

Review Article
Adoption of Personalized and Precision Medicine (PPM)-Guided Resources in addressing Clinical Oncology Practice-Related Needs
- Sergey Suchkov 1-6*
- Daniel Scherman 11
- Shawn Murphy 7,8
- David Smith 10
- Michael J. Duffy 13,14
- Hiroyuki Abe 5,9
- Lidiya Kadyrova 15
- R. Holland Cheng 12
1The Russian University of Medicine, Moscow, Russia.
2The Russian Academy of Natural Sciences, Moscow, Russia.
3EPMA, Brussels, EU.
4PMC, Washington, DC, USA.
5ISPM, Tokyo, Japan.
6AHA, Houston, TX, USA.
7MGH, Boston, MA, USA.
8Harvard Medical School, Boston, MA, USA.
9Abe Cancer Clinic, Tokyo, Japan.
10Mayo Clinic, Rochester, MN, USA.
11Member of the European Academy of Sciences, Head of the Division Medicine and Life Sciences, Paris, France.
12UC Davis, St Davis, CA, USA, USA.
13UCD Clinical Research Centre, St Vincent’s University Hospital, Dublin 4, Ireland.
14UCD School of Medicine and Medical Science, University College Dublin, Dublin 4, Ireland.
15Department of Neurophysiology of Kazan State Medical Academy, Russia.
*Corresponding Author: Sergey Suchkov, The Russian University of Medicine, Moscow, Russia
Citation: Suchkov S, Scherman D, Murphy S, Smith D, Duffy M J, et al. (2024). Adoption of Personalized and Precision Medicine (PPM)-guided Resources in addressing Clinical Oncology Practice-Related Needs. Journal of Cancer Management and Research, BioRes Scientia publishers. 2(2):1-22. DOI: 10.59657/2996-4563.brs.24.013
Copyright: © 2024 Sergey Suchkov, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 28, 2024 | Accepted: May 03, 2024 | Published: June 10, 2024
Abstract
PPM is now the recommended standard for oncology care. Individualizing treatment is thus becoming a core objective of the personalized and precision medicine (PPM), and its valuable branch, entitled as Personalized & Precision Oncology/PPO). PPO is emerging as a complementary approach that aims to bridge the gap between genotype and phenotype by modelling individual tumors in vitro. Those patient- and pre-cancer person-at-risk-derived ex vivo models largely preserve several tumor characteristics that are not captured by genomics approaches and enable the functional dissection of tumor vulnerabilities in a PPM-guided manner. Those trends and developments have opened exciting new avenues for PPO-guided clinical practice, with the potential for successful applications in contexts in which genomic data alone are not informative.
Keywords: adoption; personalized and precision medicine; clinical oncology; genomics; phenomics
Introduction: Annotation
PPM is now the recommended standard for oncology care. Individualizing treatment is thus becoming a core objective of the personalized and precision medicine (PPM), and its valuable branch, entitled as Personalized & Precision Oncology/PPO). PPO is emerging as a complementary approach that aims to bridge the gap between genotype and phenotype by modelling individual tumors in vitro. Those patient- and pre-cancer person-at-risk-derived ex vivo models largely preserve several tumor characteristics that are not captured by genomics approaches and enable the functional dissection of tumor vulnerabilities in a PPM-guided manner. Those trends and developments have opened exciting new avenues for PPO-guided clinical practice, with the potential for successful applications in contexts in which genomic data alone are not informative. To really understand PPO, we would have to understand the various fields of translational applications that provide the tools to exploit and practice PPO, and genomics- and phenomics-related tools, in particular! So, PPM and PPO along with the “OMICS-guided” diagnostic, predictive, prognostic and therapeutic manipulatios are expressions used for this paradigm shift often interchangeably [17-31].
The uptake of PPM, while advancing in cancer care, has faced several adoption challenges, including education, policy, and practical factors. For instance, personalized cancer treatment in particular stands to highly benefit from PPO-driven therapies, since extensive variability between tumors presents a need to target each case in a personalized manner. At this point, personalized cancer therapy is considered to be a treatment strategy centered on the ability to predict which patients are more likely to respond to specific cancer therapies. This approach is founded upon the idea that cancer biomarkers are associated with patient prognosis and tumor response to therapy. And personalized tumor molecular profiles (tumor biomarkers can be OMICS-profiles that predict therapy response) tumor disease site and other characteristics are then potentially used for determining optimum individualized therapy options (18-31]. Improved cancer patient (or pre-cancer person-at-risk) outcomes with the application of the biomarker tests must consider not only increased survival or quality of life, but also improved clinical decision support (CDS) & making leading to the avoidance of unnecessary therapy or toxicity. So, bioinformatics, artificial intelligence (AI), machine learning (ML) and biostatistics will be crucial in translating those Big Data into useful clinical and pre-clinical applications, leading to improved diagnosis, prediction, prognostication and treatment [32-37].
