

Research Article
From Concept to Clinical Implementation: Clinical Utilization of Mentzer Score as A Screening Tool for The Differentiation of Iron-Deficiency Anemia and Beta Thalassemia Trait
1 Department of Haematology, Dr. Essa Laboratory and Diagnostic Centre, Karachi, Pakistan.
2 Department of Allied Health and Medical Sciences, Al-Kawthar University, Karachi, Pakistan.
3 Department of Research Studies, National Institute of Blood Diseases and Bone Marrow Transplantation, Pakistan.
*Corresponding Author: Aisha Arshad, Department of Haematology, Dr. Essa Laboratory and Diagnostic Centre, Karachi, Pakistan.
Citation: Aisha Arshad, Laraib Majeed (2025). From Concept to Clinical Implementation: Clinical Utilization of Mentzer Score as A Screening Tool for The Differentiation of Iron-Deficiency Anemia and Beta Thalassemia Trait. Journal of Hematology Research and Blood Disorders, BioRes Scientia Publishers. 1(1):1-6. DOI: 10.59657/jhrbd.brs.25.004
Copyright: © 2025 Aisha Arshad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 13, 2025 | Accepted: March 27, 2025 | Published: April 10, 2025
Abstract
Introduction: Iron deficiency anemia (IDA) and Thalassemia minor are the major causes of hypochromic and microcytic anemia. The present study was to determine the role of mentzer score in IDA and thalassemia trait patients from various parts of Pakistan who presented with microcytic hypochromic anemia at our centre.
Materials And Methods: This cross-sectional study was conducted at the Dr. Essa Laboratory and Diagnostic Centre hematology department in Karachi from June 2024 to January 2025. The complete blood picture (CBC) was done by using XP-100 Sysmex analyzer. The mentzer score was calculated by dividing MCV with RBC. The score >13 was considered as an operational criterion for IDA. The mean and standard deviation were calculated for the continuous variables. The sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy were calculated by SPSS version 25.
Results: A total of 230 patients were included. The mean age of the patients was 22±14.4 years. A significantly low Hb with High RBC counts HbA2 levels were observed in patients with Thalassemia minor (p=<0.001). The Hb and RBC indices were significantly low in IDA patients(p=<0.001). The sensitivity of Mentzer index >13 in IDA patients was found to be 73.2%.
Conclusion: Mentzer score can be used as a simple and easy to calculate index for the differentiation of IDA. However, Hb electrophoresis is the reliable test for the diagnosis of Thalassemia minor.
Keywords: iron deficiency anemia; beta thalassemia trait; mentzer score
Introduction
Iron deficiency anemia (IDA), the most prevalent hematological condition in newborn and children, is caused by a lack of iron to promote hemoglobin (Hb) synthesis [1-3]. The primary cause of hypochromic microcytic anemia worldwide is IDA, which is mostly brought on by the body's diminished iron reserves. The World Health Organization estimates that iron deficiency is responsible for about half of the 1.62 billion instances of anemia that occur globally.1It is far more common in Pakistan and other third world countries[4]. Its prevalence can range from 19% in wealthy nations to 35-75% in developing nations [5].
IDA is classified as hypochromic (mean corpuscular hemoglobin, or MCH less than 25pg), and microcytic (mean corpuscular volume, or MCV, is less than 73 Fl [6]. Iron supplements can be disastrous if thalassemia is the cause of the anemia, even though they are extremely beneficial in cases of iron deficiency anemia (IDA). The symptoms of shortness of breath, exhaustion, lightheadedness, and irritability are about the same for both of these anemic types. Many people with β TT have no symptoms, while those with iron deficient anemia have more noticeable symptoms [2]. Microcytic hypochromic anemia is depicted by the complete blood counts in both the conditions [7].
To distinguish between the two circumstances, particular tests are required. Ferritin levels and iron tests are used to confirm iron deficiency anemia, but hemoglobin electrophoresis is required to estimate HbA2 for the diagnosis of β TT. A HbA2 level more than 3.5% is thought to be pathognomonic for beta thalassemia [8-10].
