

Review Article
Evaluation of the Prevalence, Knowledge, Attitude, and Practice of Diabetes Mellitus among Adults in Famgbe Community
- Obele W. Philip 1
- Owonaro A. Peter 1*
- Eniojukan F. Joshua 1
- Owonaro E. Daugther 2
- Seiyefa F. Brisibe 2
- Igbegi S. Igbegi 2
1Niger delta university, wilberforce island bayelsa state., faculty of pharmacy, department of clinical pharmacy and pharmacy practice.
2Niger delta university, wilberforce island bayelsa state., faculty of clinical sciences, department of family medicine.
*Corresponding Author: Owonaro A. Peter,Niger delta university, wilberforce island bayelsa state., faculty of pharmacy, department of clinical pharmacy and pharmacy practice.
Citation: Philip O.W, Peter O.A, Joshua. E.F, Daugther. O.W, Brisibeand S.F, Igbegi I.S. (2024). Evaluation of the Prevalence, Knowledge, Attitude, and Practice of Diabetes Mellitus among Adults in Famgbe Community. International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 3(6):1-7. DOI: 10.59657/2837-8172.brs.24.067
Copyright: © 2024 Owonaro A. Peter, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 03, 2024 | Accepted: September 16, 2024 | Published: October 04, 2024
Abstract
Diabetes mellitus is a public health issue that has consequences of nephropathy, neuropathy, and retinopathy and should be researched and prevented, so in a bid to ascertain the prevalence, knowledge, attitude, and practices of diabetes mellitus in a rural area; Famgbe Community in Bayelsa State, Nigeria was selected and a descriptive cross-sectional survey was done in the community among persons aged 18 and above, using a self-administered questionnaire to 314 respondents. From the results of this study, 75.8% of respondents reported that they do not have any family history of diabetes, 45.5% reported that they knew the range for a normal blood sugar reading, and 62.8% of respondents reported that they never checked their blood sugar levels. The findings showed that more than half of the study population had a good awareness of diabetes a positive attitude toward the disease and appropriate practices towards the diseases.
Keywords: diabetes mellitus; nephropathy, neuropathy, retinopathy; blood sugar
Introduction
Diabetes mellitus (DM) is one of the leading causes of illness and mortality, with a considerable influence on patients' quality of life, productivity, and enormous health costs for almost every country (Kasper et al 2008). The global prevalence of type 2 diabetes is steadily increasing. This increase is linked to population expansion, economic development, aging populations, increased urbanization, dietary changes, obesity, decreased physical activity, and changes in other lifestyle habits (WHO, 2012). Diabetes accounts for one out of every twenty adult fatalities in underdeveloped nations, with Africa having the greatest mortality rate (Roglic 2000). The management of diabetes mellitus (DM) is heavily reliant on patients' ability to self-care in their daily lives; hence patient education is always regarded as a vital component of diabetes management. Studies have consistently shown that improved glycemic control reduces the rate of complications, and evidence suggests that patients who are knowledgeable about DM self-care have better long-term glycemic control (Norris 2001). It is therefore critical to ensure that patients' knowledge, attitudes, and practices are adequate. The majority of disease-related deaths and disabilities are caused by risk factors such as high blood pressure, tobacco use, alcohol consumption, physical inactivity, a poor diet, being overweight, or being obese. (WHO, 2012). Approximately 20 minutes of moderate physical activity per day can reduce the risk of diabetes by 27% while also helping to lose weight. (WHO, 2012). Patients can decrease and control known modifiable risk factors by obtaining effective education and understanding. Effective disease management, risk factor control, diagnosis, and preventative awareness are all linked to the knowledge, attitudes, and practices of diabetic patients (Damaio 2013, AL-Maskari 2013).
