

Editorial Article
Focus on Dangerous Skeletal Fluorosis, how it Can be Prevented in Humans
- Shanti Lal Choubisa 1
Department of Advanced Science and Technology, National Institute of Medical Science and Research, NIMS University Rajasthan, Jaipur, Rajasthan, India; Former Department of Zoology, Government Meera Girls College, MLS University, Udaipur, Rajasthan, India.
*Corresponding Author: Shanti Lal Choubisa
Citation: Shanti L. Choubisa. (2024). Focus on Dangerous Skeletal Fluorosis, how it can be Prevented in Humans, Pollution and Community Health Effects, BioRes Scientia Publishers. 2(2):1-7. DOI: 10.59657/2993-5776.brs.24.021
Copyright: © 2024 Shanti Lal Choubisa, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 02, 2024 | Accepted: May 18, 2024 | Published: May 23, 2024
Abstract
Fluorosis is endemic in areas where people drink water containing fluoride above the recommended standard of 1.0 ppm or 1.5 ppm and/or people who are exposed to air-borne fluoride or any other fluoride sources for long periods of time. In this disease, primarily the teeth and bones are affected to varying degrees, depending on the fluoride level and its duration and frequency of exposure. Whatever the case, fluorosis primarily manifests as dental fluorosis and skeletal fluorosis. The latter form develops when fluoride accumulates excessively on various bones of the skeleton and is extremely painful. Actually, skeletal fluorosis is a bone disease caused by excessive accumulation of fluoride which causes the bones to become weak. In advanced state, skeletal fluorosis causes painful damage to the bones and joints and is extremely painful. In this disease the bones become harder and less flexible, resulting in increased frequency of fractures. Thickening of the bone structure and accumulation of bone tissue, both of which contribute to decreased joint mobility. Ligaments and cartilage can become ossified. Skeletal fluorosis is of utmost importance as it reduces mobility at a very early age by causing gradual changes in the bones such as periosteal exostosis, osteosclerosis, osteoporosis, and osteophytosis. These changes manifest clinically as vague pain in the body and joints. Excess accumulation of fluoride in the muscles also reduces mobility and the condition leads to disability or crippling. In its advanced stage, neurological complications such as paraplegia and quadriplegia and limbs deformities, such as genu-varum (outward bowing of legs at the knee) and genu-valgum (inward bowing of legs at the knee) syndromes also result from regular excessive fluoride accumulation in the bones and is the worst form of skeletal fluorosis. Once skeletal fluorosis develops it lasts a lifetime and is not curable. The presented editorial focuses on how skeletal fluorosis is dangerous and how it can be prevented in the humans. The purpose of this editorial is to provide scientific information and create awareness about this fluorosis disease among people living in fluoride endemic areas.
Keywords: bio-accumulation; bone deformities; drinking water; fluoride; industrial fluoride pollution; skeletal fluorosis; toxicosis; prevention
Introduction
It is well known that fluoride is universally found at varying levels in water, soil, air and foods. This may be due to geologic processes and/or anthropogenic or industrial activities. Fluoride intake has both beneficial and negative effects in humans that depend on the concentration of fluoride. Consumption of water containing fluoride in the range of 0.5 to 1.0 ppm is beneficial and reduces the chances and incidence of dental caries [1,2], but its excessive intake through drinking water contains fluoride more than the recommended or standard value of 1.0 ppm or 1.5 ppm then it leads to genesis of dangerous and highly painful fluorosis disease [3-5]. Globally, water-borne fluorosis (hydrofluorosis) is the most common and widespread disease in humans [3]. But industrial fluorosis is limited to specific areas or regions due to exposure to fluoride emitted from various industrial activities [6,7]. Fluorosis occurs not only in humans [8–22] but also in herbivorous wild [23–29] and domestic animals [30–55] if they are exposed to fluoride for long periods of time.
