymphatic vessels in the meninges, described pathways for the "exit" of antigens from the brain into the deep cervical lymph nodes, determined the phagocytic and antigen-presenting properties of microglia, established the infiltration of activated T-lymphocytes in pathological foci in the brain parenchyma, and identified the glymphatic system [6-10]. As a result, the central nervous system is now considered an immunologically dynamic system rather than a privileged one. These scientific advancements, along with the recognition of immune control of tumors, have raised questions about the functioning of the immune system in central nervous system tumors and the potential for its activation. Of particular interest is glioblastoma, the most common and malignant intracerebral tumor of the central nervous system. Despite the use of standard complex treatments, such as immunotherapy with checkpoint inhibitors, clinical trials have shown mixed results in terms of efficacy [6,11-12]. This highlights the need for further research and the development of new, effective treatment methods [13-17].
Glioblastoma is known to be an immunologically “cold” tumor, meaning that it has a low level of infiltration by activated immune cells [18]. The reason for this is not clear. Some researchers believe that the low infiltration of T-lymphocytes in glioblastoma is due to the high expression of inhibitory receptors on tumor cells [19,20]. Other studies suggest that the tumor microenvironment creates an immunosuppressive environment that hinders the activity of T-lymphocytes [21,22]. However, it is possible that the dysfunction of T-lymphocytes is caused by a decrease in their numbers due to treatment with dexamethasone, a drug commonly used to reduce cerebral edema, or specific anti-tumor treatments. Further research on this topic will not only enhance our understanding of the pathogenesis of glioblastoma, but also aid in determining the most effective methods of immunotherapy for this highly malignant central nervous system tumor.
Materials and Methods
The study was conducted at the Neurosurgical Department No. 4 of the Polenov Neurosurgical Institute. The Pathology Department and the Central Clinical Diagnostic Laboratory of the Almazov National Medical Research Centre were also involved in the study. The main objective of the study was to analyze lymphocyte subpopulations in peripheral blood and assess tumor infiltration by activated lymphocytes. The study included two male patients over the age of 18 who were diagnosed with supratentorial glioblastoma. Both patients provided informed consent to participate in the study, which was conducted in accordance with the Helsinki Declaration of Human Rights. The histological conclusion was based on the 2021 WHO classification of CNS tumors [11]. It is important to note that both patients underwent primary neurosurgical tumor removal. The study also took into consideration whether the patients received symptomatic therapy with dexamethasone at the time of blood donation. The clinical and demographic characteristics of the study group are presented in Table 1.
Table 1: Clinical and Demographic Characteristics of Patients with Glioblastoma.
| Patient | Age | Gender | Stage of treatment | Prescribing dexamethasone before taking a blood sample | Number of days of dexamethasone therapy |
| No 1 | 76 | m | ST | yes | 14 |
| No 2 | 63 | m | ST | no | – |
Note: m–man, w–woman, ST–surgical treatment, CT–chemotherapy.
The biopsy material was examined by fixing tumor fragments in 10% buffered formalin, dehydrating them in a standard manner, and embedding them in paraffin. Histological sections were stained with hematoxylin and eosin, and the results of immunohistochemical (IHC) reactions with antibodies to GFAP, IDH1r132h, and a marker of proliferative activity Ki67 were studied in patients no 1 and no 2. In patient no 1, antibodies from Dako (USA) and the EnVision imaging system were used to study CD45, CD3, CD4, CD8, and CD20. Histological analysis and microphotography were performed using a Leica DM2500 M microscope equipped with a DFC320 digital camera and an IM50 image manager (Leica Microsystems, Wetzlar, Germany). Lymphocyte infiltration in the tumor and perifocal zone (if present) was assessed using a semi-quantitative method, with a scale of 0 (no staining), 1+ (single cells in 1 mm2 of tissue), 2+ (10-20 stained cells in 1 mm2), and 3+ (>30-stained cells per 1 mm2). The data are presented in mean and standard deviation format.
