

Case Report
Bilateral Fused Hips with Stiff Spine in Ankylosing Spondylitis with Sub Trochanteric Fracture Right Hip
1Professor and Head, Unit II, Department of Orthopaedics, Christian Medical College Hospital, Vellore, India.
2Assistant Professor, Department of Orthopaedics, Unit II, Christian Medical College Hospital, Vellore, India.
*Corresponding Author: *Corresponding author: Anil Thomas Oommen.
Citation: Anil T. Oommen, Augustine J. Paul, J. Christo, V.V. Ramu (2024). Bilateral Fused Hips with Stiff Spine in Ankylosing Spondylitis with Sub Trochanteric Fracture Right Hip. Journal of Clinical Rheumatology and Arthritis, BioRes Scientia Publishers. 2(1):1-5. DOI: 10.59657/2993-6977.brs.24.015
Copyright: © 2024 Anil Thomas Oommen, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 24, 2024 | Accepted: May 08, 2024 | Published: May 13, 2024
Abstract
Background: Ankylosing spondylitis (AS) presents with hip and spine stiffness at total hip arthroplasty (THA) with mobility restriction. Reduced spinopelvic mobility is associated with spine stiffness, especially bilateral fused hips.
Case report: We present a rare case of bilateral fused hips due to AS with a traumatic subtrochanteric fracture of the right femur—preoperative planning with anesthetic considerations included risk assessment for bilateral versus unilateral and mobilization after the procedure. Simultaneous bilateral cementless THA using a modified Hardinge approach with modular femoral component (SROM, Depuy USA) to achieve fracture stabilization was done, followed by gradual mobilization. Care was taken to ensure correct femoral and acetabular component positioning, considering spine stiffness and loss of spinopelvic mobility. He is doing well at three years with a stiff spine in extension, walking independently, ability to sit comfortably, and good functional outcome.
Conclusion: Simultaneous bilateral THA had to be considered in this unusual case of AS, although not ideal, with risk consent for achieving mobility following significant stiffness and disability.
Keywords: ankylosing spondylitis (as); stiff hips; subtrochanteric fracture
Introduction
Ankylosing Spondylitis (AS) presents with varying degrees of hip and spine stiffness. The loss of spinal flexibility affects spinopelvic mobility with the coexistence of spine and hip stiffness. Significant spine stiffness is seen at presentation for THA in these individuals with bilateral stiff hips. The risk for fractures in AS has been described [1]. However, subtrochanteric fracture with bilateral fused hips in AS has not been reported. Spinopelvic mobility at THA and acetabular component position is essential to achieve optimal outcomes [2,3]. Cementless THA in AS provides a good outcome. THA restores movement at the hip with significant functional improvement, although the spine stiffness remains unchanged in AS. Informed consent was obtained from the patient.
Case Report
A 45-year-old gentleman with bilateral fused hips and stiff spine with AS presented with a right hip subtrochanteric fracture after a fall at home (Figure 1).
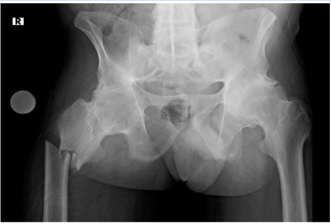
Figure 1: 45 years AS male with bilateral stiff hips and subtrochanteric fracture right femur with stiff spine. The pelvic tilt is posterior with the obturator foramen view suggestive of obliteration of lumbar lordosis which is seen in the follow up x-rays as well.
He had decreased mobility in both hips and spine (Figure 2a, b) before the fall and was walking with a stiff gait pattern. He had complaints of back pain as well as bilateral hip pain with progressive stiffness over the past 20 years. He has been on regular treatment with disease-modifying drugs for the past four years and could walk with stiff hips and spine for about 1 km without pain or discomfort. He was restricted to the bed after a fall two weeks before presentation at our center. His findings revealed significant restriction of movements in the left hip with a flexion deformity of 40 degrees with an external rotation deformity of 30 degrees with a jog of further movement. He was found to have a stiff lumbar and cervical spine both on clinical and radiological examination. His spinopelvic mobility could not be assessed due to his inability to sit or stand after the fracture of the right femur.
