

Case Report
Immediate And Long-Term Effects of Vibration-Based Physical Therapy for Stiff Person Syndrome: A Case Report
- Chiemi Kobayashi *
Japan Physical Therapy Association Home-based membership, Hananokidai Narita Chiba Japan.
*Corresponding Author: Chiemi Kobayashi PhD* Japan Physical Therapy Association Home-based membership, Hananokidai Narita Chiba Japan.
Citation: Chiemi Kobayashi. (2024). Immediate And Long-Term Effects of Vibration-Based Physical Therapy for Stiff Person Syndrome: A Case Report, International Clinical Case Reports and Reviews, BioRes Scientia Publishers. 2(3):1-9. DOI: 10.59657/2993-0855.brs.24.022
Copyright: © 2024 Chiemi Kobayashi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 14, 2024 | Accepted: October 31, 2024 | Published: November 04, 2024
Abstract
Aim: Stiff person syndrome (SPS) presents with muscle spasms and stiffness. Herein, we present the effects of vibration-based therapy in a patient with SPS.
Methods: A female patient in her late 50s was followed up for 21 months while undergoing vibration-based therapy targeting the posterior thigh and lumbar region. Outcome measures included the anterior body bending distance in a sitting position and finger floor distance (FFD). Motor function was assessed thrice using the Short Physical Performance Battery (SPPB). A paired t-test was performed to assess immediate effects, and long-term effects were compared at the beginning and at the end.
Results: Body forward bending distance and immediate FFD results significantly improved from baseline. The long-term effect also clearly improved. The SPPB improved from 2 points at baseline to a perfect score at the final follow-up.
Conclusion: Vibration-based therapy can be used to treat patients with SPS.
Keywords: autoimmune disease; body forward bending distance; finger floor distance; home rehabilitation; muscle rigidity; short physical performance battery
Introduction
Stiff person syndrome (SPS) is an extremely rare, chronic, progressive autoimmune neurological disorder, which gained notoriety after Ms. Celine Dion, an internationally acclaimed vocalist, publicly admitted her diagnosis. A survey-based study in Japanese hospitals revealed 257 SPS cases between January 2015 and December 2017 [1]. However, as the disease is rare and remains poorly understood by physicians, the number of affected patients is likely higher. High-titre anti-glutamate decarboxylase (GAD) antibody is a rate-limiting enzyme in the synthesis pathway of the inhibitory neurotransmitter γ-aminobutyric acid (GABA). Its mechanism of action, pathway, and effect on the intracellular compartment are unknown [2]. GAD and glycine receptor (GlyR) are distributed in the brainstem, spinal cord, olfactory bulb, hippocampus, cerebellum, and retina on the caudal side. Moreover, gephyrin is a scaffold protein in the inhibitory postsynaptic membrane and is involved in the synaptic localization of GlyR and some GABAA receptors. It has been suggested that the presence of these antibodies affects GABA production at the site and inhibits the action of inhibitory synapses, causing motor neurons such as α and γ neurons to become overexcited and cause muscle stiffness [3]. Although SPS is considered an autoimmune neurological disease, some patients present with negative antibody tests. The major diagnostic criteria for SPS (all criteria should be present) are as follows: (1) An insidious onset of muscular rigidity affecting the limbs and axial muscles, particularly notable in the abdominal and thoracolumbar paraspinals, accompanied by difficulties in turning or bending; (2) painful spasms that are triggered by unexpected noises, tactile stimuli, or emotional disturbances; (3) persistent motor unit activity in both agonist and antagonist muscles, as confirmed clinically; and (4) normal motor and sensory tests, except for challenges in active movements. The minor criteria include (1) the presence of anti-GAD65 antibodies (or other autoantibodies) in the serum, as determined by techniques such as immunocytochemistry, western blot, enzyme linked immunosorbent assay, enzyme immunoassay, or radioimmunoassay; (2) electromyographic evidence of continuous motor unit activity in both agonist and antagonist muscles; and (3) clinical response to benzodiazepines or sleep (symptom improvement) [1]. Meanwhile, progressive lower limb rigidity increases the risk of falls [1]. Previous studies have reported the pharmacological treatments for SPS, but only one report (n=9) published in English has documented the effects of physiotherapy for this indication [4]. Additionally, a few rehabilitation case studies have clearly reported on the use of drug treatments, types of interventions used, and endpoints examined [5,6]. Among physiotherapy-based modalities, only orthotic therapy has shown marked improvement [7], wherein the patient had used a short plastic brace during the day and at night, showing an ability to stand and walk without the use of assistive devices after 2 days of intervention [7]. The Kawahira method may improve and inhibit spasticity and stiffness by implementing vibrational stimulation [8]. In patients with stroke, vibration-based therapy delivered to the spastic muscles for more than 5 min has been shown to help reduce spasticity and excitability of spinal motor neurons in the F-wave [9]. In addition, as 10-min vibration stimulation caused a decrease in the H/M wave ratio in healthy individuals [10]. Suppression of the presynaptic spinal cord from fibres I and II is thought to suppress α and γ motor neuron activities. Herein, we present the immediate and long-term effects of vibration-based therapy on the body bending distance in a sitting position, finger floor distance (FFD) in a standing position, and the effect of the Short Physical Performance Battery (SPPB).
