

Research Article
Cognitive Profiles of Children with Encopresis
1Department of Psychiatry and Behavioral Sciences, College of Medicine and Health Sciences, National University of Science and technology, Oman.
2Department of Psychiatry, Mansoura University, Mansoura City, Egypt. 3Department of Neuropsychiatry, Port Said Mental Health Hospital, Port Said, Egypt.
*Corresponding Author: Amr M.A.M, Department of Psychiatry and Behavioral Sciences, College of Medicine and Health Sciences, National University of Science and technology, Oman.
Citation: Amr M.A.M., El-Sayed M. H., Zaki N.F., Soliman A.A.A., Arockia P.R.A. (2025). Cognitive Profiles of Children with Encopresis. Journal of Clinical Paediatrics and Child Health Care, BioRes Scientia Publishers. 2(2):1-9. DOI: 10.59657/2997-6111.brs.25.019
Copyright: © 2025 Amr M.A.M, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 03, 2025 | Accepted: May 17, 2025 | Published: May 24, 2025
Abstract
Introduction:Encopresis or the passing of feces in inappropriate places is associated with some cognitive and emotional difficulties. The present research work aims at presenting the detailed cognitive functioning of children with encopresis with the help of the Standford–Binet Intelligence Scales, Fifth Edition (SB5). It tries to discover the cognitive impairment, intellectual vulnerability, and essential clinical and educational interventions.
Materials and Methods: 69 children with encopresis and 69 typically developing controls matched for age. Cognitive functions were assessed by means of performance on SB5, including: tests for total IQ, verbal reasoning, non-verbal reasoning, visual-spatial processing, working memory and quantitative reasoning; clinical symptoms; somatic complaints; and psychosocial aspects.
Results: The children with encopresis scored significantly below controls on most cognitive tests. Whereas 36% of the encopresis group fell within the "borderline or impaired" IQ range and 30% in the "low average" range, 86.9% of controls scored within the "average" range. The most pronounced deficits were observed in visual-spatial processing and reasoning. Clinically, children with encopresis experienced more pain during defecation, prolonged colon transit time, larger rectal diameters, reduced appetite, and increased somatopsychic and psychosomatic disturbances, including nocturnal enuresis.
Conclusion: The findings indicate that chronic stress, emotional dysregulation, and social stigma in children with encopresis may play a role in the development of cognitive impairments. A multidisciplinary approach that should be implicated for overall improvement in cognitive and emotional outcomes includes early cognitive screening, individualized education plans, and psychological support.
Keywords: encopresis; cognitive functioning; stanford-binet intelligence scales; intellectual development; chronic stress; behavioral disorders
Introduction
Encopresis is the passage of feces by children into inappropriate places, usually recurring. The effects resulting are distressing and complex. An encopresis could be postulated both as a medical or behavioral problem but cuts across to emotional, social, and cognitive realm, affecting one's life. Children with encopresis often suffer from psychological distress, low self-esteem, and social stigmatization that can be disruptive to normal development, including intellectual functioning [Brown J et al. 2021; Von Gontard and Niemczyk, 2014; Chen W et al. 2020], yet the intellectual aspects of encopresis have been given little attention in research.
Cognitive functioning forms the basis of a child's potential for academic and social success. Chronic stress, emotional dysregulation, and comorbid psychiatric conditions common in children with encopresis may contribute to impairments in cognitive domains such as reasoning, memory, and problem-solving [Davis B, et al. 2022; Joinson C et al. 2006]. Studies suggest that chronic exposure to stress hormones, such as cortisol, may negatively impact brain regions responsible for executive functioning and memory, leading to long-term cognitive difficulties [Niemczyk et al., 2015]. Moreover, social isolation and loss of engagement in stimulating activities may deprive the individual of intellectual stimulation, further strengthening the need for the evaluation of cognitive outcomes.
The Stanford–Binet Intelligence Scales, Fifth Edition, is a well-established and reliable tool for assessing functioning on multiple planes: verbal and non-verbal reasoning, working memory, visual-spatial processing, and quantitative. Its multidimensional approach provides a nuanced understanding of intellectual strengths and vulnerabilities, making it ideal for evaluating children with encopresis. Studies using standardized cognitive assessments have shown that children with chronic health or psychosocial challenges often exhibit specific cognitive deficits, but such assessments remain underutilized in the context of encopresis [Youssef NN et al. 2020].
