

Case Report
Giant Left Atrial Appendage Aneurysm (LAAA)
- Shruthi Shekar *
Star Hospitals, Hyderabad, India.
*Corresponding Author: Shruthi Shekar, Star Hospitals, Hyderabad, India.
Citation: Shruthi Shekar. (2024). Giant Left Atrial Appendage Aneurysm (LAAA), Journal of Clinical Cardiology and Cardiology Research, BioRes Scientia Publishers. 3(4):1-4, DOI: 10.59657/2837-4673.brs.23.015
Copyright: © 2024 Shruthi Shekar, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 27, 2023 | Accepted: November 18, 2024 | Published: November 25, 2024
Abstract
A 27-year-old man presented to our hospital complaining of Palpitation. Based on the results of echocardiography, an aneurysm of the left atrium was suspected. Cardiac MRI confirmed the diagnosis of Left Atrial Appendage Aneurysm. The patient underwent an Aneurysmectomy via a median sternotomy with cardiopulmonary bypass. The patient had an uneventful postoperative clinical course and was discharged from the hospital on the 10th day in a satisfactory condition.
Keywords: cardiac MRI; 27-year-old patient; left atrium
Case Presentation
A 27-year-old male patient had 2 episodes of CVA with right hemiplegia and aphasia for the last 5 months. Came to the emergency with complaints of palpitations.
Atrial Fibrillation +
Chest Radiograph: Patient underwent a chest radiograph as a part of routine workup, which was notable for an abnormal well-defined bulging left cardiac border. Lung fields were otherwise normal (Figure 1). On Echo: Large aneurysm arising from LA with clot within. Normal LV function.

Figure 1: Gross enlargement of cardiac silhouette showing abnormally prominent and bulging of left heart border.
MRI Brain: MRI brain was performed next for the evaluation of neurological symptoms which showed encephalomalacia changes in the left temporal lobes. Rest of the brain showed normal grey and white matter differentiation.
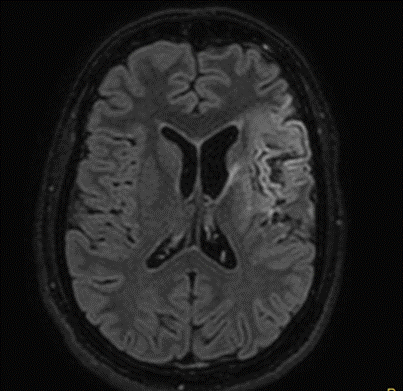
Figure 2: Axial FLAIR images showing abnormal signal intensity area involving left temporal cortices representing encephalomalacia changes.
MRA
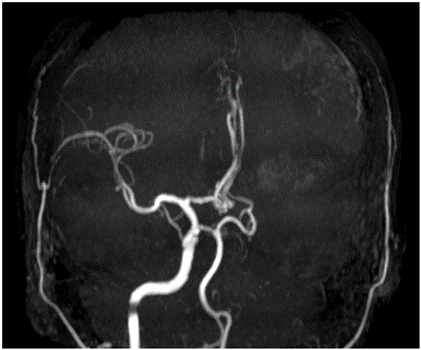
Figure 3: Time of Flight MIP image showing complete occlusion of Left ICA.
Cardiac MRI
- Large Aneurysmal dilatation of LAA (measuring 11.5 x 10.6 x 8 cm) with a wide ostium with well-defined hypointense lesion (of size 4 x 2.7 x 2.5 cm) noted within the Aneurysm, at the aneurismal apex. -- S/o LAA Aneurysm with Thrombus.
- Non dilated RV and LV with good biventricular systolic function.
- Normal Mitral valve.
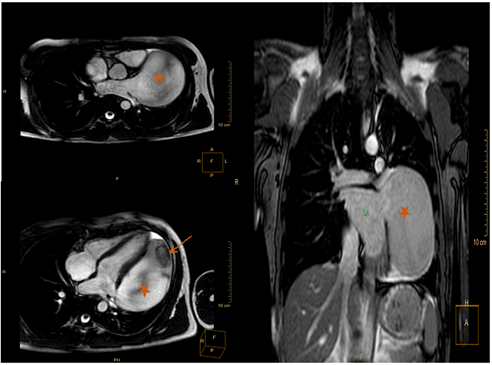
Figure 4: Cardiac MRI.
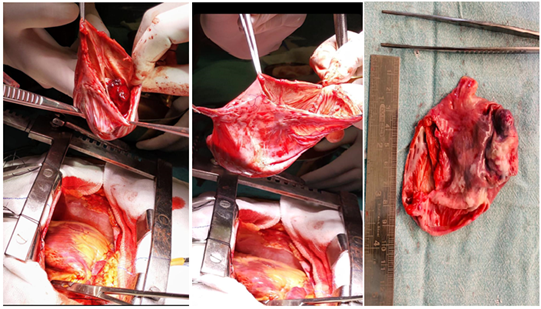
Figure 5: Intra Operative Images.