Previous research has also shown that persons living with diabetes who have high levels of knowledge and education take better care of themselves. Poor self-care knowledge can result in poor long-term metabolic management, leading to diabetic complications such as retinopathy, nephropathy, neuropathy, and atherosclerotic alterations. As a result, patients require instruction on a variety of self-care topics, ranging from general lifestyle recommendations to knowledge of prescribed medications. Because of its importance, the American Diabetes Association recommends a yearly assessment of patients' skills and knowledge. There is a small but growing body of literature on KAP concerning diabetes among newly diagnosed type 2 diabetic patients in Nigeria; such studies are important for creating methods for disease control and prevention in a resource-poor situation common in many developing nations.The researcher places significant study on the needs of the residents in the Famgbe community (rural area), to adopt and practice common public health initiatives to prevent diabetes such as: eating healthy, exercising regularly, avoiding smoking, avoiding drinking alcohol, checking their blood sugar regularly, detection of signs and symptoms of the disease, promoting good health, and health education. The purpose of this study was to assess the prevalence, knowledge, attitude, and practice of diabetes in Famgbe Community in Bayelsa State, Nigeria.
Research Methodology
Study site
The study area was Famgbe community situated in the Attisa clan in Yenagoa local government area of Bayelsa State, Nigeria.
Study design
A prospective descriptive cross-sectional design was used in this study.
Sampling technique
Convenience sampling was used to choose the community as an area of study. A simple random sampling (lucky dip) was used to select the participants.
Data collection
A semi-structured self-report questionnaire was adapted from (Nurul, et. al., 2014 and Ifeoluwa, 2019). A pilot study was carried out, after which the questionnaire was modified to suit the target population.
Data analysis
IBM SPSS version 27 and Microsoft Excel (Ver. 2013), descriptive statistics such as frequency and mean values were used to present data and further expressed in charts.
Ethical issues
Approval for this study was obtained from the Bayelsa State Ministry of Health.
Results
Demography of study participants
Age of respondents
The majority of respondents were young adults aged 18-25 years (29%).
Results
Demography of study participants
Age of respondents
The majority of respondents were young adults aged 18-25 years (29%).
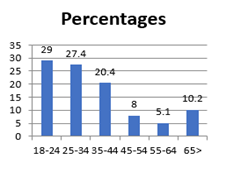
Figure 1: Age of participants
Gender of participants
Over 50% of the respondents were female.
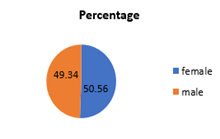
Figure 2: Gender of participants
Marital status of respondents
Single were the majority for marital status with 43.3%
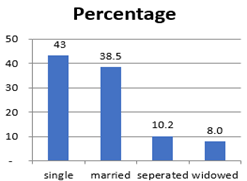
Figure 3: Marital status of participants
Educational status respondents
Persons with secondary school qualifications formed the majority of respondents with 65%.
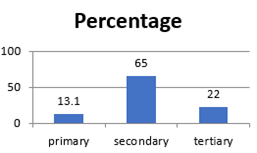
Figure 4: Educational status of respondents
Table 1: Prevalence of diabetes
| S/N | Variables | Yes | No N (%) | Not Sure N (%) |
| 1 | Do you have high blood sugar levels (diabetes)? | N (%) | 244(77.7) | 22(12.7) |
| 2 | Do you have a family history of diabetes? | 30(9.6) | 238(75.8) | 44(14.0) |
| 3 | Have any of your relations died as a result of diabetes? | 32(10.2) | 240(76.4) | 42(13.4) |
| 4 | Are you currently on any anti-diabetic drugs? | 28(93.3) | 2(6.7) | - |
| 5 | 8. Have you ever been admitted to the hospital because of diabetes? | 24(80) | 6(20) | - |
| 6 | Do you have wounds that are not healing? | 3(10) | 27(90) | 0(0) |
| 7 | When were you diagnosed to be diabetic (years)? | 0 -5 | 6-10 | 10> |
| 20(66.7) | 4(13.3) | 6(20.0) | ||
| 8 | What type of diabetes do you have? | Type1 | 06_10 | Not Sure |
| 0(0) | 4(13.3) | 11(36.7) | ||
| 9 | Is your vision currently affected? | Always | Type2 | Never |
| 18(60) | 19(63.3) | 0(0) | ||
| 10 | Do your legs swell sometimes? | 7(24.1) | Sometimes | 0(0) |
| 11 | Which of your family is/are affected? | Father | 12(40) | |
| Mother | 22(75.9) | |||
| Brother | 3(10.2) | |||
| Sister | 5(17.2) | |||
| Uncle | 6(20.7) | |||
| Aunty | 4(13.8) |
Over 70% of respondents reported that they were not diabetic, and 75.8% of respondents reported that they do not have any family history of diabetes.