The development of indices based on blood counts was prompted by the inability to distinguish between iron deficiency anemia and beta thalassemia trait based on blood pictures and the high cost of procedures such as Hb electrophoresis and iron studies. The Mentzer Index, created by Mentzer in 1973, is the most often utilized. Low red blood cell (RBC) counts and low mean corpuscular volume (MCV) are the results of bone marrow producing fewer red blood cells in iron deficiency anemia. Thus, >13 is the Mentzer Index. In thalassemia, the production of red blood cells is normal, but because of a malfunctioning beta globin chain, the red blood cells are more fragile and smaller, which leads to a low mean corpuscular volume and a normal red blood cell count and Mentzer index is less than 13 [2,11].
Dr. Thomas Cooley was the first to describe thalassemia in infants of Mediterranean descent about a century ago [12]. Thalassemia major patients have a reduced life expectancy and severe anemia during the first two years of life if untreated βTT is a kind of thalassemia that manifests in the prenatal population and causes moderate anemia in later life. Since iron treatment can have disastrous side effects, such as hepatic and cardiac damage from iron overload, diagnosing beta thalassemia is crucial. Additionally, the detection of a partner's hemoglobinopathy and the prenatal diagnosis of an offspring using chorionic villous sample might result from a thalassemia diagnosis [13].
In Pakistan, consanguinity is the most frequent contributing factor, and the carrier rate is 5-8% [14]. This hereditary condition presents a significant concern to the health sector in a developing nation like Pakistan since regular blood transfusions and iron chelation are costly, which may be out of reach for some affected individuals.Genetic counselling, prenatal diagnostics, and carrier identification are examples of preventive measures. Hemoglobin electrophoresis, which is necessary for carrier identification, is another costly test that makes it nearly hard to do on the entire population or even high-risk populations [15]. This calls for a few low-cost screening assays that are applicable to large populations.
There are numerous screening tests available to distinguish between βTT and IDA including the Red Cell Distribution Index (RDWI), England & Fraser Index (E&F), Mentzer Index (MI), Shine & Lal Index, Green & King Index (G&K), Red Cell Distribution, and Red Blood Cell Count [16]. The Mentzer Index has demonstrated varying validation statistics when used as a screening or distinguishing tool. It has been adopted in many parts of the world because of its great [11,17] acceptability.The main purpose of the present study was to determine the role of mentzer score in IDA and thalassemia trait patients from various parts of Pakistan who presented with microcytic hypochromic anemia at our centre.
Materials and Methods
A descriptive cross-sectional study was conducted at the Dr. Essa Laboratory and Diagnostic Centre hematology department in Karachi from June 2024 to January 2025. Using non-probability purposive sampling was the sampling technique. Patients with hypochromic microcytic anemia, regardless of gender, between the ages of 01-45 years, were included in the study. Patients with additional hematological conditions, chronic illness anemia, rejection of consent, and recent surgical operations were excluded. Permission from the Institutional Review Committee was obtained to conduct this study. Before any of their data was utilized for research reasons or their kid was enrolled in the study, the parents of all patients under the age of sixteen provided their informed consent.
Following sterile collection, the samples were examined for iron and CBC analyses. Hemoglobin ≤11.5 g/dl, MCV ≤ 77 fl, MCH ≤ 25 pg, transferrin saturation less than 12 percent, and Mentzer index (MCV/RBC) ≥ 13 are the operational criteria for IDA. Iron, TIBC, ferritin level, hemoglobin and red cells indices were all measured for the patient. The proforma contained the findings of the qualitative variables (anemia length, gender, marital status, and previous anemia history) and quantitative components (age, hemoglobin, and anemia duration).
Statistical Analysis
SPSS Version 25 was used for data analysis. The mean and standard deviation were calculated for the continuous variables of age, hemoglobin level, and RBC parameters. Frequencies and percentages were used to determine the Mentzer index (yes/no). Sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy were all calculated with the following formulae.