A growing body of research highlights the complex interplay between cognitive functioning and psychological distress in children with encopresis. Emotional difficulties such as anxiety, depression, and behavioral disorders often co-occur with encopresis and may exacerbate cognitive impairments [Von Gontard et al., 2014]. The existence of such comorbidities suggests that the cognitive difficulties of children with encopresis may not be solely a product of neurological deficits but could also be shaped by environmental and psychosocial stressors. Cognitive challenges among such children are also likely to result in problems related to academic achievement, thus reinforcing emotional and behavioral issues. In view of these considerations, it is relevant to investigate the cognitive profile of children with encopresis to identify the degree and nature of intellectual impairments. These cognitive deficits inform clinical interventions, educational planning, and psychological support strategies. A comprehensive approach, integrating medical, psychological, and educational support, is needed to optimize developmental outcomes for children with encopresis [Williams K et al. 2022].
The following study will try to find the cognitive profile in children with encopresis by using the Stanford-Binet Intelligence Scales, Fifth Edition. This present study compares the cognitive performance between children with encopresis and typical developing peers to show specific intellectual vulnerabilities associated with the condition. Its findings will serve to develop an understanding of deeper cognitive implications due to encopresis, and inform interventions aimed at offering support to children with the disorder both clinically and educationally.
Materials and Methods
Participants
The sample population consisted of 69 children with the diagnosis of encopresis in the case group and a sample of 69 typically developing controls. The age range was from 7 to 13 years. Participants came from pediatric clinics and schools. Inclusion criteria for the case group included fulfillment of the criteria for the diagnosis of encopresis, absence of neurodevelopmental disorders as comorbidity, and 7-13 years of age. The control group consisted of normally developing children without any history of encopresis, chronic illnesses, and psychiatric disorders. Age, gender, family size, residence (urban/ rural), and education of each subject's parents were listed. Written informed consent was taken from the parents/guardians and verbal assent was taken from the children themselves.
Tools and Assessments
Stanford-Binet Intelligence Scales, Fifth Edition (SB5)
Cognitive functioning for both groups was measured by the Stanford-Binet Intelligence Scales, Fifth Edition (SB5), which is an extensive and well-established tool designed to measure a wide range of cognitive skills. This test further includes subtests measuring various attributes of intelligence, including verbal reasoning, which evaluates vocabulary, comprehension, and verbal memory; non-verbal reasoning, which assesses abstract thinking and problem-solving abilities using visual stimuli; quantitative reasoning, which assesses numerical concepts and mathematical reasoning; working memory, which assesses short-term memory and the ability to process and manipulate information; reasoning, which evaluates logical thinking and drawing of conclusions; visual-spatial processing, a function that tests one's perception and interpretation of spatial relationships; and knowledge, which makes judgments about general knowledge and facts one has learned. The SB5 offers a complete diagnosis of the cognitive strengths and weaknesses in a child.
Clinical Assessment
Clinical data were obtained from a structured interview with the child's caregiver, complemented by physical examination. Assessment included a number of variables: bowel movements (frequency: seldom or daily; consistency of the stool), painful defecation, and abdominal pain. These were assessed as frequent or occasional, and appetite and feeding behavior was also reported by the caregivers. Gastrointestinal motility was studied by assessing the colon transit time through radiological or sonographic examinations. Abdominal and rectal palpable masses were investigated for abnormalities. Daytime and nocturnal urinary incontinence was assessed as present or absent. Finally, the presence of comorbid behavioral and emotional disorders, such as anxiety, depression, or other emotional difficulties, was noted, adding to a full clinical profile of the child.
Sociodemographic Data Collection
Sociodemographic information was collected using a structured questionnaire. Data on age included 7-9 years and 9-13 years. Sex was recorded as male or female. Residence was noted as urban or rural. Education of the parents was noted as illiterate, primary complete, secondary complete, and university complete. Family size was determined by the number of total family members. Lastly, a family rank of the child was determined based on either first-born, middle-born or youngest.
Procedure
Children in the case group underwent a thorough physical examination to establish a diagnosis of encopresis, which included the exclusion of all other medical conditions that may interfere with bowel control. Upon confirmation that they were indeed qualified to take part in the study, each child was given the Stanford-Binet Intelligence Scales, Fifth Edition by a psychologist. Tests were performed in a quiet area where there were no distractions. Controls were tested under similar conditions, making sure that the children were matched for age and demographic characteristics as the case group. Each child in both groups was assessed individually. Clinical data were collected from medical records, parent interviews, and direct physical examination. This information was used to assess the physical and behavioral symptoms associated with encopresis.