Case Report
This is a retrospective case report. According to the information from this case, in 2012, a woman in her late 40s (late 50s at the time of manuscript writing) developed spasms of the myoclonus of the tongue and the hypothenar muscles and was referred to the Department of Neurology at N Hospital by the Department of Orthopaedics at T Hospital. In the 4th year and 7th month, she received a definitive diagnosis from the Department of Neurology at C hospital. Initially, the patient was treated symptomatically with anticonvulsants (tizanidine hydrochloride 3 mg/day) and antiepileptics (aleviatin 50 mg/day and sodium valproate tablets 200 mg/day).
She had asthma from adolescence until her late twenties. Her biological mother was on dialysis due to IgA nephropathy. From the left upper limb, the cramps and stiffness gradually progressed to the lower limb and the right upper limb, necessitating the use of a cane or electric wheelchair outdoors.
Clinical Findings
Her tendon reflexes were increased in both the upper and lower limbs, and her pathological reflexes (Hoffman) were positive, while all antibody tests (anti-NMDAR antibody, anti-LGI1 antibody, anti-CASPR2 antibody, anti-GABABR antibody, anti-DPPX antibody, anti-GlyR antibody, and anti-GABAAR antibody) were serum- and intrathecal-negative. In response to diazepam, she showed improvement in painful spasms and rigid seizures during sleep. The main clinical findings were painful limb cramps and decreased mobility due to stiffness in both the lower limbs and torso. These were exacerbated by voluntary movements, cold stimuli, and agoraphobia.
Timeline
SPS is associated with diurnal and seasonal fluctuations and may be triggered by various external stimuli (such as touch, sound, emotion, and cold). The patient experienced symptom exacerbation after activity. She was prone to muscle spasms and muscle stiffness, making it difficult for her to walk. Symptom flare-ups were treated with steroid pulse therapy, which overtime resulted in steroid diabetes, cataracts, and bilateral femoral head necrosis, leading to dose reduction. Immunotherapy was initiated, and immunoglobulin therapy was administered once every 4–5 weeks. In August 2018, she obtained physical disability certificate grade 3 and walked outdoors while leaning on an electric wheelchair and a carry case. In February 2019, she resigned from her job due to home oxygen use prescribed to manage acute respiratory failure. Prior to losing her job, she had held the position of administrator of a rehabilitation department. In April 2019, she received disability certificate grade 1 (grade 3 for both lower limbs, grade 6 for both upper limbs, and grade 1 for respiratory dysfunction were merged) and disability pension grade 2. She received help with household chores such as shopping and cleaning three times a week. She struggled to cut her nails and wear socks. She was able to walk slowly and freely indoors but could not carry cargo and used a wagon with casters. As the stiffness in her lower legs progressed, she found it difficult to walk outdoors and developed agoraphobia, which forced her to use an electric wheelchair.
