

Case Report
Endometrial Tuberculosis Misdiagnosed as Endometrial Cancer in a Postmenopausal Woman: A Case Report and Literature Review
1 Aksum University, College of Health Science, Department of Obstetrics and Gynecology, Aksum, Tigray, Ethiopia.
2 Aksum University, College of Health Science, Department of Pathology, Aksum, Tigray, Ethiopia.
3 Mekelle University College of Health, Department of Obstetrics and Gynecology, Mekelle, Tigray, Ethiopia.
*Corresponding Author: Musie Negasi Gebreslase, Aksum University, College of Health Science, Department of Obstetrics and Gynecology, Aksum, Tigray, Ethiopia.
Citation: Musie N. Gebreslase, Kassie B., Guesh H., Negash D., (2025). Endometrial Tuberculosis Misdiagnosed as Endometrial Cancer in a Postmenopausal Woman: A Case Report and Literature Review. Journal of Surgical Case Reports and Reviews. Biores Scientia Publishers. 4(1):1-4. DOI: 10.59657/2993-1126.brs.25.030
Copyright: © 2025 Musie Negasi Gebreslase, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 19, 2025 | Accepted: October 03, 2025 | Published: October 10, 2025
Abstract
Background: Genital tuberculosis is a rare but important consideration in postmenopausal women, often presenting with symptoms that can mimic gynecologic malignancies such as endometrial cancer. In these cases, its variable clinical presentation can lead to a diagnostic challenge, and genital tuberculosis may be overlooked, particularly in the context of postmenopausal pyometra and cervical stenosis. A biopsy is often crucial for a definitive diagnosis, as clinical and radiological findings may be nonspecific.
Case Presentation: This report presents a case of postmenopausal women who underwent hysterectomy and bilateral salpingectomy with a diagnosis of suspected endometrial malignancy. However, the histopathological examination revealed tuberculosis endometritis.
Conclusion: The case highlights the importance of considering genital tuberculosis in the differential diagnosis, especially when malignancy is suspected. Antituberculosis therapy remains the cornerstone of treatment, even in the post-surgical setting, as the primary source of infection is often extragenital. Clinicians should be aware of the potential for misdiagnosis, and early identification of genital tuberculosis can lead to more appropriate management and avoid unnecessary interventions.
Keywords: genital tuberculosis; postmenopausal; endometrial cancer; ethiopia
Introduction
Tuberculosis remains a significant global public health challenge, particularly in developing nations, despite advancements in diagnosis and treatment [1]. While pulmonary tuberculosis—where the infection spreads beyond the lungs—is on the rise. Among these, genitourinary tuberculosis is the second most prevalent, next to lymph node involvement. Genitourinary tuberculosis often originates from a primary infection elsewhere in the body, most commonly the lungs, where the initial source may remain undetected [2]. This highlights the importance of comprehensive diagnostic approaches to identify and manage TB in its various forms [3].
Genital tuberculosis is more prevalent in females than males, with hormonal changes during pregnancy and menstruation potentially influencing the reactivation of latent tuberculosis and increasing blood flow to the genital organs. Infertility is a common complaint among women with genital tuberculosis, often leading to evaluation and diagnosis [4].
Genital tuberculosis accounts for 9% of all extrapulmonary tuberculosis cases. It is most commonly observed in women of reproductive age, often during evaluation for infertility [5]. The fallopian tubes are the most frequently affected, involved in 90-100% of cases, followed by the endometrium in 50-60%, ovaries in 10-30%, cervix in 5%, and vagina and vulva in less than 1% [7].
In postmenopausal women, genital tuberculosis is less common, which could be due to decreased vasculature to the genital organs. Tuberculosis of the endometrium can occur without fallopian involvement in such patients [1].
We report a case of female genital tuberculosis to highlight that genital tuberculosis is not uncommon and to briefly see the approach and management options in our setup.
Case presentation
A 57-year-old para 6 female patient with a 6-month history of lower abdominal pain. She had been amenorrheic for 10 years and reported no postcoital bleeding, offensive vaginal discharge, or constitutional symptoms such as cough, fever, weight loss, or night sweats. Her medical history was unremarkable, with no known drug or food allergies, family history of gynecologic or other malignancies, or prior gynecologic procedures. She denied smoking and alcohol consumption.
On clinical examination, she was alert. Her abdomen was non-tender and soft, with no palpable mass. The uterus was not enlarged but exhibited slight tenderness. The rest of the systemic examination was normal. On speculum examination, the cervix was flat and obliterated the external os; otherwise, the rest was unremarkable. A bimanual examination reveals mild tenderness.