Once fluoride enters the body it is absorbed by the digestive and/or respiratory tract and then eventually reaches all parts of the body through the blood. More than 50% of the absorbed fluoride is excreted through feces, urine, and sweat, while the rest is retained in the body where it is deposited in various organs. However, its maximum accumulation is found in calcified organs, bones and teeth compared to non-calcified organs. Bio-accumulation of fluoride causes diverse toxic effects or pathological changes and interference with various physiological and metabolic processes and ultimately triggers the occurrence of adverse reversible and non-reversible health effects in people of all age groups. This fluoride induced toxic or health changes are collectively called fluorosis [3-5]. Various fluoride induced anomalies or deformities in teeth and bones are permanent, irreversible and not curable and can be easily observed. But fluoride-induced changes in soft tissues or organs are mostly reversible and disappear when the source of fluoride exposure is removed. Chronic fluoride exposure through ingestion of drinking water containing high fluoride levels (>1.0 or 1.5 ppm) can lead to three forms of fluorosis in man and animals, dental fluorosis (dental mottling), skeletal fluorosis (bone deformities) and non-skeletal Fluorosis [56,57]. But it is not necessary that all these three forms exist in the same person. However, among the various forms of fluorosis, skeletal fluorosis is a relatively more dangerous and highly painful bone disease in both humans and animals [56,57].
Dangerous skeletal fluorosis
Excessive fluoride intake or fluoride bioaccumulation alters the balance between bone formation and resorption. This physiological process is accomplished with the participation of certain regulatory determinants and signaling pathways, leading to various bone malformations (lesions) known as skeletal fluorosis. Severity and different phases of skeletal fluorosis is much depending on the amount of fluoride accumulation in bones (mg F/kg). There will be no changes in bones at bone ash fluoride concentrations of 500 to 1,000 mg F/kg. Above this range, various signs and symptoms of bone changes or deformities in various clinical phases are shown in Table 1 [58]. This entity of chronic fluoride intoxication or skeletal fluorosis is very painful and more dangerous than other forms of fluorosis and is of utmost importance because it reduces mobility at a very early age by causing gradual changes in the bones such as periosteal exostosis, osteoporosis, osteoporosis, and osteophytosis (Figure 1) [59-61]. These changes manifest clinically as vague pain in the body and joints. Excessive accumulation of fluoride in muscles also reduces mobility and the condition leads to disability or crippling (Figure 2). In its advanced stage, neurological complications such as paraplegia and quadriplegia and syndromes of genu-valgum and genu-varum also result from regular fluoride exposure and is the worst form of skeletal fluorosis.
Table 1: Various clinical phases and symptoms and signs of skeletal fluorosis at different range of bone ash fluoride concentration. Source: [58].
| Osteosclerotic phase | Bone ash fluoride concentration (mgF/kg) | Symptoms and signs |
| Normal Bone | 500 to 1,000 | Normal |
| Preclinical Phase | 3,500 to 5,500 | Asymptomatic; slight radiographically-detectable increases in bone mass |
| Clinical Phase I | 6,000 to 7,000 | Sporadic pain; stiffness of joints; osteosclerosis of pelvis and vertebral column |
| Clinical Phase Il |
7,500 to 9,000 | Chronic joint pain; arthritic symptoms; slight calcification of ligaments; increased osteosclerosis and cancellous bones; with/without osteoporosis of long bones |
| Clinical Phase Ill | 8,400 | Limitation of joint movement; calcification of ligaments of neck vertebral column; crippling deformities of the spine and major joints; muscle wasting; neurological defects/compression of spinal cord |
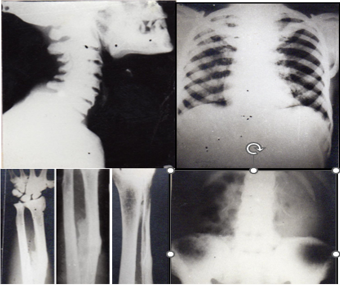
Figure 1: Radiographs of different bones of subjects, afflicted with skeletal fluorosis. Cervical and dorsal spines showing extreme osteosclerosis, lipping and osteophytosis (a, e); osteosclerosis of the pelvis with calcification of ligaments (e); contrast of the osteosclerosis in bony cage with radiolucent lungs and clavicular involvement (b); calcification of interosseous membrane (arrow) between radius and ulna bones of forearm (c); bony exostosis in tibia (d). The calcification of interosseous membrane (arrow) is the most ideal and confirmative indication of skeletal fluorosis.