Method
The patient was treated at home twice a week by the same physiotherapist. Between August 4, 2020 and April 28, 2022, vibration-based therapy was performed at 87 Hz (5,200/min) on the back of the thighs and lumbar dorsal muscles using a commercially available hand massager (THRIVE Handy Massager MD-001; Daito Electric Industry Co., Ltd.), which was applied softly over clothes, and the stiff muscles were stretched by cross massage (Video 1). Before and after physical therapy, the body was bent forward in a sitting position, and the forward bending distance was measured, as recommended by the guidelines [11] (Figure 1). In addition, FFD, usually performed at 40 cm, was evaluated on a 20-cm platform due to patient’s stiffness and concerns (Figure 2). FFD measurements in a standing position are not usually performed but were used in this case to evaluate activities of daily living, such as picking up objects. Immediate results were compared with those before the intervention using paired t-tests. The significance level was set at p less than 0.05. Long-term effects were compared based on maximum values obtained at baseline and end of follow-up. To assess motor performance, including balance function, SPPB (Table 1) was measured three times. The patient was asked if she felt comfortable or uncomfortable during treatment and evaluation. To suppress stiff and spastic muscles, vibration-based therapy was applied to the lightly rigid muscle abdomen (muscle spindle: Ia, II fibres) on the clothes for 60 s, but because it was too suppressed and the knee was unstable in the standing position, the time was gradually shortened, and the final stimulation time was determined while watching the stability of the knee.
Table 1: Short Physical Performance Battery (SPPB) Evaluation Form
| I Standing balance test (no walking aids allowed) | |||
| ( sec ) | ≥10 sec:1p□ | |
| less than 10 sec:0p□ | |||
| Impossible: 0p□ | |||
| 2. Hold semi-tandem standing position for 10 seconds *Touch one big toe and one heel | ( sec ) | ≥10 sec:1p□ | |
| less than 10 sec:0p□ | |||
| Impossible: 0p□ | |||
| 3. Hold tandem standing position for 10 seconds *Hold the position with the heel of one foot touching the toe of the other foot for 10 seconds | ( sec ) | ≥10 sec:2p□ | |
| 3-9.99 sec: 1p□ | |||
| less than 3 sec: 0p□ | |||
| Impossible: 0p□ | |||
| II Walking test | |||
| Walk 4 m at normal speed and measure the time twice | less than 4.82 sec:4p□ | ||
| *Subject aligns feet at starting line | 4.82-6.20 sec: 3p□ | ||
| *Measure the time when the subject starts walking the signal | 6.21-8.70 sec:2p□ | ||
| *Measurement stops when one foot crosses the goal | ≥8.70 sec:1p□ | ||
| *Do not stop at the goal and cross the line | Impossible: 0p□ | ||
| 1st time | 2nd time | With/without assistive devices | |
| ( sec ) | ( sec ) | ( ) | |
| Ⅲ. Chair standing test | |||
| *Pre-test: Stand up from the chair with your arms crossed in front of your chest. *Actual: Measure the time to quickly stand up/sit down 5 times | less than 11.19 sec:4p□ | ||
| 11.20-13.69 sec: 3p□ | |||
| 13.7-16.69 sec: 2p□ | |||
| ( sec ) | ≥60 sec・impossible:0p□ | ||
| Total score | |||
| Ⅰ. Balance test | ( ) Point | ||
| Ⅱ. Walking test | ( ) Point | ||
| Ⅲ. Start-up test | ( ) Point | ||
| Total score | ( ) point | ||
Figure 1: Anterior body bending distance in a sitting position. The distance travelled is indicated with the arrow.
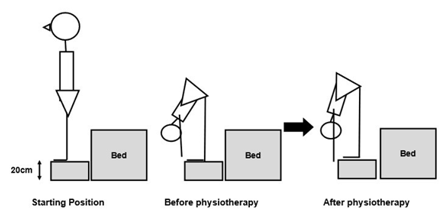
Figure 2: Finger floor distance.
Results
A sufficient stretching effect was observed with 30 s of vibration-based therapy (Video 1), and stability in a standing position was ensured. The mean (± SD) body forward bending distance before and after the intervention was 14.48 (±9.06) and 15.28 (±9.39), respectively (t = -3.77, p = 0.00023). The corresponding FFD values were 4.82 (±4.04) and 6.81 (±3.10), respectively (t = -10.91, p less than 0.001). The perceived stiffness improved, and the patient reported feeling more relaxed. Over time, the forward bend distance improved from -8.5 cm to +27.0 cm. The corresponding change to the FFD was from -12.5 cm to +12.0 cm (Appendix) Video.