Table 2: Knowledge regarding diabetes
| S/N | Variable | Yes N(%) | No N(%) | I don’t know N(%) |
| 1 | Do you know what high blood sugar is? | 213(67.8) | 25(8.0) | 76(24.2) |
| 2 | Do you know the normal reading of blood sugar levels? | 143(45.5) | 67(21.3) | 104(33.1) |
| 3 | Do you know what complications can arise if high blood sugar is not controlled? | 170(54.1) | 40(12.8) | 104(3.1) |
| 4 | Will excessive alcohol intake increase your risk of having high blood sugar? | 191(60.8) | 57(18.2) | 66(21.0) |
| 5 | Do you know high blood sugar is of many types? | 161(51.6) | 78(24.5) | 75(23.9) |
| 6 | Is being overweight one of the risk factors for developing high blood sugar? | 254(80.9) | 17(5.4) | 43(13.7) |
| 7 | Do you know the signs and symptoms of high blood sugar? | 255(81.2) | 18(5.7) | 41(13.1) |
| 8 | Do you know the signs and symptoms of low blood sugar? | 168(53.5) | 60(19.1) | 86(27.4) |
| 9 | Do you know that those with high blood sugar take drugs every day? | 260(82.8) | 20(6.4) | 34(10.8) |
| 10 | Is a regular blood sugar check necessary for high blood sugar patients? | 264(84.0) | 14(4.5) | 4(11.5) |
| Total | 2079 | 396 | 665 | |
| Mean (%) | 207.9(66.2) | 39.6 (12.6) | 66.5(21.2) |
Over 40% of respondents reported that they knew the range for a normal blood sugar reading, over 80% reported that being obese is a risk factor for becoming diabetic, and 81.2% of respondents reported that they knew the signs and symptoms of hyperglycemia.
Table 3: Attitudes towards diabetes
| S/N | Variables | SA N(%) | A N(%) | N N(%) | SDA N(%) | DA N(%) |
| 1 | Reduction of food high in fat and sugar prevents high blood sugar. | 158(50.3) | 51(16.2) | 77(24.5) | 6(1.9) | 22(7.0) |
| 2 | Regular checking of blood sugar is important. | 219(69.7) | 76(24.2) | 15(4.8) | 1(0.3) | 3(1.0) |
| 3 | Regular visits to the hospital or healthcare center are good for control of blood sugar. | 218(69.4) | 74(23.6) | 12(3.8) | 2(0.6) | 8(2.5) |
| 4 | Regular medication is important in blood sugar treatment. | 223(71.0) | 72(22.9) | 16(5.1) | 0(0) | 3(1.0) |
| 5 | People with diabetes should exercise daily | 221(70.8) | 74(23.2) | 16(5.1) | 0(0) | 3(1.0) |
| 6 | Regular Coke intake is good for someone with a high sugar level | 17(5.4) | 32(10.2) | 36(11.5) | 123(39.2) | 106(33.8) |
| 7 | Diabetes can be cured. | 17(5.4) | 32(10.2) | 36(11.5) | 122(39.1) | 107(33.9) |
| 8 | Diabetes can be inherited from the parents. | 223(71) | 72(22.9) | 16 (5.1) | 0(0) | 3(1.0) |
| 9 | Diabetes can be contracted through sex. | 2(0.6) | 8(2.5) | 15(4.8) | 138(43.9) | 151(48.1) |
| 10 | Diabetes can kill if not properly managed. | 222(70.9) | 73(23) | 16(5.1) | 0(0) | 3(1.0) |
| 11 | Diabetes can be contracted by sharing eating utensils. | 2(0.6) | 7(2.2) | 16(5.1) | 132(42.0) | 157(50) |
| 12 | Diabetes can be contracted through mosquito bites. | 3(1) | 10(3.2) | 13(4.1) | 132(42) | 156(49.7) |
| Total | 227 | 90 | 45 | 264 | 316 | |
| Mean (%) | 118.4(37.7) | 46.3(14.7) | 24.47.8) | 59.6(19.0) | 65.4(20.8) |
Over 90% of respondents agreed that adherence to medications is important in the management of diabetes, and over 90% agreed that checking blood sugar levels regularly is important.