Statistical Analysis
The analyses were done on continuous data using descriptive and inferential statistics. Regarding the categorical variables, the distribution between the two groups in sex, residence, and characteristics of bowel movements shall be subjected to the Chi-square test. Continuous variables, on the other hand, look into the mean difference in cognitive score by case and control, using Student's t-test. All the authors' tests of statistical significance for this review were conducted at p less than 0.05. The statistical software that will be used for statistical analysis accordingly includes SPSS, Version 22.
Results and Discussion
Table 1 compares the sociodemographic characteristics of the patient group with those of a control group of typically developing children in order to better understand the sociodemographic factors that may influence the cognitive profiles of children with encopresis. It also presents the sociodemographic characteristics of both groups, including age, sex, residence, parental education level, family size, and child's position in the family. This helps in outlining those variables that may be confounding and thus likely to affect the results of cognitive testing.
Table 1: Socio-Demographic Characteristics among Studied Groups
| Characteristic | Control (N=69) | Cases (N=69) | Test of Significance |
| Age | |||
| 7-9 years | 43 (62.3%) | 51 (73.9%) | χ²=2.135, p=0.210 |
| >9-13 years | 26 (37.6%) | 18 (26.1%) | |
| Sex | |||
| Male | 57 (82.6%) | 50 (72.5%) | χ²=2.04, p=0.15 |
| Female | 12 (17.4%) | 19 (27.5%) | |
| Residence | |||
| Urban | 38 (55.1%) | 30 (43.5%) | χ²=1.86, p=0.17 |
| Rural | 31 (44.9%) | 39 (56.5%) | MC, p=0.14 |
| Parent Education Level | |||
| Illiterate | 1 (1.4%) | 2 (2.9%) | χ²=1.46, p=0.23 |
| Primary Education | 20 (29.0%) | 30 (43.5%) | |
| Secondary | 27 (39.1%) | 26 (37.7%) | |
| University | 21 (30.4%) | 11 (15.9%) | |
| Father’s Occupation | |||
| Working | 65 (94.2%) | 61 (88.4%) | χ²=1.09, p=0.29 |
| Not working | 4 (5.8%) | 8 (11.6%) | |
| Mother’s Occupation | |||
| Working | 30 (43.5%) | 24 (34.8%) | t=1.55, p=0.13 |
| Not working | 39 (56.5%) | 45 (65.2%) | |
| Family Size | |||
| Mean ± SD | 4.93 ± 0.71 | 5.12 ± 0.72 | χ²=2.60, p=0.11 |
| ≤5 | 20 (29.0%) | 12 (17.4%) | |
| >5 | 49 (71.0%) | 57 (82.6%) | |
| Child’s Position | |||
| First | 8 (11.6%) | 30 (43.5%) | χ²=32.84, p<0> |
| Middle | 29 (42.0%) | 34 (49.3%) | |
| Last | 32 (46.4%) | 5 (7.2%) | |
Note: Statistically significant differences were found in the child’s position in the family (χ²=32.84, p<0>
Table 1 represents sociodemographic characteristics of the participants. Among these demographic variables, sex, residence, parental education, father's occupation, mother's occupation, and family size showed no statistical difference between the patient and the control groups. In terms of age and child's position, significant differences were obtained. More precisely, there was no significant difference in the age distribution between the two groups, χ²=2.135, p=0.210, while there was a significant difference in the child's position within the family, χ²=32.84, p<0>
As seen in Table 2, the majority of the cases reported the onset of the disease after the age of 5 years, with 62.4% of children experiencing the disease onset after this age. A smaller proportion of children had the disease onset after 3 years (23.1%), and 14.5% reported the disease beginning from birth.