Sensitivity = [true positive/ (true positive+ false negative)] * 100
Specificity = [true negative/true negative+ false negative] *100
Results
A total of 230 patients were included. The mean age of the patients was 22±14.4 years. Out of 230, the percentage of female was high 156(67.8%) as compared to males 74(32.1%). The sign and symptoms showed most prevalence of Weakness seen in 200(86.9%), followed by vertigo 165 (71.7%) as shown in figure 1. The hematological characteristics of the patients were mentioned in table 1.the Thalassemia minor was diagnosed with the elevated levels of Hemoglobin A2 which has been depicted in table 2.
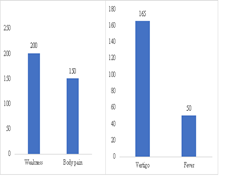
Figure 1(a, b): (a) Frequency of sign observed (b) Frequency of symptoms observed
Table 1: Hematological characteristics in IDA and Thalassemia minor patients
| Parameters | IDA n (%) | Thal Minor n (%) | P-value |
| WBC(*109/L) | 9.68±4.10 | 8.06±4.09 | 0.435 |
| RBC(*1012/L) | 4.45±0.82 | 5.21±1.21 | less than 0.001 |
| Hb (g/dl) | 7.8±2.57 | 9.2±2.36 | less than 0.001 |
| HCT (%) | 30.1±1.05 | 30.3±2.59 | 0.333 |
| MCV (fl) | 71.8±14.0 | 66.2±8.5 | less than 0.001 |
| MCH (pg) | 22.1±4.8 | 19.9±2.40 | less than 0.001 |
| MCHC(g/dl) | 29.0±2.91 | 29.4±2.21 | 0.632 |
| Platelets(*109/L) | 373±140 | 345±112 | less than 0.001 |
| TIBC (ug/dl) | 96.2±20.1 | 55±35.3 | less than 0.001 |
| Ferritin(ng/ml) | 30.2±40.0 | 66±59.8 | less than 0.001 |
WBC: White Blood Cells, RBC: Red Blood Cells, Hb: Hemoglobin, HCT: Hematocrit, MCV: Mean Cells Volume, MCH: Mean Cell Hemoglobin, MCHC: Mean Cells Hemoglobin Concentration, TIBC: Total Iron Binding Capacity, IDA: Iron Deficiency Anemia, Thal: Thalassemia n: Number of patients, %: Percentage.
Table 2: Comparison of Hemoglobin variants in IDA and Thalassemia Minor Patients
| Parameters | IDA n (%) | Thal Minor n (%) | P-value |
| HbA | 97.1±0.74 | 94.7±0.9 | less than 0.001 |
| HbF | 0.29±0.12 | 0.35±0.37 | 0.662 |
| HbA2 | 2.38±0.55 | 4.43±0.62 | less than 0.001 |
HbA: Adult Hemoglobin, HbF: Fetal Hemoglobin, HbA2: Hemoglobin A2, Thal: Thalassemia, n: Number of patients, %: Percentage.
The Mentzer index used as a diagnostic tool to rule out the iron deficiency by using iron as gold standard. The analysis shows a sensitivity of 73.2% which indicate that the Mentzer index was able to identify a substantial proportion with iron deficiency however, it has limited ability to distinguish the individual who did not have IDA the specificity was low at 17.0%. Among all the patients that actually had a disease and tested positive through Mentzer index were 77.5%. And 14.0 % were actually healthy who tested negative. Overall, the Mentzer index correctly identifies 61.7% of all patients with and without disease as depicted in table 3.
Table 3: Sensitivity and Specificity of Mentzer score in IDA and Thalassemia minor patients
| Parameters | Formula | Calculation | Percentage (%) |
| Sensitivity | TP/TP+FN x 100 | 134/134+49 | 73.2% |
| Specificity | TN/TN+FP x 100 | 8/8+39 | 17.0% |
| Positive predictive value | TP/TP+FP x 100 | 134/134+39 | 77.5% |
| Negative predictive value | TN/TN+FN x 100 | 8/8+49 | 14.0% |
| Diagnostic accuracy | TP+TN/Total x 100 | 134+8/230 | 61.7% |
TP: True Positive, FN: False Negative, FP: False Positive, TN: True Negative
Discussion
Iron deficiency anemia (IDA) and beta thalassemia trait (βTT) are the most common causes of microcytic hypochromic anemia. Numerous indices have been presented that are based on characteristics related to blood cell counts [18]. For the diagnosis of IDA, doctors typically employ tests including serum ferritin levels, total iron-binding capacity, serum iron, and complete blood counts [19]. In settings with limited resources, IDA manifests as low hemoglobin levels, microcytic and hypochromic red cells in peripheral smears, and higher hemoglobin levels following two months of iron therapy [16,20].