Table 4: Practices regarding diabetes
| S/N | Variables | Always N (%) | Sometimes N (%) | Never N (%) |
| 1 | Do you check your blood sugar regularly? | 2(0.6) | 115(36.6) | 197(62.8) |
| 2 | Do you visit your healthcare provider regularly? | 33(10.5) | 181(57.6) | 100(31.8) |
| 3 | Do you eat food high in fat and sugar in your daily diet? | 29(9.2) | 254(80.9) | 31(9.9) |
| 4 | Do you drink soft drinks (coke, Fanta, and malt) a lot? | 28(8.9) | 255(81.2) | 31(9.9) |
| 5 | Do you eat late at night often? | 30(9.6) | 251(79.9) | 33(10.5) |
| 6 | Do you do intermittent fasting? | 27(8.6) | 249(79.3) | 38(12.1) |
| 7 | Do you monitor your weight? | 44(14) | 132(42) | 138(43.9) |
| 8 | Do you do exercises? | 44(14) | 132(42) | 138(43.9) |
| 9 | Do you smoke? | 23(7.3) | 31(9.9) | 260(82.8) |
| 10 | Do you drink alcohol? | 36(11.5) | 138(43.9) | 140(44.6) |
| 11 | Are You on Any Anti-Diabetic Drugs? | 238(75.8.7) | 76(24.2) | 0(0) |
| 12 | Do you have ready access to your drugs? | 283(90.1) | 31(9.9) | 0(0) |
| 13 | Do you take your drugs regularly? | 229(72.9) | 85(27.1) | 0(0) |
| 14 | Do you miss taking your drugs? | 63(20.1) | 251(79.9) | 0(0) |
| 15 | Do you experience side effects when taking your drugs? | 0(0) | 314(100) | 0(0) |
| 16 | 55. Do you also take herbal drugs? | 104(33.1) | 190(60.5) | 20(6.4) |
| Total | 1213 | 2685 | 1126 | |
| Mean score N (%) | 75.8 (24.1) | 167.8 (53.4) | 70.4 (22.4) |
Over 60% of respondents reported that they never check their blood sugar levels, and over 40% reported that they never engage in exercise.
Hypotheses
The following hypotheses were tested in this study
Hypothesis 1: there is no significant correlation between age and knowledge.
Hypothesis 2: there is no significant correlation between age and attitude.