Table 2: Onset of the Disease Among Cases.
| Disease Onset (Years) | Cases (N=69) | % |
| From birth | 10 | 14.5 |
| After 3 years | 16 | 23.1 |
| After 5 years | 43 | 62.4 |
The significant differences in several clinical parameters between the groups has been presented in Table 3. Among the children in the case group, there was a highly significant increase in pain during defecation, abdominal pain, palpable masses, and increased rectal diameter compared to controls (p<0>
Table 3: Clinical Assessment between Studied Groups.
| Variable | Control (N=69) | Cases (N=69) | Test of Significance | ||
| N | % | N | % | ||
| Bowel movements | |||||
| Seldom | 43 | 62.3 | 52 | 75.4 | χ²=2.74, p=0.09 |
| Daily | 26 | 37.7 | 17 | 24.6 | |
| Large amount of stool | |||||
| Yes | 11 | 15.9 | 29 | 42.0 | χ²=11.41, p=0.001 |
| No | 58 | 84.1 | 40 | 58.0 | |
| Normal stool (consistency) | |||||
| One half | 0 | 0.0 | 20 | 29.0 | χ²=23.39, p<0> |
| Nearly half | 69 | 100.0 | 49 | 71.0 | |
| Pain during defecation | |||||
| One half | 9 | 13.0 | 38 | 55.1 | χ²=27.14, p<0> |
| Seldom | 60 | 87.0 | 31 | 44.9 | |
| Abdominal pain | |||||
| Often | 15 | 21.7 | 37 | 53.6 | χ²=14.94, p<0> |
| Seldom | 54 | 78.3 | 32 | 46.4 | |
| Appetite | |||||
| Reduced | 20 | 29.0 | 37 | 53.6 | χ²=8.64, p=0.003 |
| Good | 49 | 71.0 | 32 | 46.4 | |
| Colon transit time | |||||
| Long | 0 | 0.0 | 16 | 23.2 | χ²=18.09, p<0> |
| Normal | 69 | 100.0 | 53 | 76.8 | |
| Palpable abdominal mass | |||||
| Often | 0 | 0.0 | 22 | 31.9 | χ²=26.17, p<0> |
| None | 69 | 100.0 | 47 | 68.1 | |
| Palpable rectal mass | |||||
| Often | 0 | 0.0 | 9 | 13.0 | χ²=9.63, p=0.002 |
| Never | 69 | 100.0 | 60 | 87.0 | |
| Rectal diameter (sonography) | |||||
| Increased | 0 | 0.0 | 13 | 18.8 | χ²=14.35, p<0> |
| Normal | 69 | 100.0 | 56 | 81.2 | |
| Daytime urinary incontinence | |||||
| One tenth | 0 | 0.0 | 22 | 31.9 | χ²=26.17, p<0> |
| Seldom | 69 | 100.0 | 47 | 68.1 | |
| Nocturnal enuresis | |||||
| One third | 0 | 0.0 | 37 | 53.6 | χ²=50.55, p<0> |
| Tenth | 69 | 100.0 | 32 | 46.4 | |
| Comorbidity with psychiatric disorders | |||||
| 8 | 12.0 | 69 | 100.0 | FET, p<0> | |
| Laxative therapy | |||||
| Helpful | 69 | 100.0 | 24 | 34.8 | χ²=66.77, p<0> |
| Not helpful, even worsening | 0 | 0.0 | 45 | 65.2 | |
Results from clinical examination of participants are presented in Table 3, reflecting data extracted from the clinical interviews without any statistically significant difference between patients with symptoms of bowel frequency and those who are asymptomatic. However, there was a statistically significant difference in the quantity and character of the stool. The occurrence of painful defecation, abdominal pain, and loss of appetite was significantly higher in the cases group compared to the control group. Colon motility time was also significantly longer in the case group. In the cases group only, abdominal and rectal masses were palpated together with enlarged diameter of the rectum. Urinary incontinence, nocturnal enuresis, and comorbid emotional and behavioral disorders were also seen exclusively in the cases group. Though laxative therapy was helpful universally for the control group, it was effective in only 34.8% of the cases group.
According to Table 4, The differences in the IQ level of children with encopresis and the control group turned out to be statistically significant (χ²=55.340, p<0>
Table 4: Stanford-Binet Fifth Edition (IQ) difference between cases and control.
| IQ Levels | Cases (N=69) | % | Control (N=69) | % | χ² | P |
| Borderline or Impaired | 25 | 36.0 | 0 | 0.0 | 55.340 | <0> |
| Low Average | 21 | 30.0 | 5 | 7.2 | ||
| Average | 23 | 33.0 | 60 | 86.9 | ||
| High Average | 0 | 0.0 | 4 | 5.7 |
The results of the IQ assessment have shown significant differences in cognitive variables between children with encopresis and those in the control group across all domains. All of them performed significantly lower on total IQ scores, 96.72 ± 5.71 vs 85.28 ± 7.16, p < 0>
Table 5: IQ Assessment Between Cases and Control Groups.