Lymphocyte subpopulations were assessed in a venous blood sample collected the day before surgery. The main subpopulations of lymphocytes were determined using quantitative flow cytometry on a BD FACS Aria analyzer (manufactured by Becton Dickinson, USA). The standard panel for lymphocyte subpopulations included monoclonal antibodies to CD45, CD3, CD4, CD8, CD19, CD16, and CD56 (manufactured by Becton Dickinson, USA). The total number of lymphocytes, including T cells (CD3+/CD45+), cytotoxic T cell (CD3+CD8+/CD45+), T-helper cells (CD3+CD4+/CD45+), NK cells (CD3-CD16+CD56+/CD45+), and B lymphocytes (CD19+/CD45+), was determined. The results were compared with reference values and scientific literature data.
Results
The results of laboratory tests are presented in Table 2, shows the main subpopulations of lymphocytes in the peripheral blood of patients with glioblastoma.
Table 2: The main subpopulations of lymphocytes in the peripheral blood of patients with glioblastoma.
| Patient | Lymphocyte total | T cells (СD3+/ CD45+) | Cytotoxic T cell (CD3+CD8+/ CD45+) | T-helper cells (CD3+CD4+/ CD45+) | B cells (CD19/ CD45+) | Ratio CD4+/CD8+ | NK cells |
| cells/μl | cells/μl | cells/μl | cells/μl | cells/μl | cells/μl | ||
| No 1 | 1130 | 789 | 414 | 354 | 155 | 0,8 | 177 |
| No 2 | 1354 | 1002 | 372 | 603 | 176 | 1,6 | 135 |
| No 3 | 1320-3570 | 690-2540 | 190-1140 | 410-1590 | 90-660 | 1,5-2,60 | 90-590 |
Note: cells/μl – cells per microliter, Ref. – reference
Based on the results and the individual treatment characteristics of each patient, it is appropriate to consider each case separately. Patient 1, who was in the preoperative stage and receiving dexamethasone, had lymphopenia (1130 cells/μl). The T-helper cell count in the peripheral blood was below the threshold level, and the CD4+/CD8+ ratio was below the reference values (354 cells/μl). In the second clinical case, the patient did not receive dexamethasone before neurosurgical treatment or at the time of blood sampling. The total number of lymphocytes in the peripheral blood was close to the lower threshold value (1354 cells/μl), and all subpopulation quantitative indicators were within the reference values. However, the CD4+/CD8+ ratio was at a lower threshold level due to the relatively low T-helper count (603 cells/μl). In addition to the standard IHC study, lymphocyte infiltration of the tumor and perifocal zone was assessed in two patients. The results are presented in Figures 1-3.
Case no 1
Histological examination of the surgical material from a 76-year-old patient (Fig. 1) confirmed IDH-wildtype glioblastoma: a highly malignant glial tumor GFAP+ with a diffuse growth pattern and high proliferative activity, with a nuclear labeling level of 15-18% using the Ki67/MIB1 marker. Anti-IDH1r132h antibody staining was negative. Perivascular and stromal lymphocytic infiltration was detected in the central and perifocal zones of the tumor, with a score of 2+.