Table 5: Showing the correlation between age and KAP regarding diabetes
| Variables | r-value | p-value | Interpretation |
| Age And Knowledge | -0.107 | 0.059 | No correlation |
| Age And Attitude | 0.174 | 0.002 | Weak positive correlation |
Discussion
In terms of demographics, 29% of the respondents were aged 18-25; 50.6% were females; the majority had secondary school education; 43.3% were single (unmarried). The prevalence of diabetes in this study was 9.6%; in 2014 the WHO reported 8.5% of adults 18 years and older had diabetes and the number is said to have increased significantly, our study was higher than the 8.0% recorded by (Ramalan 2016) and comparable to slightly higher values of 10.3% and 10.5% reported by (Puepet & Ohovoriole, 2017) and (Chris, et. al., 2018) respectively in northeastern part of Nigeria. It is however higher than 7% reported in the northeast by (Gezawa, et. al., 2018), the marked difference in the prevalence of diabetes in this study compared to others may be due to the differences in the study settings, study population, the methodology, and in the year of study. Knowledge of a disease plays an important role in prevention and management of the disease condition, and from our results 67.8% of our respondents responded that they were aware of what diabetes is, but less than half of the respondents( 45%) responded they knew the correct reading of normal blood sugar and 42.4% of the respondents could identify normal blood sugar reading , high blood sugar reading (44.9%) and low blood sugar (56.4%), this knowledge is very important for the prevention and management of diabetes so as know when to seek for medical care, close to 50% of the population did not have this knowledge in our study, similar study was also conducted by (Umoh, V., et. al., 2020) in Uyo Having a positive attitude towards the prevention and management of diabetes is very important in the management of this disease condition, and in this study, more than half of the respondents (50.3%) responded positively to the reduction of food high in sugar, checking blood sugar regularly (69.7%), and that people with diabetes should exercise daily (70.8%), and also regular coke intake is bad for someone with high blood sugar (39.2%), this shows that the respondents have a positive attitude towards preventing and managing high blood sugar which is very important in the prevention and management of the disease, this was in line with studies made by (Umoh, V., et. al., 2020) and (Ifeoluwa, et. al., 2017). Practices regarding a disease condition will show if someone is at risk of a disease condition by failing in the correct management and prevention of the disease condition. In this study, majority (62.8 %) of respondents reported to have never checked their blood sugar, this shows bad practice from majority of the respondents because checking of blood sugar regularly is very important in the detection of pre-diabetes and diabetes so as to prevent complications and manage the disease condition early enough (Alele & Ilesanmi, 2014), 57.6% of respondents reported that they visit their health care provider sometimes, this is acceptable practices because majority of the respondents might only visit their healthcare provider when they seek healthcare , (80.9%) sometimes eat food high in fat and sugar in their daily diet, (81.2%) sometimes take soft drinks, (79.3%) sometimes eat late at night these are acceptable practices because the respondents are not always indulging in these risk factors of diabetes but how often they indulge in this practices will determine the outcome of their health in respect to diabetes, 43.9% of respondents reported that they do not monitor their weight, this is not an acceptable practice because monitoring of weight is important in the prevention and management of diabetes (Alele & Ilesanmi, 2014). The current study found there was no correlation between age and knowledge, but found a significant correlation between age and attitude, this means that age did not affect the knowledge of the respondents regarding diabetes, but the age of respondents influenced the attitudes of respondents regarding diabetes.
Conclusion
The study found a relatively moderate prevalence of diabetes and an acceptable level of KAP regarding diabetes mellitus among the study population. There was no correlation between age and knowledge with age, but there was a weak positive correlation between age and attitude. Further effective health education programs need to be carried out to improve the awareness and knowledge of the community regarding these diseases so that complications of these diseases can be prevented.
Recommendation
Based on the findings of the study, there are options for further practical interventions and corrective measures to improve health services delivery performance and to achieve the goal of public health practices, the following recommendations can be utilized. The government should continue sponsoring intensive health promotion and education campaigns on diabetes awareness and prevention through various mass media channels. Religious bodies should organize periodic health talks and seminars to sensitize their members about diabetes. Health workers in partnership with NGOs should carry out outreach programs to the community and other communities, providing education on diabetes prevention, diagnosis, and treatment.
Study Limitations
The limitation of this study was its setting which is in a small community and dealt with a small population, while our results are promising, we recommended a large survey and massive testing to broadly portray the current situation and suggest possible ways for lasting improvements of diabetes control and awareness.
Contributions to Knowledge
This study gave information about the prevalence, knowledge, attitude, and practice of Famgbe Community in Yenagoa local government area of Bayelsa State, and this knowledge can be used to know the problems that the community is facing as regards diabetes can be used in health education and promotion in the Community to help improve their health practices and can also be used for nearby communities to improve their health on diabetes.
Conflict of interest
There was no conflict of interest among the authors.
References
- Alele, F.O., & Ilesanmi, O.S. (2014). Knowledge and attitude of a semi-urban community in the south-south region of Nigeria towards diabetes mellitus. American Journal of Public Health Research. 2(3):81-85.