Figure 2: Subjects afflicted with severe skeletal fluorosis characterised with invalidism, kyphosis, genu-varum (a, b, d, e), genu-valgum (c), crippling with paraplegia and quadriplegia (a, d), and crossing or scissor-shaped legs (e).
These fluoride-induced bone changes can appear in people of any age. However, children are more sensitive to changes in these bones. Interestingly, all these bone deformities or changes in humans persist throughout their life span and cannot be corrected by any treatment. Many people with skeletal fluorosis in rural areas are unable to perform daily tasks and have higher rates of bone fractures. Women may also face problems in delivery due to skeletal fluorosis. The severity of skeletal fluorosis depends not only on the fluoride concentration and its duration and frequency of exposure, but also on gender, food, nutrients, chemicals in the water, individual fluoride sensitivity or tolerance and genetics, environmental factors, etc. [62-72]. Whatever the case, disability, neurological complications (paraplegia and quadriplegia) and limb deformities, such as genu-varum (outward bowing of legs at the knee) and genu-valgum (inward bowing of legs at the knee) syndromes are found to be extremely painful and not treatable and may persist throughout life in subjects suffering from severe skeletal fluorosis.
Prevention of skeletal fluorosis
It is well documented that all types of fluoride induced bone deformities (crippling, neurological complications, limbs deformities, etc.) are irreversible and not curable. But their further progress or severity in people can be prevented or controlled by adopting and implementing the following potentially effective and feasible methods: (a) regular supply or providing of fluoride free treated drinking water, (b) control of entry of fluoride in the body from different sources such air-borne fluoride (industrial fluoride emissions) and various food items, such as alcohol, tea, rock salt, tobacco, and betel nuts, which naturally contain high amounts of fluoride, (c) providing nutritious foods containing ample amount of calcium, vitamin C, vitamin E nutrients, and antioxidants, and (d) to disseminate current knowledge about fluorosis and create general awareness among people towards preventive measures of fluoride poisoning with the help of well-trained volunteers, students, and teachers [3].
Defluoridation technology can be used or adopted for regular supply of fluoride free drinking water in the community or population inhabiting fluoride endemic areas. However, several defluoridation techniques have been developed that are readily available [73,74]. However, among these techniques, “Nalgonda Defluoridation Technique” is an ideal technique as it is simple, effective, and low cost which can be used at both household and community levels [75,76]. In India, where hydro fluorosis disease is endemic in almost all rural areas, this Nalgonda technique is most successful in the prevention and control of hydro fluorosis disease. However, this technique is cheap and gives good results but its success rate at the community level is poor due to lack of public participation, lack of responsibility for its supervision and lack of proper monitoring and maintenance [76]. Instead of adopting any defluoridation technique, the author believes that harvesting and conservation of rainwater is a better option to get low fluoride or fluoride free water regularly. Perennial freshwater reservoirs also allow regular supply of fluoride-free water to the community as their water contains only trace amounts of fluoride [3]. Nevertheless, collective efforts are needed to control fluorosis, while monitoring and evaluation of fluorosis control projects also needs to be done honestly.
Conclusion
Long-term exposure to fluoride or excessive intake of fluoride through drinking water and industrial fluoride emissions causes serious fluorosis disease which can develop in all age groups, children, adolescents, adults, and older people. Even low levels of fluoride can also develop fluorosis in humans. This disease is endemic in many countries, especially in their rural areas. Among the various forms of fluorosis, skeletal fluorosis is the most dangerous and highly painful. Excessive bioaccumulation of fluoride in bones leads to the development of various bone deformities, such as disability, neurological complications (paraplegia and quadriplegia) and limb deformities, and they persist throughout life and they are also irreversible or incurable. This state is the worst form of skeletal fluorosis. Thousands of people in rural areas of many fluorides endemic countries suffer from this bone disease. Prevention is the only cure or solution to this dreadful disease. Prevention of this disease in human population is possible by providing regular supply or availability of fluoride free drinking water, checking the entry of fluoride into the body, providing nutritious food, and spreading current knowledge about fluorosis and creating awareness among people about preventive measures.