In the current study, the MCV was significantly low in thal minor patients with the mean of 66.2±8.5 as compared to IDA group 71.8±14.0, p=less than 0.001which was similar with the findings of Shah et al.[21] The significantly low Hb with high RBC counts were observed in thal minor group, which was consistent with the earlier research comparing several discriminant functions in IDA and BTT patients Similarly, in the study conducted by Sirdah et al. for BTT group's MCV was 66.44 ± 5.29, whereas[22] the IDA group's was 72.57 ± 5.83. The BTT group's RBC count was also was 4.92 ± 0.61 in the IDA group and 5.93 ± 0.57 [23].
For the diagnosis of thal minor, haemoglobin electrophoresis or HPLC is used to test the HbA2 percentage of RBCs [24]. In the present study, significant high levels of HbA2 with mean of 4.43±0.62, p= less than 0.001 as observed in thal minor as compared to IDA patients [25]. A repeat serum iron with electrophoresis should be performed after 16–20 weeks of iron therapy, since research has shown that iron deficiency directly affects the rates of HbA2 production in the bone marrow. This will guarantee that HbA2 levels have improved [26].
In an effort to distinguish between IDA and beta thalassemia using basic blood count values, a number of indices have been employed; however, none have been found to be 100% sensitive and 100% specific to date. Out of all the pertinent indices, the Mentzer Index offers the highest sensitivity and specificity [27].
In the present study the Mentzer Index was analyzed as a screening tool to distinguish between IDA and ΒTT which was also reported in previous studies [11,19,21]. The sensitivity of the Mentzer index in the present study was 73.2%, indicating that it was moderately effective in identifying patients who truly had IDA. Only a small proportion of true IDA cases were incorrectly classified as non-IDA, showing relatively good detection of actual cases. Patients diagnosed with that minor and having mentzer index >13 was 17%. Therefore, the Mentzer Index is more accurate in identifying IDA and ruling out βTT. This was also the conclusion of a research studies carried out in India, Indonesia and South Africa [27-29]. The Mentzer index had the highest reliability when compared to other haematological indices used to distinguish between the two significant causes of microcytic hypochromic anemia as reported in previous studies [11,30]. Therefore, the Mentzer score index can be used as a screening tool for the identification of IDA. However, Hb electrophoresis should be used as a diagnostic test for the thalassemia minor state.
Limitations of the study
This was a single centre study with limited number of sample size.
Conclusion
Mentzer index can be used as an initial screening tool in the diagnosis of IDA and differentiating beta thalassemia minor in resource limited countries where diagnostic tests are expensive. Thus, the Mentzer score can be used as a simple, reliable and budget friendly tool along with Hb electrophoresis for the confirmation of thalassemia state. However, multi centre studies with large number of sample size are needed to validate mentzer score as a sensitive marker for the diagnosis of IDA.
Abbreviations
IDA: Iron deficiency Anemia
WBC: White Blood Cells
RBC: Red Blood Cells
Hb: Hemoglobin
HCT: Hematocrit
MCV: Mean Cells Volume
MCH: Mean Cell Hemoglobin
MCHC: Mean Cells Hemoglobin Concentration
Thal: Thalassemia
n: Number of patients
%: Percentage
HbA: Adult Hemoglobin
HbF: Fetal Hemoglobin
HbA2: Hemoglobin A2
Declarations
Institutional Review Board Statement and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board. Informed consent was obtained from all subjects involved in the study.
Acknowledgement
We are thankful to all patients for their participation in the study.