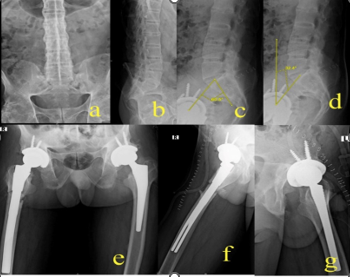
Figure 2 A, B: Lumbosacral (LS) spine AP (anteroposterior) and lateral with typical changes of AS and loss of lumbar lordosis. C, D: Post op standing xrays lateral LS spine showing a pelvic incidence of 60.5 degrees and a pelvic tilt of 32.4 degrees; E, F, G: Post op Xray with long SROM Pinnacle (DePuy, USA) right hip with bone graft and Corail Pinnacle left hip,Anteroposterior and lateral views.
A detailed clinical examination was done before preoperative planning. The stiff cervical spine with a difficult airway, possible anesthetic challenges, and risks versus benefits of staged versus bilateral were considered and discussed with the patient before a decision was made for this challenging situation. The option for internal fixation of the fracture was discussed so that planning for THA could be done after fracture healing. Perioperative care and the need for THA as soon as possible were a source of concern for the patient. He was, however, waiting for a total hip arthroplasty and, after discussion with the family, was very keen to undergo bilateral hip replacement after understanding the possible risks. Blood investigations included total protein of 7.3 g/dl, platelet counts of 304,000/mm3, and total counts of 10,600/mm3; simultaneous bilateral total hip arthroplasty (THA) was carefully planned to facilitate post-op rehabilitation and ambulation and avoid the risks of a subsequent difficult anesthesia [4]. A modified lateral approach was used for both hips [5]. This approach is routine in our unit for all THAs, which do not require posterior reconstruction. Bilateral hip arthritis requiring THA is usually carried out in the same sitting in our unit after a detailed anesthetic evaluation. The preoperative planning included templating and planning for a modular SROM (De Puy, USA ) femur component on the right side and a Cementless Corail (De Puy, USA ) for the left side. Pinnacle (DePuy, USA ) acetabulum was planned for both hips. The right hip procedure was done first with an extension of the modified lateral approach to expose the fracture and stabilize the fragments during femur preparation. The preparation and fixation were similar to subtrochanteric shortening for complex THA described [6]. Femur preparation was done judiciously to achieve optimal sizing and stabilization of the fracture with the modular femoral component. Stable fixation was achieved with a 15x 20 x 225 SROM, 20 B metaphyseal sleeve for the femoral component. Bone grafting was done using bone obtained from the head. The left hip was done in the same sitting with screws used for additional fixation of the cementless acetabular components(Pinnacle, DePuy USA) for both hips(Figure 3 a,b,c.).
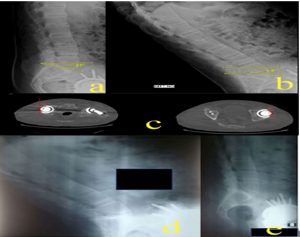
Figure 3 A, B: Post op standing Sacral slope (SS) of 23 degrees compared to sitting SS of 1.8 degrees. The spine extension is obvious at sitting. C: CT evaluation of anteversion both hips measured 12.5 degrees at the right hip and 12.6 degrees at the left hip. D, E: Xray LS spine lateral sitting and standing at follow up showing spine stiffness in extension
Care was taken regarding component positioning to achieve normal acetabular component anteversion. Left hip arthroplasty was carried out after the right hip as the patient was stable throughout the procedure, with an uneventful immediate postoperative period. He was made to sit on the first postoperative day. He was ambulated with protected weight-bearing on the right and could sit comfortably by the end of 1 week. He was ambulating comfortably with a walker, continuing protected weight bearing for 2 months, gradually progressing to full weight-bearing. He was weaned off the walker gradually after six months. The acetabular inclination was 44.7 degrees on the right and 49.6 degrees on the left hip. The spine evaluation was done with radiographs in the sitting and standing position when he could sit comfortably, and the pelvic tilt was calculated (Figure 2 c,d). The sacral tilt showed a 21.2-degree change, while the lumbar lordosis angle changed by only 3.1 degrees between sitting and standing (Figure 4 a-d). The spine stiffness was evident in the sitting position with the extension required to achieve a comfortable sitting position(Figure 4a-d). The anteversion in both the hips was calculated with a CT evaluation. Anteversion of the right acetabular component was 12.6 degrees, and the left acetabulum was 12.5 degrees(Figure 5 a,b). His Harris hip score (HHS) increased from 14 to 83, SF 12 was 54 and 62 for the physical and mental components, respectively, with the WOMAC score of 16 indicating an overall significant improvement in functional outcome [7]. The fracture progressed to complete union with clinical and radiological follow-up. He is ambulating independently at three years with the ability to sit comfortably with spine extension because of the spine stiffness(Figure 6 a,b,c,).