Video : Vibration-based therapy to the muscle spindle on the posterior surface of the thigh.
Apply stimulation to the hamstrings for about 30 seconds so that the knee progresses from the hip flexion position.
Appendix: Case Progress Data
| Finger Floor Distance | On the forward bend distance of the body in the long sitting position | |||
| Before | After | Before | After | |
| 2020/8/4 | -12.5 | -7.0 | -8.5 | -6.5 |
| 2020/8/6 | -7.5 | 7.0 | -3.0 | 0.5 |
| 2020/8/11 | -5.0 | -2.5 | -7.0 | -2.5 |
| 2020/8/13 | -6.0 | 3.0 | -3.5 | -1.0 |
| 2020/8/18 | 0.0 | -2.0 | -4.5 | -3.5 |
| 2020/8/20 | 0.0 | 2.5 | -2.5 | -4.0 |
| 2020/8/27 | 3.5 | 7.0 | 1.0 | 0.0 |
| 2020/9/1 | -8.0 | -9.0 | -6.0 | -0.5 |
| 2020/9/3 | 5.0 | 6.0 | 2.5 | 0.0 |
| 2020/9/8 | 3.0 | 5.5 | 0.5 | 1.0 |
| 2020/9/10 | 4.0 | 7.0 | 1.5 | 1.5 |
| 2020/9/15 | 1.5 | 5.0 | 0.5 | 0.5 |
| 2020/9/17 | 5.0 | 6.0 | 3.5 | 2.5 |
| 2020/10/1 | 2.5 | 6.5 | 2.0 | 2.5 |
| 2020/10/6 | -10.0 | 0.0 | -1.5 | -2.5 |
| 2020/10/8 | 3.0 | 4.5 | 3.5 | 3.0 |
| 2020/10/13 | 3.5 | 4.5 | 3.0 | 3.0 |
| 2020/10/15 | 2.5 | 3.0 | 6.0 | 3.5 |
| 2020/10/20 | -8.5 | -1.5 | -1.5 | 0.0 |
| 2020/10/22 | 0.0 | 0.5 | 3.0 | -0.5 |
| 2020/10/27 | -12.5 | -3.5 | -3.5 | -2.0 |
| 2020/10/29 | 2.5 | 4.0 | 4.5 | 5.0 |
| 2020/11/5 | 1.5 | 4.5 | 4.0 | 4.0 |
| 2020/11/9 | -8.0 | 2.5 | 2.0 | 2.0 |
| 2020/11/12 | 4.5 | 7.0 | 5.5 | 6.0 |
| 2020/11/16 | 3.5 | 6.0 | 6.5 | 6.5 |
| 2020/11/19 | 4.0 | 5.5 | 6.0 | 6.0 |
| 2020/11/26 | 6.0 | 7.0 | 7.5 | 6.0 |
| 2020/11/30 | 2.5 | 5.5 | 5.0 | 5.0 |
| 2020/12/3 | 2.0 | 5.5 | 7.0 | 4.0 |
| 2020/12/10 | 2.0 | 4.0 | 7.0 | 8.0 |
| 2020/12/14 | 5.0 | 6.0 | 5.5 | 8.0 |
| 2020/12/17 | 3.5 | 3.5 | 4.0 | 4.0 |
| 2020/12/21 | 6.0 | 7.0 | 6.5 | 6.5 |
| 2020/12/24 | 6.5 | 5.5 | 8.5 | 9.0 |
| 2020/12/28 | 6.0 | 7.5 | 7.5 | 6.5 |
| 2020/12/29 | NI | NI | NI | NI |
| 2020/12/30 | NI | NI | NI | NI |
| 2020/12/31 | NI | NI | NI | NI |
| 2021/1/14 | 2.5 | 4 | 5.0 | 6.0 |
| 2021/1/18 | 5.5 | 5.5 | 6.0 | 6.5 |
| 2021/1/21 | 6.0 | 6 | 8.5 | 5.5 |
| 2021/1/25 | 4.0 | 5.5 | 6.0 | 6.5 |
| 2021/1/28 | 5.5 | 6.5 | 8.5 | 9.0 |
| 2021/2/8 | 6.5 | 5.5 | 7.0 | 6.5 |
| 2021/2/11 | 6.0 | 8.5 | 7.0 | 10.0 |
| 2021/2/15 | 6.0 | 7.5 | 7.5 | 7.5 |
| 2021/2/18 | 5.0 | 6.5 | 12.0 | 12.0 |
| 2021/2/25 | 4.0 | 6.0 | 10.0 | 10.0 |
| 2021/3/1 | 2.0 | 4.0 | 12.0 | 10.0 |
| 2021/3/4 | 6.0 | 7.0 | 9.5 | 10.0 |