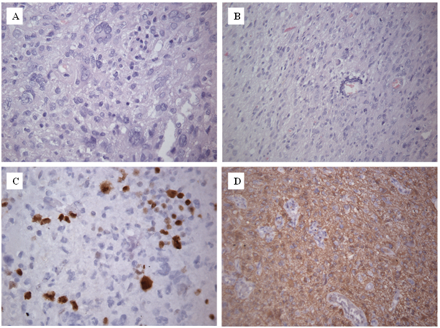
Figure 1: Results of histological examination of patient №1, 76 years old. H&E stain, A–×400, Б–×200; А: Malignant glial tumor with cellular polymorphism. Lymphocytic infiltration of the tumor stroma with a few lymphocytes, 2+; B: Perifocal zone of the tumor adjacent to unchanged brain tissue. Perivascular lymphocytic infiltration, 2+; C: Level of proliferative activity by Ki67 15–18%, ×400; D: Diffuse cytoplasmic staining with antibodies to GFAP, ×200
An immunohistochemistry (IHC) study was conducted on lymphocyte differentiation clusters in patient No. 1. The results showed that the CD45 marker-stained numerous stromal lymphocytes in the center of the tumor (Fig. 2A), as well as perivascular lymphocytes in the perifocal zone (Fig. 2B). Additionally, microglia were found to be activated in all areas of the tumor (Fig. 2C). The average number of lymphocytes in 1 mm2 of tissue was 20.73.8 cells. However, no staining of lymphocytes with the CD20 marker was observed. Further analysis revealed positive staining of tumor tissue lymphocytes with the CD3 marker, which colocalized with CD45 staining (Fig. 2 D-E). It should be noted that the CD3 marker did not stain microglia. The average number of CD3+ lymphocytes in 1 mm2 of tumor center tissue was 20.73.8 cells, while in the perifocal zone it was 25.24.4 cells. Staining with the CD4 marker (Fig. 2 F-G) showed that some lymphocytes were stained, and these cells were also colocalized with CD3+ cells. Interestingly, microglial staining with the CD4 marker was also detected, with an increase in the perifocal zone of the tumor. The average number of CD4+ lymphocytes in 1 mm2 of tumor center tissue was 7.73 cells, which accounted for 37.2% of the total T-lymphocyte pool. In the perifocal parts of the tumor, the average number of CD4+ lymphocytes in 1 mm2 of tissue was 8.31.8 cells, accounting for 32.9% of the total pool of T-lymphocytes. Similarly, staining with the CD8 marker (Fig. 2 H-I) showed that some lymphocytes were stained and colocalized with CD3+ cells. The average number of CD8+ lymphocytes in 1 mm2 of tumor center tissue was 183.2 cells, which accounted for 86.9% of the total T-lymphocyte pool. In the perifocal zone of the tumor, the average number of CD8+ lymphocytes in 1 mm2 of tissue was 10.22.6 cells, accounting for 40.5% of the total pool of T-lymphocytes.
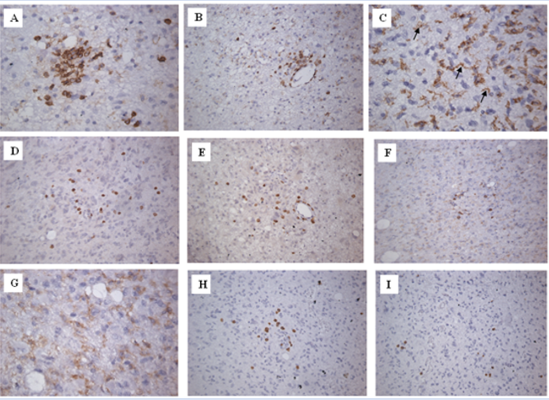
Figure 2: Results of IHC typing of lymphocytes of the patient no 1. А: IHC by antibodies to CD45 in the central part of the tumor, ×400; B: IHC by antibodies to CD45 in the perifocal parts of the tumor, ×200; C: IHC by antibodies to CD45 in the central part of the tumor, microglia staining is indicated by an arrow, ×400; D: IHC by antibodies to CD3 in the central part of the tumor, ×200; E: IHC by antibodies to CD3 in the perifocal parts of the tumor, ×200; F: IHC by antibodies to CD4 in the central part of the tumor, ×200; G: IHC by antibodies to CD4 in the perifocal parts of the tumor, ×400; H: IHC by antibodies to CD8 in the central part of the tumor, ×200; I: IHC by antibodies to CD8 in the perifocal parts of the tumor, ×200
Case no 2
Histological examination of biopsy material from patient № 2, a 63-year-old, confirmed the presence of glioblastoma. The tumor stroma showed diffuse lymphocytic infiltration, with an average of 43.86.2 cells per 1 mm2 of tissue (Fig. 3). The lymphocytes observed ranged from lymphoblasts to mature cells, with some plasmacytes also present.