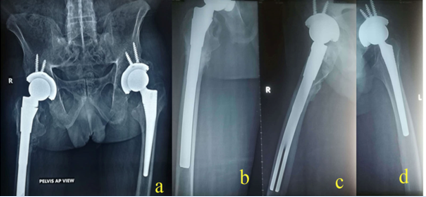
Figure 4a: Xray at 4 months post op showing good progress in union at the right subtrochanteric fracture. b, c:AP and lateral views of the right hip and femur at 1 year with evidence of fracture union, left hip with implants well integrated.
Discussion
Bilateral fused hips in ankylosing spondylitis are disabling and require THA to restore joint mobility. The aim would be to restore the center of rotation and achieve stable fixation with cementless implants in hips with good bone stock. The spine is stiff with the stuck sitting spinopelvic mobility pattern [3,7,8]. This spinopelvic mobility pattern seen with the fused spine in AS requires an extension of the spine to enable a comfortable sitting position with the thighs parallel to the floor. The pelvic incidence and change in sacral tilt were identical at post-op and review with spine stiffness. The pre-op assessment is essential, especially with associated spine stiffness [2,7,8]. Our patient had fused hips for bilateral THA, with a subtrochanteric fracture presenting two weeks after the injury. He was keen to undergo bilateral THA to restore mobility and consented to the same after risk considerations. Bilateral THA was performed after careful planning, although staged THA could have been considered for reduced risk of perioperative complications. The spinopelvic mobility is restricted, and anteversion of the acetabulum needs to be reduced in these fused hips to avoid posterior impingement and anterior dislocation [3,10]. THA in AS has associated risks including late dislocation, which must be considered when planning for the same [11].
A proximal femur fracture with a fused hip poses a challenging situation for THA [12]. The subtrochanteric fracture stabilization and hip arthroplasty were performed using the SROM (DePuy USA) femoral component. Femur fracture with bilateral fused hips in ankylosing spondylitis has not been reported. The risk of fracture in ankylosing spondylitis exists in the hip and the vertebrae [1].
Bilateral fused hips with bony ankylosis have a severe restriction of daily activity. The mobility is significantly reduced, and the spinopelvic mobility is also affected. The spine was fused, as evidenced by the preop and post-op spine x-rays. The loss of spinopelvic mobility is like a stuck sitting pattern. Movements are restricted to walking with a stiff spine and hips and lying supine. Osteosynthesis for the fracture was considered; however, the individual who was preparing for hip arthroplasty was not keen and wanted to go ahead with arthroplasty, being aware of the possible risks. Fracture stabilization and mobility of the hip joints were achieved at THA with a long modular stem. Fracture stability was achieved, enabling gradual mobilization. The mobility, as well as weight-bearing, was gradually increased based on the clinical and radiological union. The acetabular component positioning was done with care to avoid increased anteversion, compensate for the change in spinopelvic mobility, avoid impingement, and provide a stable functional hip joint. Our patient is comfortable with the ability to walk, sit, and stand comfortably, having residual spine stiffness with spine extension to enable sitting with the thighs parallel to the floor. This pattern of spine stiffness is seen especially in AS, with movement occurring predominantly only at the hips after THA in these stiff individuals.