| 2021/3/8 | 6.0 | 7.5 | 12.0 | 10.0 |
| 2021/3/11 | 7.0 | 9.5 | 10.0 | 10.5 |
| 2021/3/15 | 7.0 | 8.0 | 11.5 | 12.0 |
| 2021/3/18 | 3.5 | 8.0 | 9.0 | 10.5 |
| 2021/3/22 | 6.0 | 7.5 | 10.0 | 11.0 |
| 2021/3/25 | 6.0 | 6.5 | 9.0 | 10.0 |
| 2021/3/29 | 10.5 | 10.0 | 12.5 | 11.5 |
| 2021/4/1 | 9.0 | 6.5 | 11.0 | 10.0 |
| 2021/4/5 | 7.5 | 9.0 | 11.5 | 12.0 |
| 2021/4/8 | 6.5 | 9.0 | 9.5 | 11.5 |
| 2021/4/12 | 7.0 | 8.0 | 9.5 | 9.5 |
| 2021/4/15 | 8.5 | 8.5 | 9.5 | 9.5 |
| 2021/4/19 | 9.5 | 10.5 | 10.0 | 11.5 |
| 2021/4/22 | 10.0 | 9.5 | 9.5 | 9.5 |
| 2021/4/26 | 9.5 | 8.5 | 11.5 | 11.5 |
| 2021/5/6 | 4.0 | 7.5 | 8.0 | 8.5 |
| 2021/5/10 | 7.5 | 8.5 | 9.0 | 9.5 |
| 2021/5/13 | 4.5 | 9.5 | 9.0 | 10.0 |
| 2021/5/17 | 6.0 | 6.5 | 8.0 | 9.0 |
| 2021/5/20 | 6.0 | 7.0 | 9.0 | 10.0 |
| 2021/5/24 | 7.0 | 8.5 | 9.5 | 11.0 |
| 2021/5/27 | 7.0 | 7.5 | 11.0 | 11.0 |
| 2021/5/31 | 5.0 | 6.5 | 25.0 | 26.0 |
| 2021/6/3 | 10.0 | 10.0 | 21.0 | 29.0 |
| 2021/6/7 | 7.0 | 9.0 | 26.0 | 26.0 |
| 2021/6/10 | 5.0 | 5.5 | 22.5 | 26.0 |
| 2021/6/14 | 6.0 | 7.0 | 28.0 | 21.0 |
| 2021/6/17 | 6.0 | 8.0 | 22.0 | 21.5 |
| 2021/6/21 | 5.5 | 8.0 | 25.5 | 26.0 |
| 2021/6/24 | 6.0 | 8.0 | 22.0 | 21.0 |
| 2021/6/28 | 7.0 | 7.5 | 20.5 | 19.0 |
| 2021/7/1 | 5.5 | 8.0 | 21.5 | 22.5 |
| 2021/7/5 | 7.0 | 8.0 | 20.5 | 18.5 |
| 2021/7/8 | 2.0 | 5.0 | 21.5 | 20.5 |
| 2021/7/12 | 6.0 | 9.5 | 23.0 | 24.0 |
| 2021/7/15 | 7.5 | 11.0 | 21.5 | 23.5 |
| 2021/7/19 | 6.5 | 9.5 | 19.0 | 20.0 |
| 2021/7/25 | 4.0 | 10.5 | 16.5 | 24.5 |
| 2021/7/29 | 7.0 | 9.5 | 21.0 | 24.5 |
| 2021/8/2 | 7.0 | 8.0 | 19.5 | 21.0 |
| 2021/8/5 | 5.5 | 8.0 | 19.0 | 21.5 |
| 2021/8/12 | 4.0 | 6.0 | 18.5 | 21.5 |
| 2021/8/16 | 5.5 | 6.5 | 19.5 | 19.0 |
| 2021/8/19 | 4.0 | 6.0 | 19.0 | 20.5 |
| 2021/8/23 | 5.5 | 7.0 | 24.0 | 23.0 |
| 2021/8/26 | 6.0 | 7.0 | 19.0 | 22.0 |
| 2021/8/30 | 4.5 | 7.5 | 13.5 | 20.5 |
| 2021/9/2 | 4.0 | 5.0 | 17.5 | 24.0 |
| 2021/9/6 | 3.5 | 6.5 | 14.0 | 21.0 |
| 2021/9/9 | 8.0 | 9.0 | 20.0 | 23.5 |
| 2021/9/13 | 5.5 | 7.5 | 23.0 | 18.0 |
| 2021/9/16 | 6.5 | 7.0 | 23.0 | 19.5 |
| 2021/9/23 | NI | NI | NI | NI |
| 2021/9/27 | 4.5 | 10.5 | 23.5 | 23.5 |
| 2021/9/30 | 5.5 | 7.5 | 20.0 | 17.5 |
| 2021/10/4 | 7.5 | 10.0 | 22.0 | 23.5 |
| 2021/10/7 | 7.5 | 8.5 | 24.0 | 23.5 |
| 2021/10/11 | 8.0 | 10.0 | 18.5 | 19.0 |
| 2021/10/14 | 3.0 | 4.5 | 17.0 | 18.0 |
| 2021/10/18 | 3.0 | 7.0 | 22.0 | 23.0 |
