

Case Report
Case Report: Croup Caused by Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2)
Second-year Resident Physician in Pediatrics. IHSS-HRN. UNAH-VS Pediatrics.
*Corresponding Author: Ana G. Rodríguez, Second-year Resident Physician in Pediatrics. IHSS-HRN. UNAH-VS Pediatrics.
Citation: Rodríguez A.G, Velásquez B, Banegas L, Portillo M. (2025). Case Report: Croup Caused by Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2). Journal of Clinical Paediatrics and Child Health Care, BioRes Scientia Publishers. 2(1):1-4. DOI: 10.59657/2997-6111.brs.25.013
Copyright: © 2025, Ana G. Rodríguez, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 06, 2024 | Accepted: December 28, 2024 | Published: January 06, 2025
Abstract
We described the first case of croup associated with SARS-COV-2 in the pediatric Intensive Care Unit of the Instituto Hondureño de Seguridad Social – Hospital Regional del Norte (IHSS-HRN) with clinical manifestations of severe croup in a previously healthy9 months old child, who required rapidintubation sequence (RIS),mechanical ventilation assistance and management in the intensive care unit. The child responded to standard treatment of croup in addition of Remdesivir.
Keywords: croup; sars-cov-2; remdesivir
Introduction
In most cases, determining the etiology of croup is rarely useful. However, currently, due to the pandemic, identifying whether croup is associated with SARS-CoV-2 infection has acquired a novel importance for the management and isolation of hospitalized patients [1]. Croup is the most common cause of acute upper airway obstruction in childhood, with predominance between 6 months and 3 years of age. The triad: dysphonia, metallic cough and inspiratory stridor, with or without dyspnea, generally after a catarrhal prodromal picture characterizes this disease. Most cases are of viral etiology and, although it is often a respiratory emergency, it is usually mild [2]. In rare cases, croup leads to acute respiratory failure requiring intubation and mechanical ventilation [3]. It has been reported that 1 in 30,000 cases become fatal [4].
Children are less affected by SARS-COV-2 than adults, and clinical disease of COVID-19 occurs in less than 2% of total confirmed cases, with the majority experiencing mild illness that does not require hospitalization [5]. The disease occurs in children as a consequence of household exposure to SARS-COV-2. Respiratory involvement is usually an upper respiratory tract infection or pneumonia, which may progress to acute respiratory distress syndrome (ARDS) or multi-organ dysfunction [6, 7]. Recently, a total of 401 patients diagnosed with croup have been reported in some studies during the peak of infection of the Delta variant, and 107 cases reported for the Omicron variant which represented twice the number of cases normally recorded [8]. In the Pediatric Intensive Care Unit of the IHSS-HRN, a total of 83 patients with severe SARS-COV-2 have been admitted in the 2 years of the pandemic, which represents around 5.6% of the total number of children admitted to the hospital for SARS-COV-2 [9].
Clinical Case
A 9-month-old male infant, with no previous personal or family pathological history, with a vaccination schedule according to the Expanded Immunization Program complete for his age, with a Z score (weight/height) above 2. With a history of hyaline rhinorrhea and fever of 2 days of evolution, dry cough with metallic characteristics of 1 day of evolution. The patient was admitted to the IHSS-HRN emergency room with mixed acute respiratory failure secondary to upper airway obstruction (inspiratory stridor audible without a stethoscope, silent lungs, severe work of breathing, Taussig score of 9 points, heart sounds of decreased intensity and encephalopathic (sleepy). The patient had a positive reverse transcription polymerase chain reaction (RT-PCR) for SARS-COV-2, with no possibility of performing genomic sequencing to type the variant. The result of serology for influenza was negative. Both parents with positive serology for SARS-COV-2, without vaccination, deny respiratory symptoms. The patient was transferred to the ICU, a rapid sequence intubation protocol was performed during laryngoscopy. It was observed that the patient had significant edema and erythema of the glottis, without secretions or exudates, which made intubation with a 4.0 Fr. ETT (endotracheal tube) impossible, so he was intubated with an ETT. 3.5 Fr. with balloon without the need to inflate it, not recording a leak in the mechanical ventilator.
Laboratories upon admission reported leukocytosis due to lymphocytes, CRP 13.4 mg/L, procalcitonin 0.1 ng/mL, ferritin 50 ng/mL, IL-6: 29.5 pg/mL, D-dimer: 0.22 µg/mL. Patient with hypoxemia (P/F: 184). Chest CT reports discrete mediastinal widening predominantly on the right, with diffuse, interstitial infiltrates and consolidation in both posterior segments, more marked at the level of both lung bases (images 1 and 2). Control X-rays at 48 hours showed right basal radiopacity (Image 3). Chest ultrasound was performed, observing pneumonic consolidations and right basal atelectasis. The patient was extubated on the 3rd day without complications, with good evolution. Treatment: Remdesivir 5 mg/kg/day for 5 days, Dexamethasone 0.2 mg/kg/dose every 6 hours for 3 days, mucolytic, gastric protection and antipyretics. Post-extubation, nebulizations with racemic adrenaline 0.5 mL every 12 hours for one day and budesonide 1 mg every 12 hours for two days. As limitations in our health service, we do not have Heliox, nor a respiratory molecular panel. The patient was discharged from the intensive care service, with follow-up by outpatient Pediatrics and Pulmonology.
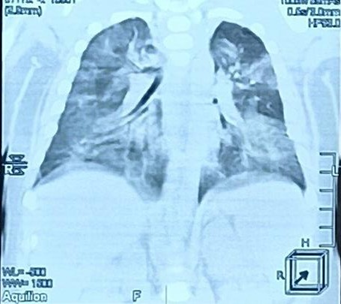
Figure 1: Source: clinical record: predominantly right mediastinal widening with diffuse, interstitial infiltrates is observed.