Conclusion
Bilateral fused hips with subtrochanteric fracture and spine stiffness have not been reported so far. Fracture stability with the restoration of joint mobility is justified in this unusual case of AS with stiff hips and spine and associated subtrochanteric fracture. Fixation and THA with the restoration of joint mobility were achieved with an extended modular femoral component. Bilateral THA, rather than staged THA, although not ideal, was carried out in this unusual case to facilitate early mobilization after carefully considering risks, spinopelvic mobility, and perioperative care. The overall functional outcome has significantly improved, and he is doing well at three years follow up.
Declarations
Acknowledgment
Not applicable.
Conflict of interest
Nil
Declaration of competing interest
Nil
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of funding
None.
References
- Zhang M, Li XM, Wang GS, Tao JH, Chen Z, et al. (2017). The association between ankylosing spondylitis and the risk of any, hip, or vertebral fracture: A meta-analysis. Medicine (Baltimore), 96(50):8458.
Publisher | Google Scholor - Stefl M, Lundergan W, Heckmann N, McKnight B, Ike H. et al. (2017). Spinopelvic mobility and acetabular component position for total hip arthroplasty. Bone Joint J, 99(1):37-45.
Publisher | Google Scholor - Lum ZC, Coury JG, Cohen JL, Dorr LD. (2018). The Current Knowledge on Spinopelvic Mobility. J Arthroplasty, 33(1):291-296.
Publisher | Google Scholor - Lin D, Charalambous A, Hanna SA. (2019). Bilateral total hip arthroplasty in ankylosing spondylitis: a systematic review. EFORT Open Rev, 4(7):476-481.
Publisher | Google Scholor - Mulliken BD, Rorabeck CH, Bourne RB, Nayak N. (1998). A modified direct lateral approach in total hip arthroplasty: a comprehensive review. J Arthroplasty, 13(7):737-747.
Publisher | Google Scholor - Oommen AT, Chandy VJ, Jeyaraj C, Kandagaddala M, Hariharan TD. et al. (2020). Subtrochanteric femoral shortening for hip centre restoration in complex total hip arthroplasty with functional outcome. Bone Jt Open, 1(5):152-159.
Publisher | Google Scholor - Innmann MM, Merle C, Gotterbarm T, Ewerbeck V, Beaulé PE. et.al. (2019). Can spinopelvic mobility be predicted in patients awaiting total hip arthroplasty? A prospective, diagnostic study of patients with end-stage hip osteoarthritis. Bone Joint J, 101-(8):902-909.
Publisher | Google Scholor - Innmann MM, Merle C, Phan P, Beaulé PE, Grammatopoulos G. (2020). How Can Patients with Mobile Hips and Stiff Lumbar Spines Be Identified Prior to Total Hip Arthroplasty? A Prospective, Diagnostic Cohort Study. The Journal of Arthroplasty, 35(6):255-261.
Publisher | Google Scholor - Luthringer TA, Vigdorchik JM. (2020). A Preoperative Workup of a “Hip-Spine” Total Hip Arthroplasty Patient: A Simplified Approach to a Complex Problem. J Arthroplasty, 34(7):57-70.
Publisher | Google Scholor - Heckmann N, McKnight B, Stefl M, Trasolini NA, Ike H. et.al. (2018). Late Dislocation Following Total Hip Arthroplasty: Spinopelvic Imbalance as a Causative Factor. J Bone Joint Surg Am, 100(21):1845-1853.
Publisher | Google Scholor - Blizzard DJ, Penrose CT, Sheets CZ, Seyler TM, Bolognesi MP.et.al. (2017). Ankylosing Spondylitis Increases Perioperative and Postoperative Complications After Total Hip Arthroplasty. J Arthroplasty, 32(8):2474-2479.
Publisher | Google Scholor - Malhotra R, Khurana A, Shekhar S, Gautam D. (2020). Proximal femoral fracture in ankylosed hip treated with primary total hip arthroplasty: Technical tips with report of two cases. J Clin Orthop Trauma, 11(1):99-104.
Publisher | Google Scholor