An abdominal ultrasound revealed an enlarged uterus with hypoechoic areas and internal echoes. The endometrium was irregularly thickened with heterogenous and internal echogenic foci. Due to cervical stenosis, an endometrial biopsy was not feasible. Considering the clinical findings, transabdominal hysterectomy and bilateral salpingo-oophorectomy were performed with a provisional diagnosis of endometrial cancer.
Histopathological examination revealed necrotic debris lining the endometrial cavity, sheets of mixed inflammatory cell infiltrates, and numerous multinucleated giant cells with well-formed granulomata consistent with tuberculosis (Figure 1). The cervix and bilateral adnexa were unremarkable. After learning the postoperative diagnosis of tuberculous endometritis, the patient was started on anti-tuberculosis, and she is doing well.
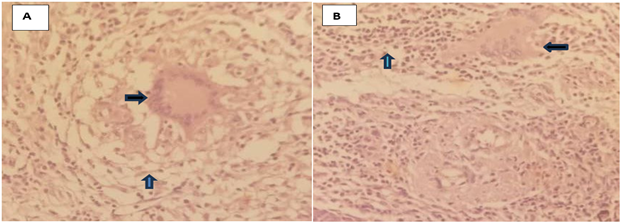
Figure 1: Hematoxylin and eosin-stained histologic sections. A. 10x magnification showing langhans type multinucleated giant cells (black arrow) surrounded by aggregates of epitheliod (blue arrow) histiocytes and lymphoplasmacytic inflame-matory cells. B. 10x magnification showing the multinucleated giant cells (black arrow) and extensive lymphoplasmacytic inflammatory cells (blue arrow).
Discussion
Tuberculosis is the most worrisome communicable disease worldwide. It remains a major health issue in most developing nations, and genital tuberculosis is responsible for a significant proportion of women seeking infertility treatment [6].
Genital tuberculosis is the second most common extrapulmonary tuberculosis, next to lymph nodes [3]. Isolated involvement is observed in 10-30% of patients, and female genital tuberculosis is more prevalent than male, and the possible explanation could be due to hormonal, anatomic, and extensive evaluation differences between both genders [4]. The exact prevalence of genital tuberculosis is difficult to know, as most cases are underreported, and due to the variable presentation of the cases, patients may not be evaluated for tuberculosis [6].
Genital tuberculosis occurs either due to reactivation of latent bacilli in the genital organs or secondary involvement from the already infected organs, mostly the lungs. The spread of the disease is through hematogenous or lymphatic routes, mostly from the lung or the abdomen [5].
Female genital tuberculosis is often considered a disease of young women, with the fallopian tubes, endometrium, ovaries, cervix, vagina, and vulva being areas affected in decreasing order. Notably, Myometrial involvement is rare and typically limited to the endometrial fundus, decreasing towards the cervix [2, 4]. Endometrial infection sheds monthly, and it is reinfected with extension from tubal infection with each cycle. It is rarely seen in postmenopausal women, and persistent endometrial infection without tubal involvement is possible, which is supported by its absence of monthly menstrual clearance [6].
The clinical presentation of female genital tuberculosis is variable, ranging from asymptomatic cases to symptoms such as abdominal pain, abnormal uterine bleeding, infertility, and vaginal discharge. Less common presentations include abdominal mass, tubo-ovarian abscess, and pyometra [3, 7]. Our patient presented with pyometra.
Diagnosing FGTB can be challenging due to its diverse manifestations. Pelvic ultrasound plays a crucial role in identifying pelvic pathology, although it is not specific to genital tuberculosis. Patients may present with an ovarian cyst, tubo-ovarian mass or abscess, hydrosalpinx, or pyosalpinx. Uterine features can include a thin endometrium, calcification, endometrial collection with irregular and thickened edges, and endometrial synechiae [7]. Pyometra is more common in post-menopausal women due to concomitant cervical adhesion and atrophy [8]. In our case, imaging revealed an irregularly heterogeneous thickened endometrium with areas of hypoechoic and echogenic internal foci, suggestive of genital tuberculosis. This highlights the importance of considering tuberculosis in the differential diagnosis of women presenting with gynecologic symptoms, regardless of age. Early recognition and appropriate treatment are essential to prevent complications and to improve patient outcomes.
In our case, imaging revealed an irregularly heterogeneous thickened endometrium with areas of hypoechoic and echogenic internal foci, suggesting the presence of FGTB. This highlights the importance of considering FGTB in the differential diagnosis of women presenting with gynecological symptoms, regardless of age.
Early recognition and appropriate treatment are essential to prevent complications such as infertility and to improve patient outcomes.