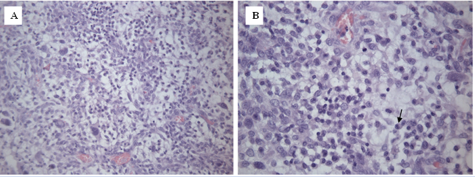
Figure 3: Results of histological examination of patient № 2, 63 years old. H&E stain, A –×200, B–×400. А: Abundant lymphocytic infiltration of the tumor stroma, 3+, B: Numerous lymphocytes of varying degrees of maturity, single plasmacytes indicated by an arrow, 3+.
This patient had a higher number of lymphocytes in both the peripheral blood and tumor tissue compared to patient no1. Patient no 3 had a higher number of lymphocytes in the peripheral blood compared to patients no 1 and no 2, but no tumor tissue was obtained.
Discussion
The role and function of lymphocyte subpopulations in immune control have been previously described in various oncological pathologies, such as leukemia, gastric cancer, colorectal malignancies, and lung cancer [24-27]. T-lymphocytes, specifically T-helper cells (CD3+CD4+/CD45+) and T-cytotoxic cells (CD3+CD8+/CD45+), play a crucial role in immune control [1-3, 23]. T-helper cells stimulate the adaptive immune response by interacting with dendritic cells carrying information about tumor antigens. Through the release of cytokines and direct contact, they activate effector cells of the immune system. T-cytotoxic lymphocytes target malignant cells and are responsible for their destruction [28].
The study of the immune status of patients with malignant gliomas of the central nervous system, particularly glioblastoma, is highly relevant. In 1977, it was first reported that patients with intracerebral astrocytomas had low levels of T lymphocytes in their blood [29]. Subsequent studies have confirmed T-lymphocyte dysfunction in patients with glioblastomas [30-32], with 42% of cases showing this immune system state at diagnosis, unrelated to specific antitumor treatment [32]. These studies defined lymphopenia as a T-lymphocyte count below 1500 cells/μl. Additionally, it was found that the decrease in T lymphocytes is primarily due to a decrease in T helper cells. In our study, patient No. 1, who is undergoing surgical treatment, had a total lymphocyte count below the threshold (1130 cells/μl), mainly due to a low level of T-helper cells (354 cells/μl). In the second clinical case, before specific antitumor therapy, the total T-lymphocyte count was 1354 cells/μl, which is below the borderline norm according to the study. It has been suggested that T cells may be sequestered in the bone marrow in intracerebral neoplasms [33]. One study found that patients with glioblastomas who did not receive specific antitumor treatment had a significant number of T cells, including T helper cells and T cytotoxic lymphocytes, in their bone marrow aspirates compared to their blood count. In contrast, the healthy control group had similar levels of T-lymphocytes in both blood and bone marrow. The mechanism behind the isolation of immune system cells in the bone marrow is linked to a decrease in the expression of the S1P1 protein (sphingosine-1-phosphate receptor 1) on the surface of T lymphocytes. However, the reason why only intracranial tumors cause this defect in immune system functioning and the mechanism behind it are still unknown.
Today, there is ongoing debate in the scientific medical community regarding the impact of glucocorticosteroids on systemic immunity. While some studies have not found a connection between lymphopenia and the use of dexamethasone [6,32], others have reported a correlation [34, 35]. It is important to note that patient № 1 received symptomatic therapy with dexamethasone, unlike patient № 2, and in the first case, the level of T-lymphocytes was lower. Additionally, the infiltration of tumor T-lymphocytes in the histological material was significantly lower in the first patient compared to the second clinical case, where dexamethasone was not prescribed. Studies have shown that naive T cell are the most sensitive subpopulation to glucocorticosteroids. The administration of dexamethasone led to an increase in CTLA-4 (cytotoxic T-lymphocyte-associated protein-4) on the surface of these cells, which blocked the cell cycle and differentiation [35].