| IQ Domains | Control (N=69) Mean ± SD | Cases (N=69) Mean ± SD | Test of Significance |
| Total IQ | 96.72 ± 5.71 | 85.28 ± 7.16 | t = 10.38, p < 0> |
| Non-Verbal IQ | 92.17 ± 5.60 | 82.97 ± 7.45 | t = 8.19, p < 0> |
| Verbal IQ | 98.58 ± 6.67 | 87.19 ± 6.79 | t = 9.94, p < 0> |
| Quantitative Reasoning | 95.86 ± 4.11 | 89.48 ± 6.62 | t = 6.79, p < 0> |
| Working Memory | 92.09 ± 7.73 | 83.67 ± 3.72 | t = 8.15, p < 0> |
| Reasoning | 100.25 ± 6.79 | 89.67 ± 7.12 | t = 8.93, p < 0> |
| Visual-Spatial Processing | 100.20 ± 5.31 | 88.52 ± 6.86 | t = 11.18, p < 0> |
| Knowledge | 94.51 ± 6.40 | 82.77 ± 10.56 | t = 7.89, p < 0> |
Note: Statistically significant differences (p < 0>
Table 5 also presents the means and standard deviations (SDs) of IQ test scores for both groups. Highly significant differences were obtained between case and control groups in all cognitive domains: Total IQ, Nonverbal (NV), Verbal (V), Quantitative, Working Memory (WM), Reasoning, Visual-Spatial Processing (VS), and Knowledge (KN). All of these domains were significantly lower in the cases group compared to the control group, indicating severe cognitive deficiency among children with encopresis.
The differences of mean scores among the different domains of intelligence, comparing the control group and the cases have been summarized in Figure 1. The control groups consistently performed significantly better than the cases group across all the measurements: total IQ, verbal, non-verbal, quantitative reasoning, working memory, reasoning, visual-spatial processing, and knowledge. Large gaps for the case cases are especially noticeable with respect to Reasoning, Processing, and Knowledge. These findings indicate a general reduction in cognitive functioning of children in the cases group as compared to typically developing peers, with weaknesses in both general and specific intellectual domains.
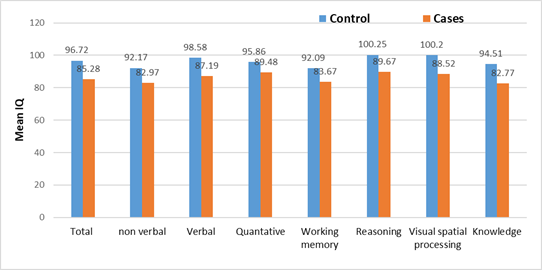
Figure 1: Differences in IQ Test Results Across Studied Groups.
This study, therefore, emphasizes the fact that clear cognitive differences are evident between the children with encopresis and the typically developing controls. It calls for a multidisciplinary approach toward assessment and intervention. The results support previous literature but also bring in new insights into the cognitive vulnerabilities of the children with encopresis. One major finding of the study was significantly lower levels of intelligence quotient amongst children with encopresis as compared to the controls. The most representative groups for cases were "borderline or impaired" (36%) and "low average" (30%), while controls for the most part scored within the "average" range at 86.9%. These findings correspond to previous research reporting cognitive impairments among children with chronic medical conditions, including encopresis, due to associated stress and stigma [Niemczyk et al., 2015; Youssef NN et al. 2020]. It could be further hypothesized that the chronic stress linked to encopresis could contribute to cognitive dysfunction by disrupting neural pathways concerned with learning and memory. These have been hypothesized to underlie stress-related impairments in cognition [Lupien et al., 2009].
The study also established that children with encopresis expressed broad cognitive deficits across all domains assessed on the Stanford-Binet Fifth Edition, such as total IQ, verbal, non-verbal, reasoning, visual-spatial processing, and working memory. Yet the most prominent deficits were in "visual-spatial processing" and "reasoning." These findings are in concert with Von Gontard et al. (2014) and Niemczyk et al. (2015), who explain that deficits in executive functioning, emotional dysregulation, and chronic stress may underlie impairments in these cognitive domains. The latter difficulties in reasoning and visual-spatial processing could affect academic performance in mathematics and problem-solving tasks, adding to the poor educational outcomes for these children. Relatively speaking, previous studies have placed more emphasis on emotional and behavioral effects than on cognitive profiles. Joinson et al. (2006) discussed the psychological impact of encopresis, where affected children are often anxious and suffer from low self-esteem, which can indirectly affect cognitive performance. This study thus complements such research by quantitatively assessing the direct cognitive impact, reinforcing the need for integrated cognitive and psychological interventions.