Declarations
Funding sources
No any funding sources for this work.
Acknowledgements
The author thanks to Prof. Darshana Choubisa, Department Prosthodontics and Crown & Bridge, Geetanjali Dental and Research Institute, Udaipur, Rajasthan 313002, India for their cooperation.
References
- Petersen PE, Ogawa H. (2016). Prevention of dental caries through the use of fluoride-the WHO approach. Commun Dent Health, 33:66-68.
Publisher | Google Scholor - Pollick H. (2018). The role of fluoride in the prevention of tooth decay. Pediat Clinic North America, 65(5):923-940.
Publisher | Google Scholor - Adler P, Armstrong WD, Bell ME, Bhussry BR, Büttner W. et al. (1970). Fluorides and human health. World Health Organization Monograph Series No. 59. Geneva: World Health Organization.
Publisher | Google Scholor - Choubisa SL. (2023). Is drinking groundwater in India safe for human health in terms of fluoride? J Biomed Res, 4(1): 64-71.
Publisher | Google Scholor - Choubisa SL, Choubisa D, Choubisa A. (2023). Can people get fluorosis from drinking water from surface water sources? Fluoride test of water mandatory before its supply. SciBase Epidemiol Public Health, 1(2):1006.
Publisher | Google Scholor - Choubisa SL, Choubisa D. (2015). Neighbourhood fluorosis in people residing in the vicinity of superphosphate fertilizer plants near Udaipur city of Rajasthan (India). Environ Monit Assess, 187(8):497.
Publisher | Google Scholor - Choubisa SL, Choubisa D. (2016). Status of industrial fluoride pollution and its diverse adverse health effects in man and domestic animals in India. Environ Sci Pollut Res, 23(8): 7244-7254.
Publisher | Google Scholor - Choubisa SL, Sompura K, Bhatt SK, Choubisa DK, Pandya H, Joshi SC, et al. (1996). Prevalence of fluorosis in some villages of Dungarpur district of Rajasthan. Indian J Environ Health, 38(2):119-126.
Publisher | Google Scholor - Choubisa SL, Verma R. (1996). Skeletal fluorosis in bone injury case. J Environ Biol, 17(1):17-20.
Publisher | Google Scholor - Choubisa SL, Sompura K. (1996). Dental fluorosis in tribal villages of Dungarpur district (Rajasthan). Poll Res, 15(1):45-47.
Publisher | Google Scholor - Choubisa SL, Choubisa DK, Joshi SC, Choubisa L. (1997). Fluorosis in some tribal villages of Dungarpur district of Rajasthan, India. Fluoride, 30(4):223-228.
Publisher | Google Scholor - Choubisa SL. (1997). Fluoride distribution and fluorosis in some villages of Banswara district of Rajasthan. Indian J Environ Health, 39(4):281-288.
Publisher | Google Scholor - Choubisa SL. (1998). Fluorosis in some tribal villages of Udaipur district (Rajasthan). J Environ Biol, 19(4): 341-352.
Publisher | Google Scholor - Choubisa SL. (1999). Chronic fluoride intoxication (fluorosis) in tribes and their domestic animals. Intl J Environ Stud, 56(5): 703-716.
Publisher | Google Scholor - Choubisa SL. (2001). Endemic fluorosis in southern Rajasthan (India). Fluoride, 34(1):61-70.
Publisher | Google Scholor - Choubisa SL, Choubisa L, Choubisa DK. (2001). Endemic fluorosis in Rajasthan. Indian J Environ Health, 43(4):177-189.
Publisher | Google Scholor - Choubisa SL. (2012). Fluoride in drinking water and its toxicosis in tribals, Rajasthan, India. Proc Natl Acad Sci, India Sect B: Biol Sci, 82(2):325-330.
Publisher | Google Scholor - Choubisa SL. (2018). A brief and critical review of endemic hydrofluorosis in Rajasthan, India. Fluoride, 51(1):13-33.
Publisher | Google Scholor - Choubisa SL, Choubisa D. (2019). Genu-valgum (knock-knee) syndrome in fluorosis- endemic Rajasthan and its current status in India. Fluoride, 52(2):161-168.