Data Availability Statement
The data and materials supporting the findings of this study are available from the corresponding authors upon reasonable request.
Competing of Interest
The authors declare that they have no competing interests.
Funding
This research received no funding.
Authors' contributions
AA: Concept, design, data collection, manuscript writing of the original draft, editing, critical review and approval of final manuscript draft, LM: Contributed in statistical analysis.
References
- Ntaios G, Chatzinikolaou A, Saouli Z, Girtovitis F, Tsapanidou M, et al., (2007) Discrimination indices as screening tests for β-thalassemic trait. Annals of hematology,86:487-491.
Publisher | Google Scholor - Tabassum S, Khakwani M, Fayyaz A, Taj N., (2022). Role of Mentzer index for differentiating iron deficiency anemia and beta thalassemia trait in pregnant women. Pakistan journal of medical sciences. 38(4Part-II):878.
Publisher | Google Scholor - Arshad AA, Abdullah FFE, Essa NNF. 5573836 (2023). Clinicohematological characteristics of iron deficiency anemia and hemoglobinopathies in pakistan; an experience of non-hospital-based laboratory. HemaSphere.,7(S1):50.
Publisher | Google Scholor - Ullah A, Sohaib M, Saeed F, Iqbal S. (2019). Prevalence of anemia and associated risk factors among pregnant women in Lahore, Pakistan. Women & health.59(6):660-671.
Publisher | Google Scholor - Öztürk M, Öztürk Ö, Ulubay M, Karaşahin E, Özgürtaş T, et al., (2017). Anemia prevalence at the time of pregnancy detection.Turkish journal of obstetrics and gynecology.14(3):176.
Publisher | Google Scholor - Warner MJ, Kamran MT. (2023) Iron deficiency anemia. StatPearls [Internet]: StatPearls Publishing.
Publisher | Google Scholor - Jameel T, Baig M, Ahmed I, Hussain MB, bin Doghaim Alkhamaly M.(2017).Differentiation of beta thalassemia trait from iron deficiency anemia by hematological indices. Pakistan journal of medical sciences,33(3):665.
Publisher | Google Scholor - MADAN N, SIKKA M, SHARMA S, RUSIA U, KELA K. (1999).Red cell indices and discriminant functions in the detection of beta-thalassaemia trait in a population with high prevalence of iron deficiency anaemia. Indian Journal of Pathology and Microbiology.42(1):55-61.
Publisher | Google Scholor - Harrington AM, Ward PC, Kroft SH. (2008). Iron deficiency anemia, β-thalassemia minor, and anemia of chronic disease: a morphologic reappraisal. American journal of clinical pathology.129(3):466-471.
Publisher | Google Scholor - De Sanctis V, Kattamis C, Canatan D, Soliman AT, Elsedfy H, et al., (2017) β-thalassemia distribution in the old world: an ancient disease seen from a historical standpoint. Mediterranean journal of hematology and infectious diseases. 9(1): e2017018.
Publisher | Google Scholor - Hehapoglu A, Ozgurhan G, Demir AD, Uzuner S, Nursoy MA, et al., (2014). Hematological indices for differential diagnosis of Beta thalassemia trait and iron deficiency anemia. Anemia (1):576738.
Publisher | Google Scholor - Rund D. Thalassemia (2016). Modern medicine battles an ancient disease. American journal of hematology. 91(1):15-21.
Publisher | Google Scholor - Origa R. Beta-thalassemia. (2021).
Publisher | Google Scholor - Ahmed S, Saleem M, Modell B, Petrou M. (2002). Screening extended families for genetic hemoglobin disorders in Pakistan. New England journal of medicine.347(15):1162-1168.
Publisher | Google Scholor - Ghafoor M, Sabar MF, Sabir F. (2021). Prevention programmes and prenatal diagnosis for beta thalassemia in Pakistan: A narrative review. Journal of Pakistan Medical Association. 71(1):326-.
Publisher | Google Scholor - Sherali A, Ahad A, Tikmani SS, Sohail S (2023). Screening of Iron deficiency Anemia in children using Mentzer index in Pakistan: a cross sectional study. Global Pediatric Health. 10:2333794X221130986.