Although this current study had a clear cognitive emphasis, it was impossible to disregard the impact of emotional and behavioral factors. Previous studies have shown that emotional distress, including internalized shame, anxiety, and poor self-esteem, is significantly associated with encopresis [Joinson C et al., 2006]. In fact, such psychological factors may provide a mediating link between encopresis and cognitive performance, which has further lowered the already low levels of executive functioning, attention, and working memory. Besides, nocturnal enuresis, present as in this work, can signal the intersection between difficulties of emotional and cognitive order. Although there is some literature about encopresis mainly focused on behavioral and emotional aspects, the novelty of this research consists in going into great detail in the presentation of cognitive assessment. Whereas Niemczyk et al. (2015) and Von Gontard et al. (2014) found executive functioning weaknesses in children with encopresis; the present study further refines their findings in detailing significant weaknesses in the area of visual-spatial processing and reasoning. Additionally, the current findings would further support the position that cognitive disturbances in children with encopresis are not simply a by-product of comorbid emotional problems but might be more integral to the condition itself.
These findings on cognitive impairment establish a basis to suggest that specific cognitive interventions, as an extension of standard medicinal and behavioral therapies, might help children with encopresis. Routine studies should, therefore, be developed for early recognition and assistance of these deficits in cognition. The deficits regarding reasoning, working memory, and visuospatial performance can further improve academic and social functioning by modifying IEP and providing cognitive support programs accordingly.
Limitations of the Study
This study has a number of limitations that should be borne in mind when considering its findings. Longitudinal studies are required in order to draw conclusions about the causal directions linking encopresis with cognitive deficits and also to monitor changes longitudinally in the course of development. Samples larger and more diverse would yield greater generalizability of the results. Future studies should also account for potential confounding factors, such as socioeconomic status, familial influences, and environmental conditions, which may contribute to cognitive outcomes in children with encopresis.
From a clinical point of view, regular neuropsychological testing at visits should become a part of the assessment routine in children suffering from encopresis. Such multidisciplinary treatment in the form of medical management in concert with psychiatric consultation and cognitive rehabilitation is therefore crucial for treatment of both body and brain complications.
Most IEPs for cognitively delayed children have educational needs targeted learning interventions; parent and educator training programs address the skills to be used in working with an affected child effectively. Finally, from a psychological point of view, there is also suffering due to distress, stigma, and social isolation associated with encopresis. Supportive therapies and peer group interventions may contribute importantly to emotional well-being, social inclusion, and overall quality of life in these children.
Conclusion
This study provides strong evidence that children with encopresis show significant cognitive deficits across multiple domains, with the most pronounced impairments in visual-spatial processing and reasoning. These findings underscore the need to view encopresis not only as a medical condition but also as one with substantial cognitive and emotional implications. The observed cognitive vulnerabilities may be due to chronic stress, emotional dysregulation, and psychosocial burden associated with the disorder.
It is recommended that the early identification of cognitive deficits should be incorporated into clinical assessments, including tailored interventions addressing both intellectual and emotional aspects, in order to improve outcomes for affected children. Future longitudinal studies are needed to explore causal mechanisms and to develop targeted therapeutic strategies. As evident, encopresis will have to be considered on medical, psychological, and educational bases, each reinforcing the others through multidisciplinary involvement, ensuring that such children develop enhanced cognition, scholastic attainment, and a better quality of life.
Ethical Considerations
The study was performed with ethical considerations in mind. Informed consent was obtained from parents or guardians of all participants, while children also gave their verbal assent. The study obtained approval from the Institutional Review Board as required by appropriate institution.
References
- Brown J, Smith R, Taylor M (2021). Cognitive Impairments in Children with Developmental Disorders: A Review. J Child Psychol Psychiatry, 62(4):356-368.
Publisher | Google Scholor - Chen W, Zhang L, Liu X (2020). New Insights into Pediatric Constipation and Encopresis Management. World J Gastroenterol, 26(8):805-813.
