

Case Report
Huge Single Bladder Stone: A Case Report from Leku General Hospital, Sidama, Ethiopia
- Asfaw Kibret *
- Muluken Asres
- Bizuneh Sime
- Derbe Adisu
Leku general hospital, 3 ayirgalem medical college, Ethiopia.
*Corresponding Author: Asfaw Kibret, Leku general hospital, 3 ayirgalem medical college, Ethiopia.
Citation: Kibret A, Asres M, Sime B, Adisu D. (2024). Huge Single Bladder Stone: A Case Report from Leku General Hospital, Sidama, Ethiopia. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3 (3):1-3. DOI: 10.59657/2992-9989.brs.24.030
Copyright: © 2024 Asfaw Kibret, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 02, 2024 | Accepted: September 19, 2024 | Published: August 30, 2024
Abstract
Urinary tract calculi are common but huge bladder stones weighing more than 100gm are the rarest occurrences. This is a case of huge bladder stone in 22yrs old adult who presented with acute urinary retention who had repeated urinary tract infection but used to take oral antibiotics from his nearby health centers. Otherwise, he has no predisposing infra vesical obstructive causes. 800gm single stone removed by open cystolithotomy and few reported cases available from Ethiopia.
Keywords: huge single bladder stone; urinary tract calculi; 22yrs old adult; oral antibiotics; health centers
Introduction
Giant urinary bladder calculi are defined as a stone more than 100g in weight. It is rare condition in current practice. There are various conditions believed to be predisposing common factors associated to genito-urinary calculi. Among this urinary tract infections, prostatic hyperplasia, uretral stricture, intravesical foreign body encrustation are common predisposing causes of urinary bladder stones. Bladder stones develop when mineral deposits in urine begin to crystallize and form a hard mass. These stones can affect men, women, and children although men are most likely to develop stones as they age increases [1].
Untreated bladder stone can lead to damage to urinary tract, recurrent stone formation or infection. Urinary stones of up to 5 mm of diameter are known to pass spontaneously through the urinary tract; whereas those exceeding 7 mm of diameter almost always require surgical intervention [2,3].
The incidence of bladder stones among younger patients is low and that of large stones is rare. The formation of a large stone occurs over a long period of time and it may be complicated by concurrent serious infections, requiring open surgery for stone removal. This case report is a young man with huge bladder stone with preceding recurrent urinary tract infection and treated locally by oral medications. This delayed him to present to our set up at least which had imaging services for better diagnosis of such cases.
Case Presentation
This is a 22yrs old male patient presented to leku general hospital, one of the general hospital in sidama, Ethiopia, on may,2024.Upon presentation he was complaining difficulty of passing urine for last 24hrs,he had previous long standing urinary complains like dysuria, urinary frequency, has also lower abdominal burning type of abdominal pain, has also urethral discharge after urination sometimes, for which he repeatedly visited his nearby health center and treated as they diagnosed him for urinary tract infection. Inspite of the treatment his complains continued intermittently. during presentation to our hospital, he was in severe lower abdominal pain due to urine retention and bladder was full, he had minimal tenderness on lower abdominal palpation. He had been catheterized at emergency and 2L turbid urine was evacuated then work up started. On laboratory investigation Wbc=12000, Hgb=10.5g|dl, PLT=250,000. Creatinine 0.9mg|dl, on urine analysis there was many bacteria, and full of RBC, the available imaging in the hospital also sent and came with the report of 9.5 x7.4cm bladder stone. There was no evidence of any pathology on the upper urinary tract, no sign of hydronephrosis. Then the patient started antibiotics and after 1week elective surgery was scheduled and open cystolithotomy done to remove 800mg single stone (figure 1). Post operatively the patient developed surgical site infection and bladder dehiscence and reoperated and bladder repair and wound care done, lately discharged with stable condition, catheter removed on the 3rd week postoperatively.
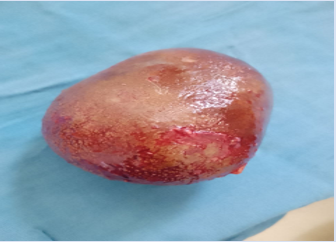
Figure 1: Huge bladder stone removed by open cystolithotomy at Leku general hospital, Sidama, Ethiopia
Discussion
Bladder calculi are the rarest form and account for 5% of urinary calculi and usually occur because of bladder outlet obstruction, neurogenic voiding dysfunction, urinary tract infection, or foreign bodies. Males are more likely to be affected than females. Bladder stones weighing more than 100gm are considered as huge and they are rare occurrences and there were few reported cases in literatures [1,2].
