

Case Report
Extremely Rare Frontal, Temporal and Parietal Giant Cerebral Hydatid Cyst Causing None Communicating Hydrocephalus: A Case Report
1Department of Surgery, School of Medicine, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia.
2Life care Hospital, Kenya.
*Corresponding Author: Tigabu Daniel, Department of Surgery, School of Medicine, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia.
Citation: Daniel T, Woldegiorgis T. (2024). Extremely Rare Frontal, Temporal and Parietal Giant Cerebral Hydatid Cyst Causing None Communicating Hydrocephalus: A Case Report, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 1(6):1-4. DOI: 10.59657/2997-6103.brs.24.030
Copyright: © 2024 Tigabu Daniel, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 28, 2024 | Accepted: October 25, 2024 | Published: November 01, 2024
Abstract
Introduction: Hydatid disease is an animal illness that has been accidentally transmitted to humans. Humans become infected after consuming contaminated water or food, or via direct contact with canine feces. It is unusual to discover intracranial echynococosis. The therapy for an intracranial hydatid cyst is to perform a craniotomy and deliver the cyst intact, with concurrent pre- and post-operative albendazole medication.
Case Report: An eight-year-old child of Sidama ethnicity presented with a change in mentation and one week of projectile vomiting. She has left-extremity weakness, seizures, and a history of dog interaction. She was diagnosed with intracranial cerebral hydatid multiple cysts on the left cerebrum, which causes none communicating hydrocephalus. She was given oral albendazole, and an emergency base left craniotomy was performed, removing several cysts, daughter cysts, and some adhesions as intact cysts without rupture. Except for the power, all circumstances have improved dramatically. She was discharged with oral phenytoin, albendazole, and an appointment.
Conclusion: Intracranial hydatid cysts, notably frontal, temporal, and parietal, were highly unusual to occur. The mainstay of treatment is surgically removing a whole intact cyst and administering albendazole both before and after surgery.
Keywords: intracranial hydatid cyst; hydrocephalus; albendazole
Introduction
Background: hydatid disease is an animal illness that accidentally affects human beings [1]. Hydatid cysts have a life cycle that involves both herbivores and canines [1,2]. Humans become infected after consuming dog feces-contaminated water or food [1-3]. Hydatid infection is prevalent in pastors because to direct contact with dogs and ingestion of echynococcal eggs, which hatch in the gastro-intestinal tract and go to the liver via enterohepatic circulation, where the parasite is usually lodged. The most typically afflicted bodily part is the liver, followed by the lungs. Intracranial echynococosis is extremely uncommon [3,4].
Intracranial hydatid illness develops when it moves from the liver, lung, and heart to the skull. Although its clinical characteristics vary depending on the portion of the body affected, it often takes decades to grow to a bigger size and produce symptoms. Cerebral echynococcosis is uncommon, and the clinical presentation is similar to that of other cerebral space-occupying lesions, resulting in mass effect and nonspecific weight loss, anorexia, and cachexia. medication for cerebral hydatid cyst involves conducting craniotomy and delivering intact cyst totally with concurrent pre- and post-operative albendazole medication [2,5].
Case Report
A female Sidama ethnicity patient, aged 8, arrived with a week-long change in mentation and projectile vomiting. She has had generalized tonic-clonic abnormal body movement for five months. She has also experienced left side extremities weakness over the last two years, as well as considerable yet unquantifiable weight loss. She experienced anorexia, but no other gastrointestinal problems. She frequently had direct contact with her dog at home.
On physical examination, she had normal vital signs, head and neck examination, chest, cardiovascular, abdominal, and other system exams. On neurologic examination: GCS-13/15 (eye-opening 4, verbal 3, and motor 6), pupil-left dilated and fixed but right constricted and reactive, power on lower extremity bilaterally 3/5 but 5/5 upper extremities bilaterally, spastic.