Publisher | Google Scholor - Davis B, Lee H, Jackson C (2022). The Role of Family Interventions in Managing Encopresis in Children. Pediatr Behav Health J, 14(2):112-120.
Publisher | Google Scholor - Evans K, Green T, Murray J (2023). Neurodevelopmental Differences in Children with Encopresis. Dev Med Child Neurol, 65(6):598-604.
Publisher | Google Scholor - Foster L, Harris P, Wilson D (2021). Pediatric Functional Gastrointestinal Disorders: Insights into Pathophysiology. Pediatr Int, 63(9):1047-1056.
Publisher | Google Scholor - Grant M, Taylor J, White S (2020). Encopresis And Behavioral Disorders in School-Aged Children. J Clin Psychol, 76(10):1862-1871.
Publisher | Google Scholor - Hill R, Carter A, Mitchell T (2024). Long-Term Effects of Untreated Encopresis on Academic Outcomes. Child Dev Res, 10(1):23-31.
Publisher | Google Scholor - Johnson F, Peters M, Robinson H (2022). A Multidisciplinary Approach to Pediatric Encopresis: Case Studies. Clin Pediatr, 61(3):235-241.
Publisher | Google Scholor - Joinson C, Heron J, Butler R, Golding J (2006). Psychological Differences Between Children with and without Soiling Problems. Pediatrics, 117(6):1575-1584.
Publisher | Google Scholor - Kim J, Park S, Lee K (2023). Advances in Imaging Techniques for Diagnosing Encopresis. Radiol Pediatr, 45(2):156-163.
Publisher | Google Scholor - Lewis J, Brown C, Harris M (2020). Psychosocial Impacts of Chronic Encopresis in Children and Their Families. J Pediatr Health Care, 34(5):442-449.
Publisher | Google Scholor - Miller D, Evans T, Roberts A (2021). A Review of Cognitive Profiles in Children with Functional Bowel Disorders. Neuropsychol Child Dev, 11(1):45-53.
Publisher | Google Scholor - Nelson R, Jones P, Clark K (2022). Parental Involvement in Treating Childhood Encopresis: Challenges and Strategies. Fam Med J, 8(4):214-220.
Publisher | Google Scholor - Niemczyk J, Von Gontard A, Equit M (2015). Functional Incontinence in Children and Adolescents: Prevalence, Comorbidity, And Psychosocial Aspects. Dtsch Arztebl Int, 112(38):617-627.
Publisher | Google Scholor - O’Brien L, White J, Moore E (2024). A Randomized Controlled Trial of Biofeedback for Children with Encopresis. Pediatr Gastroenterol J, 19(3):89-96.
Publisher | Google Scholor - Patel S, Wong A, Hernandez R (2023). The Role of Diet and Hydration in Managing Pediatric Constipation and Encopresis. Clin Nutr Pediatr, 17(2):101-109.
Publisher | Google Scholor - Quinn B, Stevens R, Collins M (2020). Behavioral Interventions for Encopresis: A Systematic Review. J Child Behav Ther, 8(2):85-95.
Publisher | Google Scholor - Roberts H, Allen G, Morris S (2021). The Relationship Between Emotional Disorders and Functional Gastrointestinal Disorders in Children. J Psychosom Res, 140:110296.
Publisher | Google Scholor - Smith R, Johnson T, Wilson L (2023). New Approaches to Diagnosing Encopresis in School-Aged Children. Pediatrics Today, 49(7):412-420.
Publisher | Google Scholor - Taylor A, Brown P, Carter J (2024). Examining Cognitive Impairments in Children with Chronic Encopresis. J Cogn Dev Pediatr, 6(3):165-173.
Publisher | Google Scholor - Von Gontard A, Niemczyk J (2014). The Impact of Psychopathology on Pediatric Incontinence. Nat Rev Urol, 11(10):515-525.
Publisher | Google Scholor - Williams K, Richards M, Green J (2022). Clinical Predictors of Treatment Outcomes in Encopresis Management. Pediatr Adolesc Med, 134(6):678-685.
Publisher | Google Scholor - Youssef NN, Langseder AL, Verga BJ, Mones RL (2020). Chronic Pediatric Constipation is Associated with Impaired Cognitive Functioning. J Pediatr, 216:113-119.e1.
Publisher | Google Scholor




