| 2021/10/21 | 4.0 | 6.5 | 22.5 | 23.0 |
| 2021/10/25 | 7.0 | 8.0 | 16.5 | 20.5 |
| 2021/10/28 | 7.5 | 7.5 | 22.5 | 21.0 |
| 2021/11/1 | 7.5 | 8.5 | 24.0 | 23.5 |
| 2021/11/4 | 7.5 | 8.5 | 21.5 | 21.5 |
| 2021/11/8 | 7.0 | 9.0 | 21.0 | 25.0 |
| 2021/11/11 | 8.0 | 10.0 | 21.0 | 26.0 |
| 2021/11/15 | 10.0 | 10.5 | 27.0 | 25.5 |
| 2021/11/18 | 8.5 | 8.5 | 21.0 | 23.5 |
| 2021/11/22 | 8.0 | 9.0 | 22.5 | 23.0 |
| 2021/11/25 | 9.0 | 10.0 | 25.0 | 25.5 |
| 2021/11/29 | 6.5 | 8.0 | 22.5 | 23.0 |
| 2021/12/2 | 8.0 | 10.0 | 22.0 | 24.5 |
| 2021/12/6 | 9.0 | 9.5 | 25.0 | 21.0 |
| 2021/12/9 | 9.5 | 8.5 | 26.5 | 23.5 |
| 2021/12/13 | 10.0 | 11.5 | 24.5 | 25.0 |
| 2021/12/16 | 8.0 | 10.5 | 25.0 | 21.0 |
| 2021/12/28 | 8.5 | 10.5 | 22.5 | 25.0 |
| 2022/1/6 | 4.5 | 7.0 | 17.5 | 20.0 |
| 2022/1/3 | 7.5 | 8.5 | 21.0 | 21.5 |
| 2022/1/17 | 6.0 | 8.0 | 22.0 | 23.0 |
| 2022/1/20 | 7.0 | 7.5 | 20.0 | 21.5 |
| 2022/1/24 | 6.0 | 7.0 | 22.5 | 27.0 |
| 2022/1/27 | 3.0 | 7.0 | 22.0 | 24.0 |
| 2022/1/31 | 2.5 | 5.0 | 18.5 | 25.5 |
| 2022/2/3 | 7.0 | 7.5 | 21.5 | 23.0 |
| 2022/2/7 | 5.0 | 7.0 | 21.5 | 26.5 |
| 2022/2/10 | 5.5 | 9.0 | 21.0 | 27.0 |
| 2022/2/14 | 8.0 | 6.0 | 25.0 | 27.5 |
| 2022/2/17 | 6.0 | 6.0 | 24.5 | 23.0 |
| 2022/2/21 | 4.0 | 4.5 | 23.5 | 23.0 |
| 2022/2/24 | 8.0 | 10.5 | 23.5 | 24.0 |
| 2022/3/7 | 5.0 | 6.0 | 25.0 | 27.5 |
| 2022/3/10 | 5.0 | 2.0 | 26.0 | 19.0 |
| 2022/3/14 | 5.5 | 6.5 | 24.4 | 26.0 |
| 2022/3/18 | 4.0 | 5.5 | 24.0 | 24.0 |
| 2022/3/24 | 4.0 | 6.5 | 23.0 | 23.0 |
| 2022/3/28 | 8.0 | 7.5 | 23.0 | 26.0 |
| 2022/3/31 | 5.0 | 8.0 | 22.5 | 25.5 |
| 2022/4/4 | 8.0 | 9.0 | 23.0 | 23.5 |
| 2022/4/7 | 5.5 | 8.5 | 21.5 | 25.0 |
| 2022/4/11 | 5.5 | 7.5 | 22.0 | 27.0 |
| 2022/4/14 | 8.5 | 10.5 | 22.0 | 26.5 |
| 2022/4/18 | 7.5 | 12.0 | 25.5 | 25.5 |
| 2022/4/21 | 7.5 | 9.0 | 22.5 | 23.5 |
| 2022/4/25 | 7.5 | 9.0 | 25.5 | 19.0 |
| 2022/4/28 | 5.0 | 8.5 | 19.5 | 27.0 |
| MAX | 10.5 | 12.0 | 28.0 | 27.0 |
| MIN | -12.5 | -9.0 | -8.5 | -6.5 |
Initially, she had temporary abdominal muscle cramps during FFD, which gradually subsided and eventually stopped. The SPPB improved from 2 points at baseline to 11 points on 24 June 2021 and 12 points (perfect score) on 9 September 2021.
Discussion