Publisher | Google Scholor - Choubisa SL. (2022). The diagnosis and prevention of fluorosis in humans (editorial). J Biomed Res Environ Sci, 3(3):264-267.
Publisher | Google Scholor - Choubisa SL. (2022). Status of chronic fluoride exposure and its adverse health consequences in the tribal people of the scheduled area of Rajasthan, India. Fluoride, 55(1): 8-30.
Publisher | Google Scholor - Choubisa SL, Choubisa D, Choubisa A. (2023). Fluoride contamination of groundwater and its threat to health of villagers and their domestic animals and agriculture crops in rural Rajasthan, India. Environ Geochem Health, 45:607-628.
Publisher | Google Scholor - Shupe JL, Olson AE, Sharma R.P. (1972). Effects of fluoride in domestic and wild animals. Clinic Toxicol, 5(2): 195-213.
Publisher | Google Scholor - Shupe JL, Olson AE, Peterson HB, Low JB. (1984). Fluoride toxicosis in wild ungulates. J Ame Vet Med Assoc, 185(11):1295-1300.
Publisher | Google Scholor - Suttie JW, Hamilton RJ, Clay AC, Tobin ML, Moore WG. (1985). Effects of fluoride ingestion on white-tailed deer (Odocoileus virginianus). J Wildlife Dis, 21(3):283-288.
Publisher | Google Scholor - Van PM, Dierick N, Janssens G, Fievez V, De Smet S. (2010). Selected trace and ultratrace elements: Biological role, content in feed and requirements in animal nutrition – Elements for risk assessment. EFSA Support Public, 7(7):68E.
Publisher | Google Scholor - Kierdorf U, Death C, Hufschmid J, Witzel C, Kierdorf H. (2016). Developmental and post-eruptive defects in molar enamel of free-ranging eastern grey kangaroos (Macropus giganteus) exposed to high environmental levels of fluoride. PLoS One, 11(2): e0147427.
Publisher | Google Scholor - Kierdorf U, Kierdorf H, Sedlacek F, Fejerskov O. (1996). Structural changes in fluorosed dental enamel of red deer (Cervus elaphus L.) from a region with severe environmental pollution by fluorides. J Anat, 188(1):183-195.
Publisher | Google Scholor - Choubisa SL. (2024). Can fluoride exposure be dangerous to the health of wildlife? If so, how can they be protected from it? J Vet Med Animal Sci, 7(1):1-6,1144.
Publisher | Google Scholor - Choubisa SL, Pandya H, Choubisa DK, Sharma OP, Bhatt SK. et.al. (1996). Osteo-dental fluorosis in bovines of tribal region in Dungarpur (Rajasthan). J Environ Biol, 17(2):85-92.
Publisher | Google Scholor - Choubisa SL. (1996). An epidemiological study on endemic fluorosis in tribal areas of southern Rajasthan. A technical report. The Ministry of Environment and Forests, Government of India, New Delhi, pp 1-84.
Publisher | Google Scholor - Choubisa SL. (1999). Some observations on endemic fluorosis in domestic animals of southern Rajasthan (India). Vet Res Commun, 23(7):457-465.
Publisher | Google Scholor - Choubisa SL. (2000). Fluoride toxicity in domestic animals in Southern Rajasthan. Pashudhan, 15(4):5.
Publisher | Google Scholor - Swarup D, Dwivedi SK. (2002). Environmental pollution and effect of lead and fluoride on animal health. New Delhi: Indian Council of Agricultural Research.
Publisher | Google Scholor - Choubisa SL. (2007). Fluoridated ground water and its toxic effects on domesticated animals residing in rural tribal areas of Rajasthan (India). Intl J Environ Stud, 64(2):151-159.
Publisher | Google Scholor - Choubisa SL. (2008). Dental fluorosis in domestic animals. Curr Sci, 95(12):1674-1675.
Publisher | Google Scholor - Choubisa SL. (2010). Osteo-dental fluorosis in horses and donkeys of Rajasthan, India. Fluoride, 43(1):5-10.
Publisher | Google Scholor - Choubisa SL. (2010). Fluorosis in dromedary camels of Rajasthan, India. Fluoride, 43(3): 194-199.