CBC, serum electrolyte, coagulation profile, and organ function tests all came back normal. Chest x-rays and abdomen ultrasounds were also normal. A brain MRI revealed a massive intra-axial left cerebral hemisphere hydatid cyst affecting the left frontal, temporal, and parietal lobes of the brain parenchyma, as well as several daughter cysts. It has had a widespread impact (Figure 1).
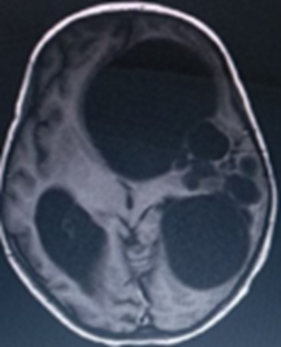
Figure 1: Multiple Cysts Causing Mass Effect.
The patient was then given albendazole for three days before undergoing an emergency craniotomy due to elevated intracranial pressure. Intraoperative examinations revealed many typical hydatid cysts with daughter cysts inside, as well as effaced bilateral ventricles. The cysts were removed whole, together with their daughter cysts, and hemostasis was achieved. The bone returned and the scalp closed, and the patient was transferred to the critical care unit intubated (ICU), was in good postoperative condition.
She was extubated and doing well on the third day after being admitted to the ICU. Her vital signs are within normal limits, and her pupils have become reactive and normal size bilaterally. Her GCS has increased to 15/15, but her lower extremity power is still 3/5 bilaterally, and she has no seizure history. Her post-operative recovery is now going well. She was discharged on oral phenytoin and albendazole and is on follow-up.

Figure 2: Multiple Hydatid Cyst Removed Intact and Adhesive Tissues.
Discussion
Hydatid disease is animal disease that affects human being accidentally [1-15]. The lifecycle of hydatid cyst is between herbivores and canines [1,2]. Humans become infected after consuming dog feces-contaminated water or food [1-3]. Hydatid infection is widespread in pastoralists due to direct contact with dogs and the ingestion of echynococcal eggs, which hatch in the gastrointestinal tract and travel to the liver via enterohepatic circulation, where the parasite is usually lodged.
The most commonly damaged bodily parts are the liver and the lungs. It is uncommon to encounter intracranial echynococosis [3,4]. Intracranial hydatid disease develops when it goes through the liver, lung, and heart before reaching the brain. Although its clinical characteristics vary according on the portion of the body affected, it often takes decades to grow large enough to elicit symptoms. Intracranial echynococcosis is uncommon, and the clinical features are typically those of any intracranial space-occupying lesions, including mass effect and nonspecific weight loss, anorexia and cachexia [2,5]. The reported incidence of brain hydatid cyst was about 1.6–5.2% [10]. Like the case reported by Cindea et al., our patient suffered headache and vomiting, however contrary to this report, our patient had no visual loss [2]. Unlike our patient, Umerani et al. reported no lateralizing signs or vomiting [3].
Alok et al. reported similar case report like our patient who has lateralizing signs [4]. Akrim et al. reported secondary intracranial hydatid cyst (post-surgery), whereas ours which is primary kind [11]. Magoha et al reported nearly similar case regarding age of the patient, lateralizing sign, and duration of the head ache to our case report [13]. Un like report by Assefa et al. and case report from Addis Ababa, Ethiopia our patient has seizure [6,7]. Another study by Chen et al. found liver and lung hydatid with simultaneous brain hydatid cyst, which contradicts our result of primary brain hydatid cyst [8]. Like most case reports it is diagnosed by clinical features and imaging finding [1-15]. Unique to our case was extensively involving the whole hemisphere causing none communicating hydrocephalus.
Conclusion
Intracranial hydatid cysts, notably frontal, temporal, and parietal, were highly unusual to occur. The mainstay of treatment is surgically removing a whole intact cyst and administering albendazole both before and after surgery.
Declaration
Ethical Approval and Consent for Participation
Written informed consent for participation was obtained from the child mother and according to the Hawassa University IRB guideline, an IRB approval letter is not needed for publication of case reports.