Vibration-based therapy improved the short- and long-term assessments of muscle stiffness in this case. In a previous study of body bending distance in a sitting position in healthy individuals, the age/sex-matched mean (±SD) value was +41.78±8.99 cm [12], which was more than the final result in this case. However, herein, the SPPB improved and indoor mobility stabilized. A previous study [13] suggested that an SPPB score of 7 points was associated with the risk of falls in hospitalized patients. Another study [9] reported a decrease in spinal motor neuron excitability that occurred in the F-waves. In SPS, the straight leg raising stretching stimulation of the tendon receptors of the extensor muscle causes simultaneous contraction of the antagonist muscles. Hypostimulation of the muscle spindle is required. Time adjustment is important to avoid excessive stimulation. Patients with SPS who are hypersensitive to tactile stimuli or have sensitive skin may require adjustment of the stimulation intensity by applying a towel. In addition, in patients who are hypersensitive to sound stimuli, it is necessary to relieve stimulation with earplugs. Although α-motor neuron excitation is expected in SPS through presynaptic suppression, a decrease in the H-wave was observed in this patient. In addition, as the antibody test results were negative, a greater suppression effect was attained. Late responses have been observed in F-waves, and vibration-based therapy may have been effective mainly for F/M waves. However, because this patient underwent home-based rehabilitation, evaluating these methods was not possible.
Vibration-based therapy and massage may be an effective spasticity stretching technique in SPS, as they have previously shown some efficacy and can be effectively accomplished in 30 s. However, this approach may not be suitable for patients with myo-contractures or joint contractures. In addition, hypersensitive patients may not be willing to undergo this treatment.
Abbreviations
SPS, stiff person syndrome; GAD, glutamate decarboxylase; GABA, γ-aminobutyric acid; GlyR, glycine receptor; SPPB, Short Physical Performance Battery; FFD, finger floor distance.
Declarations
Patient’s Perspective
The patient stated that it had become easier for her to wear socks and to perform activities such as outdoor walking and gardening. In addition, she mentioned that vibration-based therapy was less painful and more pleasurable than regular stretching.