Publisher | Google Scholor - Al-Maskari, F., El-Sadig, M., Al-Kaabi, J.M., Afandi, B., Nagelkerke, N., & Yeatts, K.B. (2013). Knowledge, attitude and practices of diabetic patients in the United Arab Emirates. PLoS One. (1)8:e52857.17.
Publisher | Google Scholor - Berkman, N.D., Sheridan, S.L., Donahue, K.E., Halpern, D.J., & Crotty, K. (2011). Low health literacy and health outcomes: an updated systematic Department of Health 2002. National service framework for diabetes: Standards. Ann InternMed, 155(2):97-107.
Publisher | Google Scholor - Demaio, A.R., Dugee, O., De Courten, M., Bygbjerg, I.C., Enkhtuya, P., & Meyrowitsch, D.W. (2013). Exploring knowledge, attitudes, and practices related to alcohol in Mongolia: a national population-based survey. BMC Public Health, 13(1):178.
Publisher | Google Scholor - Gezewa, I.D., Puepet, F.H., Mubi, B.M., Uloko, A.E., Bakki, B., Talle, M.A., et. al. (2015). Socio-demographic and anthropometric risk factors of type 2 diabetes in Maiduguri, North-Eastern Nigeria. Sahel Med J, 18(5):1-7.
Publisher | Google Scholor - Ifeoluwa, 0.A., Patricia, U.O., Bolajoko, A. (2019). Knowledge, attitude and pratices towards diabetes mellitus among residents of Igbo-ora, a rural community in south-western Nigeria. The Nigeria journal of pharmacy, (53):2.
Publisher | Google Scholor - Kasper L. Harrison’s principle of internal medicine, 17th ed. Graw Hill Company: 2008.
Publisher | Google Scholor - Norris, S.L., Engelgau, M.M., & Narayan, K.M. (2001). Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials. Diabetes Care, 24:561-587.
Publisher | Google Scholor - Nurul, F.B., Nor Azilna, A.R., & Mainul, H. (2019). Knowledge, attitude and practice regarding hypertension among residents in a housing area in Selangor, Malaysia. Med pharms rep, 92(2):145-152.
Publisher | Google Scholor - Puepet, F.H., & Ohovoriole, A.E. (2008). Prevalence of risk factors for DM in non-DM population in Jos, Nigeria, 17(1):71-74.
Publisher | Google Scholor - Ramalan, M.A. (2016). Glycated hemoglobin in screening type 2 diabetes in Nigeria. Fellow, Medical College of Physicians (FMCP) dissertation’s part 2. Lagos; National Postgraduate Medical College of Nigeria.
Publisher | Google Scholor - Rani, P., Raman, R., Subramani, S., Perumal, G., Kumaramanickavel, G., & Sharma, T. (2008). Knowledge of diabetes and diabetic retinopathy among rural populations in India, and the influence of knowledge of diabetic retinopathy on attitude and practice. Rural Remote Health, 8(3):838.
Publisher | Google Scholor - Roglic, G., Unwin, N., Bennett, P.H., Mathers, C., Tuomilehto, J., Nag, S., Connolly, V., & King, H. (2005). The burden of mortality attributable to diabetes: Realistic estimates for the year 2000. Diabetes Care, 28(9)2130- 2135.
Publisher | Google Scholor - Umoh, V.A., Jombo, H.E., & Effiong, E.A. (2020) Knowledge, attitudes, and practices on diabetes mellitus among out-patients with type 2 diabetes in Uyo, South-South Nigeria. JMSCR, 11(8):423-430.
Publisher | Google Scholor - World Health Organization (2012). Prevention of diabetes mellitus.
Publisher | Google Scholor - Zaman, M.J., Patel, A., Jan, S., Hillis, G.S., Raju, P.K., Neal, B., & Chow, C.K. (2012). Socio-economic distribution of cardiovascular risk factors and knowledge in rural India. Int J Epidemiol, 41(5):1302-1314.
Publisher | Google Scholor