Publisher | Google Scholor - Choubisa SL, Mishra GV, Sheikh Z, Bhardwaj B, Mali P. et.al. (2011). Toxic effects of fluoride in domestic animals. Adv Pharmacol Toxicol, 12(2):29-37.
Publisher | Google Scholor - Choubisa SL. (2012). Status of fluorosis in animals. Proc Natl Acad Sci, India Sect B: Biol Sci, 82(3):331-339.
Publisher | Google Scholor - Choubisa SL, Modasiya V, Bahura CK, Sheikh Z. (2012). Toxicity of fluoride in cattle of the Indian Thar Desert, Rajasthan, India. Fluoride, 45(4):371-376.
Publisher | Google Scholor - Choubisa SL, Mishra GV. (2013). Fluoride toxicosis in bovines and flocks of desert environment. Intl J Pharmacol Biol Sci, 7(3):35-40.
Publisher | Google Scholor - Choubisa SL. (2015). Industrial fluorosis in domestic goats (Capra hircus), Rajasthan, India. Fluoride, 48(2):105-115.
Publisher | Google Scholor - Choubisa SL. (2018). A brief and critical review on hydrofluorosis in diverse species of domestic animals in India. Environ Geochem Health, 40(1):99-114.
Publisher | Google Scholor - Choubisa SL. (2022). A brief and critical review of chronic fluoride poisoning (fluorosis) in domesticated water buffaloes (Bubalus bubalis) in India: focus on its impact on rural economy. J Biomed Res Environ Sci, 3(1):96-104.
Publisher | Google Scholor - Choubisa SL. (2022). A brief review of chronic fluoride toxicosis in the small ruminants, sheep and goats in India: focus on its adverse economic consequences. Fluoride, 55(4):296-310.
Publisher | Google Scholor - Choubisa SL. (2023). Endemic hydrofluorosis in cattle (Bos taurus) in India: an epitomised review. Int J Vet Sci Technol, 8(1):001-007.
Publisher | Google Scholor - Choubisa SL. (2023). Chronic fluoride poisoning in domestic equines, horses (Equus caballus) and donkeys (Equus asinus). J Biomed Res, 4(1):29-32.
Publisher | Google Scholor - Choubisa SL. (2023). A brief review of endemic fluorosis in dromedary camels (Camelus dromedarius) and focus on their fluoride susceptibility. Austin J Vet Sci & Anim Husb, 10(1):1-6, id 1117.
Publisher | Google Scholor - Choubisa SL. (2023). A brief and critical review of endemic fluorosis in domestic animals of scheduled area of Rajasthan, India: focus on its impact on tribal economy. Clinic Res Anim Sci, 3(1):1-11
Publisher | Google Scholor - Choubisa SL. (2023). Industrial fluoride emissions are dangerous to animal health, but most ranchers are unaware of it. Austin Environ Sci, 8(1):1-4, id 1089.
Publisher | Google Scholor - Choubisa SL. (2023). A brief review of industrial fluorosis in domesticated bovines in India: focus on its socio-economic impacts on livestock farmers. J Biomed Res, 4(1):8-15.
Publisher | Google Scholor - Choubisa SL. (2023). Is drinking groundwater in India safe for domestic animals with respect to fluoride? Arch Animal Husb & Dairy Sci, 2(4):1-7.
Publisher | Google Scholor - Choubisa SL. (2023). Is it safe for domesticated animals to drink fresh water in the context of fluoride poisoning? Clinic Res Anim Sci, 3(2):1-5.
Publisher | Google Scholor - Choubisa SL. (2024). Are bovine calves ideal bio-indicators for endemic fluorosis? J Vet Sci Res, Article ID: OAJVSR-ED-24-302 (In-press).
Publisher | Google Scholor - Choubisa SL. (2022). The diagnosis and prevention of fluorosis in humans. J Biomed Res Environ Sci, 3(3):264-267.
Publisher | Google Scholor - Choubisa SL. (2022). How can fluorosis in animals be diagnosed and prevented? Austin J Vet Sci Anim Husb, 9(3):1-5.