Systemic lymphopenia also affects the local immune response. As demonstrated in clinical case № 1, the infiltration of glioblastoma by T lymphocytes is very weak. In addition to the systemic decrease in lymphocytes, there are other known mechanisms by which glioblastoma evades immune control. Once in the tumor microenvironment, the few effector T cells encounter an immunosuppressive environment created by glioblastoma [6]. Tumor cells and tumor-associated macrophages express proteins that inhibit the functioning of effector cells of the immune system, while myeloid cells attracted by glioblastoma produce enzymes that break down nutrients for T lymphocytes. As a result, the T lymphocytes infiltrating glioblastoma represent a small population of exhausted immune cells. It was also shown that pre-chemotherapy Systemic Inflammatory Index < 480>
Thanks to recent studies, our understanding of the immune status of patients with glioblastomas has significantly expanded. One of the main challenges in achieving an effective immune response is systemic lymphopenia. However, the development of treatment methods such as CAR T-therapy (chimeric antigen receptor T-lymphocyte therapy) may offer a promising solution to this issue. Additionally, the impact of glucocorticosteroids on lymphocytes should be considered. Some experts suggest replacing these drugs with bevacizumab to achieve an anti-edematous effect [37-38]. Furthermore, the unique features of local immune surveillance in glioblastoma must be considered. Given the various mechanisms of local immunosuppression in this tumor, it is advisable to develop different combinations of immunotherapy to increase the number of T cells and activate them. When considering the use of checkpoint inhibitors, it is important to analyze the lymphocytic infiltration of the tumor stroma in each individual patient.
Conclusion
With the results of fundamental research from the past decade, we can expect numerous preclinical and clinical studies soon to develop new immunotherapeutic approaches for the treatment of glioblastoma, the most malignant and common tumor of the central nervous system. These advancements have the potential to greatly improve the prognosis for our patients.
Declarations
Conflict of interest
The author declares no conflict of interest.
Funding
The study was performed without external funding.
Compliance with patient rights and principles of bioethics. All patients gave written informed consent to participate in the study.
References
- Abbot M, Ustoyev Y. (2019). Cancer and the Immune System: The History and Background of Immunotherapy. Semin Oncol Nurs, 35(5):150923.
Publisher | Google Scholor - Blair G.E, Cook G.P. (2008). Cancer and the immune system: an overview. Oncogene, 27(45):5868.
Publisher | Google Scholor - Dunn G.P, Old L.J, Schreiber R.D. (2004). The three Es of cancer immunoediting. Annu Rev Immunol, 22:329-60.
Publisher | Google Scholor - Chen D.S, Mellman I. (2013). Oncology meets immunology: the cancer-immunity cycle. Immunity, 39(1):1-10.
Publisher | Google Scholor - Topalian S, Hodi F.S, Brahmer J.R, Gettinger S.N, Smith D.C, McDermott D.F, Powderly J.D, Carvajal R.D, Sosman J.A, Atkins M.B, Leming P.D, Spigel D.R, Antonia S.J, Horn L, Drake C.G, Pardoll D.M, Chen L, Sharfman W.H, Anders R.A, Taube J.M, McMiller T.L, Xu H, Korman A.J, Jure-Kunkel M, Sznol M. (2012). Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med, 366(26):2443-2454.
Publisher | Google Scholor - Sklyar S.S, Trashkov A.P, Matsko M.V, Safarov B.I, Vasiliev A.G. (2022). Immune response to primary glioblastoma. Pediatrician, 13(2):49-60.
Publisher | Google Scholor - Aspelund A, Antila S, Proulx S.T, Karlsen T.V, Karaman S, Detmar M, Wiig H, Alitalo K. (2015). A dural lymphatic vascular system that drains brain interstitial fluid and macromolecules. J. Exp. Med, 212:991-999.
Publisher | Google Scholor - Louveau A, Smirnov I, Keyes T.J, Eccles J.D, Rouhani S.J, Peske J.D, Derecki N.C, Castle D, Mandell J.W, Lee K.S. (2015). Structural and functional features of central nervous system lymphatic vessels. Nature, 523:337-341.
Publisher | Google Scholor - Majc B, Novak M, Kopitar-Jerala N, Jewett A, Breznik B. (2021). Immunotherapy of Glioblastoma: Current Strategies and Challenges in Tumor Model Development. Cells, 10(265):2-22.
Publisher | Google Scholor - Kondratyev A.N, Tsentsiper L.M. (2019). Glymphatic system of the brain: structure and practical significance. Russian Journal of Anaesthesiology and Reanimatology. Anesteziologiya i Reanimatologiya, 6:72-80.