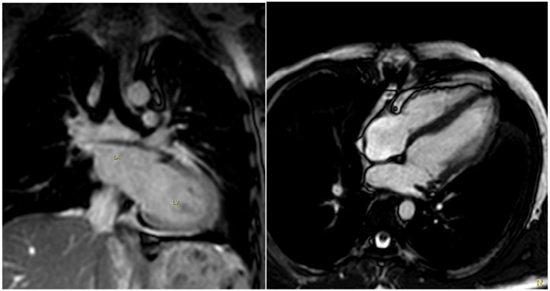
Figure 6: Post Operative Image: No Residual Lesion Noted.
Discussion
Left atrial appendage aneurysm (LAAA) is regarded as localized or diffuse dilatation of the left atrial appendage. The mean age of presentation is 23.5 years however, it may vary widely from 1 month to 66 years [1].
It is a very rare entity with less than a hundred cases reported in literature [2]. An aneurysm of the left atrial appendage is one of the rare but potentially hazardous heart defects. The risk of lethal complications grows with its size. To date, about 150 cases of this defect have been described in the literature. It may be Congenital or Acquired.
Types of LAAA
- Similar to our case, if seen as a primary pathology with an otherwise normal atrial chamber, it is considered congenital.
- Congenital aneurysms are rare and thought to be caused by dysplasia of the musculi pectinate [1]. These are associated with supraventricular tachyarrhythmias and systemic thromboembolism.
- Absence of coexisting mitral valve disease, wide aneurysmal necks, and intrapericardial location were compatible with a congenital etiology.
- However, should be considered Acquired if it has developed secondary to raised left atrial pressure [3]. This condition is caused by dysplasia of the atrial muscle bands and can also occur as sequelae of mitral valve disease or left ventricular myocardial disease [4] which can be due to increased pressure in the left atrium or weakening of the atrial wall [5]. Acquired left atrium aneurysms are caused by mitral valve disease.
Clinical Presentation
Majority of the patients remain asymptomatic, there is a propensity for embolic events and supraventricular arrhythmias likely secondary to the stasis of blood within the aneurysm [5]. Chest pain is another presentation, due to tension over the pericardium or by temporary compression on the coronary arteries. Due to aneurysmal compression, there may be reduced left ventricular compliance leading to raised ventricular filling pressures and diastolic dysfunction.
Neonates and infants are more prone to congestive heart failure and respiratory distress with large aneurysms because the condition may be associated with physical compression of the pulmonary veins and airway obstruction, respectively [6]. Mild symptoms may be treated with conservative management while in cases of compressive symptoms surgical intervention is needed to be performed [6].
Most of the authors have proposed surgical resection as the standard treatment regardless of the presence or absence of symptoms in order to prevent the occurrence of atrial fibrillation, thromboembolic events or myocardial dysfunction [3].
Conclusion
This case report demonstrates that a Large LAAA has probably led to the propensity of thromboembolic events that resulted in stroke. There were no signs of heart failure.
Differential Diagnosis
- Left atrial appendage aneurysm
- Left Atrial Diverticula
- Cystic Para Cardiac Tumour
- Pericardial Cyst
References
- Akhtar P, Habib S, Hussain M, Tasneem H, Hussain A, et al. (2007). Congenital Giant Aneurysm of The Left Atrial Appendage: Diagnosis and Management. Pakistan Heart Journal. 40(1-2):14-18.
Publisher | Google Scholor - Ota C, Kimura M, Kitami M, Kure S. (2018). Asymptomatic Left Atrial Appendage Aneurysm (LAAA) With Pericardial Defect in A 1-Year-Old Girl. BMJ Case Reports.
Publisher | Google Scholor - Sarin SS, Bindra T, Chhabra GS. (2012). A Giant Left Atrial Appendage Aneurysm with A Large Pinball-Like Thrombus in A 2-Year-Old. Annals of Pediatric Cardiology. 5(2):215-216.
Publisher | Google Scholor - Bamous M, Aithoussa M, Abetti A, Boulahya A. (2017). Congenital Left Atrial Appendage Aneurysm: Atypical Presentation. Annals of Pediatric Cardiology. 10(3):293-294.
Publisher | Google Scholor - Valentino MA, Al Danaf J, Morris R, Tecce MA. (2017). Giant Left Atrial Appendage Aneurysm: A Case of Mistaken Identity. Journal of Cardiology Cases. 15(4):129-131.
Publisher | Google Scholor - Chen Y, Mou Y, Jiang LJ, Hu SJ. (2017). Congenital Giant Left Atrial Appendage Aneurysm: A Case Report. Journal of Cardiothoracic Surgery. 12(1):1-5.
Publisher | Google Scholor