Publisher | Google Scholor - Review of fluoride benefits and risks: report of the Ad Hoc Subcommittee on Fluoride of the Committee to Coordinate Environmental Health and Related Programs. Washington, D.C.: Public Health Service, Department of Health and Human Services, 1991.
Publisher | Google Scholor - Choubisa SL. (1996). Radiological skeletal changes due to chronic fluoride intoxication in Udaipur district (Rajasthan). Poll Res, 15(3):227-229.
Publisher | Google Scholor - Choubisa SL. (2012). Toxic effects of fluoride on bones. Adv Pharmacol Toxicol, 13(1):9-13.
Publisher | Google Scholor - Choubisa SL. (2022). Radiological findings more important and reliable in the diagnosis of skeletal fluorosis. Austin Med Sci, 7(2):1-4, id1069.
Publisher | Google Scholor - Choubisa SL, Choubisa L, Choubisa D. (2009). Osteo-dental fluorosis in relation to nutritional status, living habits and occupation in rural areas of Rajasthan, India. Fluoride, 42(3):210-215.
Publisher | Google Scholor - Choubisa SL, Choubisa L, Choubisa D. (2010). Osteo-dental fluorosis in relation to age and sex in tribal districts of Rajasthan, India. J Environ Sci Engg, 52(3):199-204.
Publisher | Google Scholor - Choubisa SL. (2010). Natural amelioration of fluoride toxicity (fluorosis) in goats and sheep. Curr Sci, 99(10):1331-1332.
Publisher | Google Scholor - Choubisa SL, Choubisa L, Choubisa D. (2011). Reversibility of natural dental fluorosis. Intl J Pharmacol Biol Sci, 5(20):89-93.
Publisher | Google Scholor - Choubisa SL, Mishra GV, Sheikh Z, Bhardwaj B, Mali P. et.al. (2011). Food, fluoride, and fluorosis in domestic ruminants in the Dungarpur district of Rajasthan, India. Fluoride, 44(2):70-76.
Publisher | Google Scholor - Choubisa SL. (2012). Osteo-dental fluorosis in relation to chemical constituents of drinking waters. J Environ Sci Engg, 54(1):153-158.
Publisher | Google Scholor - Choubisa SL. (2013). Why desert camels are least afflicted with osteo-dental fluorosis? Curr Sci, 105(12):1671-1672.
Publisher | Google Scholor - Choubisa SL, Choubisa A. (2021). A brief review of ideal bio-indicators, bio-markers and determinants of endemic of fluoride and fluorosis. J Biomed Res Environ Sci, 2(10):920-925.
Publisher | Google Scholor - Choubisa SL, Choubisa D, Choubisa P. (2023). Are tribal people in India relatively more susceptible to fluorosis? More research is needed on this. Poll Commun Health Effect, 1(2): 1-10.
Publisher | Google Scholor - Choubisa SL. (2024). Are sheep and goat animals relatively more tolerant to fluorosis? J Vet Med Res, 11(1): 1-5,1261.
Publisher | Google Scholor - Choubisa SL. (2024). Is the water buffalo species (Bubalus bubalis) relatively more sensitive to fluorosis than other species of domestic animals? Still, there is a need for more in-depth research on this. J Vet Med Animal Sci, 7(1):1-6,1139.
Publisher | Google Scholor - Ayoob S, Gupta AK, Bhat VT. (2008). A conceptual overview on sustainable technologies for the defluoridation of drinking water, critical reviews. Environ Sci Technol, 38(6):401-470.
Publisher | Google Scholor - Jamwal KD, Slathia D. (2022). A review of defluoridation techniques of global and Indian prominence. Curr World Environ, 17(1):41-57.
Publisher | Google Scholor - Nawlakhe WG, Paramasivam R. (1993). Defluoridation of potable water by Nalgonda technique. Curr Sci, 65:743-748.
Publisher | Google Scholor - Choubisa SL. (2023). Nalgonda technique is an ideal technique for defluoridation of water: its use can prevent and control hydrofluorosis in humans in India. Acad J Hydrol & Water Resourc, 1(1):15-21.
Publisher | Google Scholor




