Publisher | Google Scholor - Filley A.C, Henriquez M, Dey M. (2017). Recurrent glioma clinical trial, checkmate- 143: the game is not over yet. Oncotarget, 8(53):91779-91794.
Publisher | Google Scholor - Omuro A, Vlahovic G, Lim M, Sahebjam S, Baehring J, Cloughesy T. (2018). Nivolumab with or without ipilimumab in patients with recurrent glioblastoma: results from exploratory phase 1 cohorts of checkmate 143. Neuro-Oncology, 20(5):674-686.
Publisher | Google Scholor - Brat D.J, Ellison D.W, Figarella-Branger D, Hawkins C.E, Louis D.N. et al. (2021). WHO Classification of Tumours Editorial Board. Central nervous system tumours. Lyon (France): International Agency for Research on Cancer. WHO Classification of Tumours Series, 5th ed, 2.
Publisher | Google Scholor - Ostom Q.T, Price M, Neff C, Cioffi G, Waite K.A, Kruchko C, Barnholtz-Sloan J.S. (2022). CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015-2019. Neuro Oncol, 24:1-95.
Publisher | Google Scholor - Matsko M.V, Sklyar S.S, Ulitin A.Yu, Matsko D.E, Imyanitov E.N, Ievleva A.G, Ni V.I, Volkov N.M, Zrelov A.A, Baksheeva A.O, Galkina D.V. (2021). Changes in the MGMT gene expression in patients with primary glioblastoma after relapse. Influence of clinical characteristics and MGMT expression on survival of patients. Siberian Journal of Oncology, 20(3):5-17.
Publisher | Google Scholor - Nechaeva A.S, Kukanov K.K. (2023). Achievements and prospects in dendritic cell vaccine therapy in patients with malignant glial tumors. Russian Journal for Personalized Medicine, 3(3):79-90.
Publisher | Google Scholor - Nazaralieva E.T, Fedorov V.S, Zabrodskaya Yu.M, Kim A.V, Djanaliev B.R, Shevtsov M.A, Samochernych K.A. (2022). Heat shock proteins as diagnostic and prognostic markers in malignant tumors of the central nervous system. Translational Medicine, 9(6):5-15.
Publisher | Google Scholor - Jackson C.M, Choi J, Lim M. (2019). Mechanisms of immunotherapy resistance: lessons from glioblastoma. Nature Immunology, 20(9):1100-1109.
Publisher | Google Scholor - Berghoff A.S, Kiesel B, Widhalm G, Rajky O, Ricken G, Wohrer A. (2015). Programmed death ligand 1 expression and tumor-infiltrating lymphocytes in glioblastoma. Neuro-Oncology, 17:1064-1075.
Publisher | Google Scholor - Nduom E.K, Wei J, Yaghi N.K, Huang N, Kong L.Y, Gabrusiewicz K. (2016). PD-L1 expression and prognostic impact in glioblastoma. Neuro-Oncology, 18(2):195-205.
Publisher | Google Scholor - Laviron M, Boissonnas A. (2019). Ontogeny of Tumor-Associated macrophages. Frontiers in Immunology. Front Immunol, 31(10):1799.
Publisher | Google Scholor - Majc B, Novak M, Kopitar-Jerala N, Jewett A, Breznik B. (2021). Immunotherapy of Glioblastoma: Current Strategies and Challenges in Tumor Model Development. Cells, 10(265):2-22.
Publisher | Google Scholor - Li F, Li C, Cai X, Xie Z, Zhou L, Chaeng B, Zhong R, Xiong S, Li J, Chen Z, Yu Z, He J, Liang W. (2021). The association between CD8+ tumor-infiltrating lymphocytes and the clinical outcome of cancer immunotherapy: A systematic review and meta-analysis. E Clinical Medicine, 41:101134.
Publisher | Google Scholor - Chetveryakov A.V, Tereshkov P.P, Tsepelev V.L, Kryukova V.V. (2023). Cytotoxic T-lymphocyte subpopulations content in patients with colon tumor. Modern Problems of Science and Education, 3.