Consent for Publication
Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing Interests
The authors report no conflicts of interest in this work.
Funding
There is no financial support.
Authors’ Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
My deepest gratitude goes to the patient family.
References
- Ganjeifar B, Ghafouri M, et al. (2021). Giant Cerebral Hydatid Cyst: A Rare Case Report. Clin Case Rep. 9(3):1774-1778.
Publisher | Google Scholor - Cindea CN, Saceleanu V, Saceleanu A. (2021). Intraoperative Rupture of an Intracranial, Extradural Hydatid Cyst: Case Report and Treatment Options. Brain Sci. 11(12):1604.
Publisher | Google Scholor - Umerani MS, Abbas A, Sharif S. (2013). Intra Cranial Hydatid Cyst: A Case Report of Total Cyst Extirpation and Review of Surgical Technique. J Neurosci Rural Pract. 4(Suppl 1):S125-S128.
Publisher | Google Scholor - Alok R, Mahmoud J. (2020). Successful Surgical Treatment of a Brain Stem Hydatid Cyst in a Child. Case Rep Surg. 5645812.
Publisher | Google Scholor - T. Todorov, K. Vutova, D. Petkov, G. Balkanski. (1988). Albendazole Treatment of Multiple Cerebral Hydatid Cysts: Case Report, Transactions of The Royal Society of Tropical Medicine and Hygiene, 82(1):150-152.
Publisher | Google Scholor - Assefa G, Biluts H, Abebe M, Birahanu MH, Ababa A. (2011). Cerebral Hydatidosis, A Rare Clinical Entity in Ethiopian Teaching Hospitals: Case Series and Literature Review. East and Central African Journal of Surgery. 16:123-129.
Publisher | Google Scholor - Arega G, Merga G, Tafa G, Salah FO, Abebe G, et al. (2022). Temporoparietal Brain Hydatid Cyst in an Eight-Year-Old Child: A Rare Case Report. Pediatric Health Med Ther. 13:361-365.
Publisher | Google Scholor - Chen S, Li N, Yang F, Wu J, Hu Y, et al. (2018). Medical treatment of an unusual cerebral hydatid disease, BMC Infectious Diseases. 12.
Publisher | Google Scholor - Singh, R.K., Patwa, P.A., Mishra, G.V. et al. (2022). An Unusual Case Report on Intracranial Hydatid Cyst with Intraventricular Extension. Egypt J Radiol Nucl Med, 53:52.
Publisher | Google Scholor - Kist S, Olgu H. (2024). Cerebral Hydatid Cyst: A Case Report. Turkish Journal of Neurology. 20(3):87-90.
Publisher | Google Scholor - Akrim Y, Barkate K, Arrad Y, Ghannane H, El Hakkouni A. (2022). Multiple Cerebral Hydatid Cysts: A Case Report. Cureus. 14(5):e25529.
Publisher | Google Scholor - Nashibi M, Tafrishinejad A, Hussain Khan Z. (2020). Deep Seated Cerebral Hydatid Cyst and Its Anesthetic Considerations: A Case Report. Arch Neurosci. 7(1):e100044.
Publisher | Google Scholor - M. A. Magoha, N. K. Mohan, C.K. Musau, M.P. Okemwa. (2016). Giant Solitary Cerebral Hydatid Cyst in A Child, Complicated with Post-Operative Subdural Haematoma: Case Report and Review of Literature. East African Medical Journal. 93(11):626-631.
Publisher | Google Scholor - Boujan, M.M.K, Jalal, Z.S.A. (2013). A Rare Case of Primary Multiple Hydatid Cysts of The Brain in A 10-Year-Old Child. Eastern Mediterranean Health Journal, 19(Supp.2):1-8.
Publisher | Google Scholor - Menschaert D, Daron A, Frere J. (2023). Case Report of Cerebral Cystic Echinococcosis in A 5-Year-Old Child. Front. Trop. Dis. 4:1090644.
Publisher | Google Scholor