Figure 2: Source: clinical record (9): adequate expansion of both lung fields with infiltrates and consolidation in both posterior segments is observed.

Figure 3: Source: clinical record (9): note right basal radiopacity
Discussion
The severe cases that have been admitted to our service related to SARS-COV-2 have been due to pneumonia plus ARDS, this being the first case of severe croup reported in our unit. Croup has been a mild entity with a self-limiting evolution, caused by parainfluenza, respiratory syncytial virus and influenza; however, a series of cases have been reported where SARS-COV-2 has been the cause of croup. Although we do not have a molecular respiratory panel in our center, serology for influenza and SARS-COV-2 was performed, the latter being positive. Our patient presented pulmonary involvement, the severity of the condition was associated with croup, however, oxygen requirements were low and mechanical ventilation was quickly withdrawn with the established management for airway edema. Contrary to the 3 cases reported by Schmidt and Mullan (1) where the children presented upper airway symptoms and where only one of them required management in the intensive care room with bilevel positive airway pressure (BiPAP), Pistick et al. reported the case of a 14-month-old infant with inspiratory stridor, who only required observation in the emergency room for 24 hours (7).
Mojtaba and Hosein (6) described the case of a 3-year-old child who, like our patient, presented upper respiratory symptoms that required mechanical ventilation; but in that case, for 17 days, despite having started with typical symptoms of croup, he subsequently developed bacterial tracheitis and generalized convulsions, contrary to the child in our report who only required 3 days with low ventilatory parameters. In the same case reported by Mojtaba and Hosein (6), the minor was managed with nebulizations with racemic adrenaline, as in the cases reported by Schmidt and Mullan (1) where each received multiple doses of nebulized racemic adrenaline (more than 3) with minimal or no improvement of the condition, requiring the use of Dexamethasone for 24-72 hours. In our case, the minor was managed with 2 doses of nebulized racemic adrenaline, and received intravenous Dexamethasone for 3 days. Remdesivir, a drug approved for severely ill children affected by SARS-COV-2, was administered to our patient for 5 days; as in one of the cases reported by Schmidt and Mullan (1) that required admission to the intensive care unit. In the study published in the journal Pediatrics in May 2021, the safety of compassionate use of Remdesivir was investigated in 77 children with severe COVID-19, observing that said medication reduces the need for oxygen ventilatory support, and of the patients who have required mechanical ventilation, 90% have been successfully disconnected (10).
Conclusion
Currently, in the context of the pandemic, SARS-COV-2 must be considered as another causal agent of croup; therefore, patients should be tested for RT-PCR as part of the respiratory panel. Although viral tests are not routinely performed for patients with croup, given that the frequency of viral agents involved in this pathology is already well established, the isolation of SARS-COV-2 should be highlighted as another cause of viral stridor in children, in which the frequency and severity of this symptom has yet to be determined, as well as variants of SARS-COV-2 involved in a faster replication of the virus in the upper respiratory tract, which enables the presentation of stridor; which can manifest itself in a severe form and severely compromise the patient's ventilation. As it is an emerging disease, it is important to characterize the different presentation letters of this infection in the pediatric patient. It is worth mentioning that the cases with which our article was compared do not mention whether there was concomitant pulmonary disease (SARS-COV-2 pneumonia), which our patient did have, since the mixed respiratory failure may not have been entirely caused by croup but by the parenchymal disease, which cannot be ruled out in this patient. Although the presentation of croup was severe, it responded effectively to the traditionally used treatment regardless of the etiology.
Declarations
Conflict of interest
The authors have indicated that they have no potential conflicts of interest to disclose.
Financial disclosure
The authors have indicated that they have no financial relationships relevant to this article to disclose.
References
- Venn A, Schmidt J, Mullan P. (2020). A case series of pediatric croup with COVID-19. American Journal of Emergency Medicine.
Publisher | Google Scholor - Temprano M, Torres M. (2017). Laringitis, crup y estridor. Pediatría Integral, (7):458-464.
Publisher | Google Scholor - Moraa I, et al. (2021). Meta-Analysis. Heliox for croup in children. Cochrane Database Syst Rev.
Publisher | Google Scholor - Cloete H, Kruger A. (2021). Rapid rise in paediatric COVID-19 hospitalizations during the early stages fo the Omicron wave. Tshwane District, South Africa. MedRxiv.
Publisher | Google Scholor - Williams P. (2020). SARS-COV2 in children: spectrum of disease, transmission and immunopathological underpinnings. Focus on SARS-COV2, 52(7):801-808.
Publisher | Google Scholor - Mojtaba K, Hosein S. (2021). Case report: Croup is one of the clinical manifestations of novel coronavirus in children. Hindawi, Case Reports in Pulmonology.
Publisher | Google Scholor - Pitstick C D.O, Rodríguez K MD, Smith A. (2021). A Curious Case of Croup: Laryngotracheitis caused by COVID-19. Pediatrics.
Publisher | Google Scholor - Tunc E, Usoro E. (2022). Pediatric Croup during the COVID-19 Omicron variant surge. MedRxiv. Febrero.
Publisher | Google Scholor - Departamento de Epidemiología. (2022). Instituto Hondureño de Seguridad Social-Hospital Regional del Norte.
Publisher | Google Scholor - Goldma D. Aldrich M. Hagmann S. et al. (2021). Compassionate Use of Remdesivir in Children with Severe COVID-19.
Publisher | Google Scholor