Publisher | Google Scholor - Jin K, Cao Y, Gu Y. (2021). Poor clinical outcomes and immunoevasive contexture in CXCL13+CD8+ T-cells enriched gastric cancer patients. Onco immunology, 10 (1):1915560.
Publisher | Google Scholor - Radpour R, Riether C, Simillion C. (2019). CD8+ T cells expand stem and progenitor cells in favorable but not adverse risk acute myeloid leukemia. Leukemia, 33(10):2379-2392.
Publisher | Google Scholor - Wang W.J. (2013). Variation of blood T lymphocyte subgroups in patients with non-small cell lung cancer. Asian Pacific journal of cancer prevention, 14(8):4671-4673.
Publisher | Google Scholor - Semiglazov V.F, Tseluiko A.I, Baldueva I.A, Nekhaeva T.L, Artemyeva A.S, Kudaybergenova A.G, Protsenko S.A, Novik A.V, Semiglazov V.V, Donskikh R.V, Semiglazova T.Yu, Pesotskiy R.S, Apollonova V.S, Krivorotko P.V, Belyaev A.M. (2021). Immunology and immunotherapy in the complex treatment of malignant tumors. Meditsinskiy sovet. Medical Council, 4:248-257.
Publisher | Google Scholor - Mahaley M.S. Jr, Brooks W.H, Roszman T.L. (1977). Immunobiology of primary intracranial tumors. Part 1: studies of the cellular and humoral general immune competence of brain-tumor patients. J Neurosurg, 46:467-476.
Publisher | Google Scholor - Dix A.R, Brooks W.H, Roszman T.L. (1999). Immune defects observed in patients with primary malignant brain tumors. J Neuroimmunol, 100:216-232.
Publisher | Google Scholor - Woroniecka K.I, Rhodin K.E, Chongsathidkiet P. (2018). T-cell dysfunction in Glioblastoma: applying a new framework. Clin Cancer Res, 24(16):3792-3802.
Publisher | Google Scholor - Kim W.J, Dho Y, Ock C, Kim J.W, Choi S.H, Lee S, Kim I.H, Kim T.M, Park C.K. (2019). Clinical observation of lymphopenia in patients with newly diagnosed glioblastoma. J Neurooncol, 143(2):321-328.
Publisher | Google Scholor - Chongsathidkiet P, Jackson C, Koyama S, Loebel F, Cui X, Farber S.H, Woroniecka K, Elsamadicy A, Dechant C.A, Kemery H.R, Sanchez-Perez L, Cheema T.A. (2018). Sequestration of T cells in bone marrow in the setting of glioblastoma and other intracranial tumors. Nat Med, 24(9):1459-1468.
Publisher | Google Scholor - Iorgulescu J.B, Gokhale P.C, Speranza M.C, Eschle B.K, Poitras M.J, Wilkens M.K, Soroko K.M. (2021). Concurrent Dexamethasone Limits the Clinical Benefit of Immune Checkpoint Blockade in Glioblastoma. Clin Cancer Res, 27(1):276-287.
Publisher | Google Scholor - Giles A, Hutchinson M.N.D, Sonnemann H.M, Jung J, Fecci P.E. (2018). Dexamethasone-induced immunosuppression: mechanisms and implications for immunotherapy. J Immunother Cancer, 6(1):51.
Publisher | Google Scholor - Gurrieri L, Mercatali L, Ibrahim T. et al. (2023). Immuno markers in newly diagnosed glioblastoma patients underwent Stupp protocol after neurosurgery: a retrospective series. J Neurooncol, 164:55-64.
Publisher | Google Scholor - Yu M.W, Quail D.F. (2021). Immunotherapy for Glioblastoma: Current Progress and Challenges. Front Immunol, 12:676301.
Publisher | Google Scholor - Morgacheva D.A, Sitovskaia D.A, Dinikina Yu.V. (2023). Diagnostic and therapeutical approaches to H3K27M-altered diffuse midline glioma in children: a review. Oncohematology, 18(4):104-114.
Publisher | Google Scholor