Publisher | Google Scholor - Awais M, Ahmad A, Farid A, Khan H (2022). Mentzer index as a screening tool for iron deficiency anemia in 6-12 years old children. Journal of Postgraduate Medical Institute. 36(4):235-238.
Publisher | Google Scholor - Garg S, Srivastava A, Singh S, Jaiswal R, Singh YK (2016). Role of hematological indices in the screening of Β-thalassemia minor (trait) and iron deficiency anaemia. American research journal of Hematology.1(1):1-5.
Publisher | Google Scholor - Idrees M, Khan JUA, Riaz H, Shah MA, Shah H, et al., (2023). Utilization of Mentzer Index to Discriminate Between Beta Thalassemia Minor and Anemia of Iron Deficiency, Followed by HPLC. Pakistan Journal of Medical & Health Sciences.17(01):843-.
Publisher | Google Scholor - Zafar M, Tabassum A, Cheema QA, Mazhar SB (2020). Role of red cell distribution width and Mentzer index in differentiating iron deficiency anemia from anemia due to β thalassemia trait. Journal of South Asian Federation of Obstetrics and Gynaecology.11(5):297-300.
Publisher | Google Scholor - Shah TP, Shrestha A, Agrawal JP, Rimal S, Basnet A (2023). Role of Mentzer index for differential diagnosis of iron deficiency anaemia and beta thalassemia trait. J Nepal Health Res Counc.,21(1):99-102.
Publisher | Google Scholor - Jabeen M, Iqbal H, Ahmed A, Ahsan J, Shujaat U, et al., (2023) Differentiation of Beta-Thalassemia Trait (β-TT) from Iron Deficiency Anaemia (IDA) by Haematological Indices. Pakistan Armed Forces Medical Journal.73(3):829.
Publisher | Google Scholor - Sirdah M, Tarazi I, Al Najjar E, Al Haddad R (2008). Evaluation of the diagnostic reliability of different RBC indices and formulas in the differentiation of the β‐thalassaemia minor from iron deficiency in Palestinian population. International journal of laboratory Hematology. 30(4):324-330.
Publisher | Google Scholor - Kaur G, Tyagi S, Seth T, Mahapatra M, Viswananthan GK, et al., (2023). Comparison of HbA2 Using High Performance Liquid Chromatography Versus Haemoglobin Capillary Zone Electrophoresis. Indian Journal of Hematology and Blood Transfusion.39(4):572-578.
Publisher | Google Scholor - Değermenci Ş, Aslan D (2024). HbA2 levels in children with β-thalassemia trait associated with iron deficiency: A perspective for pediatricians. American Journal of Clinical Pathology. 162(6):544-548.
Publisher | Google Scholor - Ravanbakhsh M, Mousavi SA, Zare S (2016). Diagnostic reliability check of red cell indices in differentiating iron deficiency anemia (IDA) from beta thalassemia minor (BTT). Hormozgan Medical Journal.20(3).
Publisher | Google Scholor - Bose S, Maimoon S (2018). Is Mentzer index a reliable diagnostic screening tool for beta thalassemia trait. IOSR J Dent Med Sci.,17(7):7-11.
Publisher | Google Scholor - Alam SLS, Purnamasari R, Bahar E, Rahadian Kyk (2014). Mentzer index as a screening tool for iron deficiency anemia in 6-12-year-old children. Paediatrica Indonesiana,54(5):294-298.
Publisher | Google Scholor - Lawrie D, Glencross D (2015). Use of the Mentzer index will assist in early diagnosis of iron deficiency in South African children. SAMJ: South African Medical Journal.,105(9):703-.
Publisher | Google Scholor - Sundh A, Kaur P, Palta A, Kaur G (2020). Utility of screening tools to differentiate beta thalassemia trait and iron-deficiency anemia-do they serve a purpose in blood donors? Blood research.55(3):169-174.
Publisher | Google Scholor




