Supportive evidence is required to reach a conclusion, as imaging is nonspecific towards genital tuberculosis. Female genital TB is a paucibacillary disease; obtaining the bacteria from tissue or fluid of the genital tract is very challenging [9, 10]. Supportive tests in addition to the imaging mentioned above include menstrual blood analysis, endometrial curettage, and laparoscopic or open surgical tissue histopathology, which are helpful. In our case, endometrial curettage could not be done due to cervical stenosis, and we were forced to go for laparotomy.
The mainstay of treatment of genital tuberculosis is medical management, which is the initiation of antituberculosis (ATT) for 6–9 months. To stop the infection from spreading or perhaps recurring, ATT must be started even if there is no active illness in other pelvic structures. Under some circumstances, latent genital tuberculosis (GTB) may reactivate and cause problems like pelvic masses or chronic symptoms. Therefore, to guarantee total infection elimination, a full course of ATT is advised [6, 10, 11]. Surgical interventions are needed in situations where fertility enhancement is mandatory such as hydrosalpinx, pyosalpinx, tube-ovarian complexes or abscesses, Asherman syndrome, pelvic adhesions, and peritonitis, or in the case of failed medical management [7].
Conclusion
Genital tuberculosis is currently increasing. Due to its variable presentations, clinicians should lower their threshold in considering tuberculosis, especially in tuberculosis-endemic areas like our setup. Even though it needs further study, in patients diagnosed with genital tuberculosis after surgical interventions for non-tuberculosis reasons, it is better to continue with anti-tuberculosis as the primary source might be elsewhere.
Declarations
We would like to express our deepest gratitude to the patient for allowing us to write this case report.
Conflict of interest
There is no conflict of interest for all authors.
Ethical Consideration
Written consent was obtained from the patient to publish this article, and ethical approval for the case report was obtained from the Aksum University Ethics Committee.
Author contributions
Musie Negasi: Conceptualization, methodology design, analysis, investigation, data curation, writing original draft, and project administration. Birhanu Kassie: Data curation, review, and editing. Haftom Guesh: review and editing, analysis.Dawit Negash: Data curation, reviewing, and editing
References
- Güngördük K, Ulker V, Sahbaz A, Ark C, Tekirdag AI, (2007). Postmenopausal tuberculosis endometritis. Infect Dis Obstet Gynecol., 2007.
Publisher | Google Scholor - Arora A, Sadath SA. (2018). Genital tuberculosis in postmenopausal women with variable clinical presentations: A report of 3 cases. Case Rep Womens Health., 1-18.
Publisher | Google Scholor - Tzelios C, Neuhausser WM, Ryley D, Vo N, Hurtado RM. (2022). Female Genital Tuberculosis. Open Forum Infect Dis. 9(11):.1
Publisher | Google Scholor - Panda drs, Gupta drag, Varma drpp, Rao drtv. (2024). Female genitourinary tuberculosis: A clinico epidemiological and diagnostic study. International Journal of Gynaecology Sciences., 6(2):04–9.
Publisher | Google Scholor - Desai R, Kumar S, Brindini U. (2016). Female genital tuberculosis: a clinicopathological study. Int J Reprod Contracept Obstet Gynecol., 2780–2783.
Publisher | Google Scholor - Tuberculosis of the Female Genital Tract _ GLOWM.
Publisher | Google Scholor - Sharma JB, Khurana A, Hari S, Singh U, Yadav R, D. (2021). Evaluation of role of transabdominal and transvaginal ultrasound in diagnosis of female genital tuberculosis. J Hum Reprod Sci.,14(3):250–259.
Publisher | Google Scholor - Lee DH, Cho DH, Lee JH, Kim YR. (2021). A case of postmenopausal pyometra caused by endometrial tuberculosis. Korean Journal of Obstetrics & Gynecology. X., 55(6):429.
Publisher | Google Scholor - Malik S. (2020). Genital Tuberculosis and its Impact on Male and Female Infertility. US Endocrinol.,16(2):97–103.
Publisher | Google Scholor - Wanyoike-Gichuhi J, Parkar R. (2014). East african medical Journal ATYPICAL TUBERCULOSIS PRESENTING WITH PRIMARY INFERTILITY AND ENDOMETRIAL CALCIFICATION ATYPICAL TUBERCULOSIS PRESENTING WITH PRIMARY INFERTILITY AND ENDOMETRIAL CALCIFICATION. Vol. 91, East African Medical Journal..
Publisher | Google Scholor - Kyejo W, Moshi B, Gidion D, Abeid M, Somji S, Kaguta M, et al. (2023). A rare case report of tuberculosis endometritis in a private hospital Dar es salaam, Tanzania. SAGE Open Med Case Rep.,11.
Publisher | Google Scholor




