There are different predisposing factors which are baseline cause for development of urinary bladder caliculi. Bladder outlet obstruction especially in aged patients due to benign prostatic hyperplasia and urethral stricture. Chronic urinary retention, recurrent urinary tract infection is also predisposing conditions for bladder calculi. These all may lead to concentrated residual urine and predispose to stone formation [3,4]. Bladder stones are mostly associated with renal or ureteral calculi, and they rarely ever occur without associated upper urinary tract calculi, as in our patient. There were also environmental and lifestyle associations of bladder stone formation. The incidence of urolithiasis is higher in the population with more laborious work, because it is more likely to have an unhealthy lifestyle, irregular diet, and less fluid intake thus leading to dehydration. Furthermore, people with outdoor working activities and high temperatures like in our patient who is a farmer and living in hot environment, are twice as likely to suffer from urolithiasis. Hot temperature accelerates evaporation from skin, accompanied by low fluid intake, which can lead to dehydration and concentrated urine. Excessive exposure to sunlight can lead to higher production of vitamin D, which further drives calcium absorption in the gut [5,6].
Bladder stone can be asymptomatic and sometimes identified incidentally. But most patients present with urinary symptoms like dysuria, lower abdominal pain, and hematuria. Like in our patient they may present with urinary retention. There are also patients reported with renal failure [4,6].
The diagnosis of vesical calculi requires a high index of suspicion. A history of suprapubic pain that is aggravated by exercise, an interruption of the urinary stream, and terminal hematuria are helpful but not pathognomonic of the disease because they may be caused by other lesions in the bladder. The preferred method for diagnosis is cystoscopy, but an X-ray or an ultrasound is sometimes enough. Because of its size, cystolithotomy is the correct treatment for a giant bladder stone. As the urological surgery recommendation there are a number of techniques and modalities available to remove bladder stones. Relieving the obstruction, eliminating the infection, meticulous surgical technique, and accurate diagnosis are essential in their treatment [7].
Even in urologic centers where cystoscope is available, open cystolithotomy is the preferred mode of treatment for large bladder stone. Our set up I not a urologic set up but as a general resource limited set up, open cystolithotomy is done regularly despite of the size of the stone [5,7].
Conclusion
Giant bladder stone is a rare condition though urolithiasis is common. In developing nations patients present late due to their economic factors or due to the poor set ups in the primary care to identify the cases early or due to unavailability of imaging services. Huge bladder stone can be formed without infravesical bladder outlet obstructions like this case.
Declarations
Ethics approval and consent-the study was conducted according to the guidelines of the Declaration of Helsinki and approved by leku general hospital ethical committee.
Patient consent for publication-consent was obtained from the patient for publication of the patient data image included in this case report.
Conflict of interest
No conflict of interest
Funding
No fund taken for this case report
References
- Tahtalı İN, Karataş T. (2014). Giant bladder stone: A case report and review of the literature. Turk J Urol, 40(3):189-191.
Publisher | Google Scholor - Napitupulu T, Susanto M, Duma G, Yudha Rahman E. (2022). Giant Bladder Stone: A Case Report and Literature Review. JMA J. 5(3):384-388.
Publisher | Google Scholor - Wei X, Qin Y, Wang X, Qian J, Niu S, Tu S, Yao J. (2022). Giant bladder stone: A case report. Exp Ther Med, 24(2):535.
Publisher | Google Scholor - Katsimperis S, Pikramenos K, Livadas K, Chatzikrachtis N, Bellos TT. (2022). Giant Bladder Stone: A Case Report. Cureus, 14(5):e25439.
Publisher | Google Scholor - Douenias R, Rich M, Badlani G, Mazor D, Smith A. (1991). Predisposing factors in bladder calculi: review of 100 cases. Urology, 37(3):240-243.
Publisher | Google Scholor - Ma C, Lu B, Sun E. (2016). Giant bladder stone in a male patient: a case report. Medicine (Baltimore), 95(30).
Publisher | Google Scholor - Molla YD, Getahun GM, Assefa MA. (2023). Giant bladder stone a rare cause of renal failure, a case report. Int J Surg Case Rep, 105:108085.
Publisher | Google Scholor - Schwartz BF, Stoller MZ. (2000). The vesical calculus. Urol Clin North Am, 27:333-346.
Publisher | Google Scholor