Ethics approval and consent to participate
This case involved standard clinical treatment. All interventions and case reporting adhered to the tenets of the Declaration of Helsinki. Due to the retrospective nature of the study, the case report was not subject to an ethics review. The patient provided consent to treatment and case study reporting. In addition, written consent was obtained from the Visiting Nursing Officer for the presentation of the report.
Acknowledgements
I developed the treatment and evaluation plan, maintained records, and conducted statistical analysis. The practitioner was [blinded for review]. I would like to express my gratitude to Mr. Daisuke Fujishima, a representative of the Fujinohana Rehabilitation Visiting Nursing Station, for his cooperation in implementing and measuring physical therapy. I would like to thank Editage (www.editage.jp) for editing the English language. There are no conflicts of interest to disclose in this case report.
References
- Matsui N, Tanaka K, Ishida M, Yamamoto Y, Matsubara Y, Saika R, Iizuka T, Nakamura K, Kuriyama N, Matsui M, Arisawa K, Nakamura Y, Kaji R, Kuwabara S, Izumi Y, Japanese SPS Study. (2023). Prevalence, clinical profiles, and prognosis of stiff-person syndrome in a Japanese nationwide survey. Neurology, Neuroimmunology and Neuroinflammation, 10(6):e200165.
Publisher | Google Scholor - Mutou T. (2019). Stiff-person syndrome and progressive encephalomyelitis with rigidity and myoclonus. In S. Tuji (Ed.), Immune neurological diseases – All about pathophysiology and treatment. Nakayama syoten.
Publisher | Google Scholor - Kenji E, Hiroo A, Takurou O, Shohei M. (2006) Stiff-person syndrome which had difficulty with convulsive treatment. The 362nd Tokyo medical University Clinical Forum, 64:604-613.
Publisher | Google Scholor - Vaiyapuri A, Kashyap P, Kashyap N, Muthusamy H, Unnikrishnan R, Alqahtani M. (2019). Is stiff person syndrome benefited by physical therapy intervention? Summary of case reports. BioMed Research International, 5613680.
Publisher | Google Scholor - Belgen Kaygisiz B.B, Çoban F, Selcuk F. (2021). The effect of clinical pilates-based physiotherapy program for a Stiff Person Syndrome patient: A case report. Acta Neurologica Belgica, 121(1):79-85.
Publisher | Google Scholor - Khan F, Chevidikunnan M.F, Almalki R.A, Mirdad M.K, Nimatallah K.A, Al-Zahrani S, Alshareef A.A. (2020). Stiff-person syndrome outpatient rehabilitation: A case report. Journal of Neurosciences in Rural Practice, 11(4):651-653.
Publisher | Google Scholor - Christopher A.H. (2011). Physical therapist management of stiff person syndrome in a 24-year-old woman. American Physical Therapy Association, 91:1403-1411.
Publisher | Google Scholor - Kawahira, K. (2013). Repetitive facilitation exercise, so called Kawahira methods, might innovate stroke rehabilitation; a strategy of promoting patient's efforts to strengthen neural circuits. Zen Nihon Shinkyu Gakkai Zasshi, 63(4):244-251.
Publisher | Google Scholor - Kawahira K, Simodozono M. (2012). Physiotherapy evidence and practice: Vibration stimulation. Clinical Rehabilitation, 21(6):574-579.
Publisher | Google Scholor - Nakabayashi K, Kodama T, Mizuno K, Ikeda T, Kai N, Fukura T, Kai S. (2011). The inhibitory effect of vibration stimulus on muscle tone of the triceps surae: Analysis of the H/M ratio. Rigakuryoho Kagaku, 26(3):393-396.
Publisher | Google Scholor - Ministry of Education, Culture, Sports, Science and Technology. (2016). New physical fitness test implementation guideline.
Publisher | Google Scholor - Ministry of Education, Culture, Sports, Science and Technology. (2016). Age-specific test results, 2023.
Publisher | Google Scholor - Veronese N, Bolzetta F, Toffanello E.D, Zambon S, De Rui M, Perissinotto E, Coin A, Corti M.C, Baggio G, Crepaldi G, Sergi G, Manzato E. (2014). Association between Short Physical Performance Battery and falls in older people: The Progetto Veneto Anziani Study. Rejuvenation Research, 17(3):276-284.
Publisher | Google Scholor