The EDITORIAL describes along modern modes and technologies of diagnostics, translational cancer therapeutics and the way forward from clinical and molecular diagnosis to treatment. Also, the Review concerns the role of bioinformatics and biostatistics, considering the Big Data analysis serving PPM and PPO approaches. Facilitating the transformation toward PPM that will improve patient outcomes in the oncology setting requires a coordinated effort among policymakers, cancer agencies, health systems, and industry. To implement PPM effectively in cancer practice requires an informatics solution beyond the legacy electronic medical record platforms currently available to clinical teams. Therefore, the proposed EDITORIAL demonstrates the successful evidence for the use of PPM-driven resources in the treatment of cancer and its future clinical perspectives as PPO-driven trends. The latter fills the gaps in cancer biology and oncology with its up-to-date content and well-designed sections. It will serve as a valuable resource for biodesigners, general practitioners, oncologists, medical students, and interdisciplinary researchers. And the concept of PPM and PPO as its branch appear to hold promising results, having potential benefits for the effectiveness of care, new disease taxonomy, and population healthcare as a whole.
The Introductory comments
Contemporary views of human disease (including cancer) and thus modern medicine, clinical oncology and healthcare are based on simple correlation between clinical syndromes, pathological analysis and data rooted in the latest research and applications. In this context, the link that might exert reliable control over morbidity, mortality and disabling rates and to thus improve the healthcare services and to significantly optimize the efficacy of treatment for those who had fallen ill (patients) and for persons-at-risk is Personalized & Precision Medicine (PPM) (Fig. 1).
Figure 1: Personalized & precision medicine (PPM) as a Model of Healthcare Services of the Next-Step Generation
PPM refers to the tailoring of diagnostics or therapeutics to individual patients based on their unique genetic and physiologic characteristics. Although “personalized or individualized care” (i.e., tailoring investigations and therapies to each patient) has long been the hallmark of good clinical care, more recently, an emphasis on genomics, proteomics and other biologic omics platforms has come to be understood to underpin personalized care. Personalized medicine takes these differences and implements preventions/treatments tailored to the individual. Precision medicine identifies differences in individuals, categorizing based on environmental, biological, and psychosocial factors.
PPM is one of the most promising approaches to tackling diseases that have thus far eluded effective treatments or cures. In particular, cancer, takes an enormous toll on individuals, families and societies as a whole. An example of current personalized care is the use of biomarkers and targets to better delineate disease subtype, define prognosis or to inform therapy decisions. With regard to cancer, PPM most often means looking at how changes in certain genes or proteins in a person’s cancer cells might affect their care, such as their treatment options. PPM holds promise for better personalization of care in the future. To achieve further improvements in health care, progress on all of those fronts needs to continue, not just in OMICS-based PPM [16,38].
PPM uses a patient’s genetic profile to guide decisions about disease prevention, diagnosis, and treatment. That is GENES, GENOME CLUSTERS and GENOME LANDSCAPES are really the core of PPM being assessed and analyzed by diagnostic, predictive and prognostic analytics tools, on one hand and presented to the practitioners, on the other one. PPM as being the Grand Challenge to forecast, to predict and to prevent is rooted in a big and a new science generated by the achievements of systems biology [39-47] (Fig. 2A, B).
Systems Biology
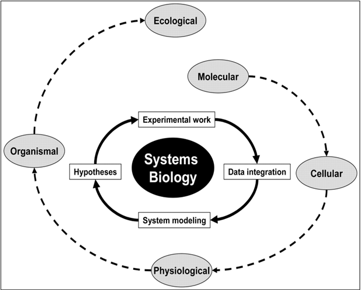
Figure 2A: Systems Biology in theory
Systems biology is a comprehensive quantitative analysis of the manner in which all the components of a biological system interact functionally over time. Systems biology is a field of research that focuses on understanding whole biological systems, such as protein complexes, metabolic pathways, or gene regulatory networks, and it attempts to understand cells, tissues, and organisms and how they behave and function from a systems perspective. Systems biology is an integrative discipline connecting the molecular components within a single biological scale and also among different scales (e.g., cells, tissues and organ systems) to physiological functions and organismal phenotypes through quantitative reasoning, computational models and high-throughput experimental technologies. In other words, systems biology is a computational and mathematical analysis and modeling of complex biological systems, and a systemic view of biological issues means that the function of no organ is independent of the other so that the behavior of all components will affect the behavior of the whole system.
The masses of data generated by high-throughput technologies are challenging to manage, visualize, and convert to the knowledge required to improve patient (including cancer patient and pre-cancer person-at-risk) outcomes. Systems biology integrates engineering, physics, and mathematical approaches with biologic and medical insights in an iterative process to visualize the interconnected events within a cell that determine how inputs from the environment and the network rewiring that occurs due to the genomic aberrations acquired by patient tumors determines cellular behavior and patient outcomes. A cross-disciplinary systems biology effort will be necessary to convert the information contained in multidimensional data sets into useful specific (including cancer) biomarkers that can classify patient tumors by prognosis and response to therapeutic modalities and to identify the drivers of tumor behavior that are optimal targets for cancer therapy. An understanding of the effects of targeted therapeutics on signaling networks and homeostatic regulatory loops will be necessary to prevent inadvertent effects as well as to develop rational combinatorial therapies. Systems biology approaches identifying molecular drivers and biomarkers will lead to the implementation of smaller, shorter, cheaper, and individualized clinical trials that will increase the success rate and hasten the implementation of effective therapies into the clinical armamentarium [39-44].
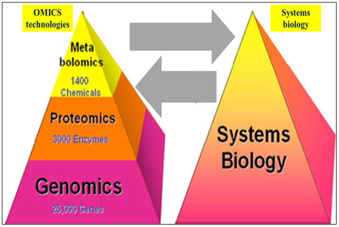
Figure 2B: Systems Biology in action
The goal of systems biology is to discover new emergent properties in order to better understand the entirety of processes that happen in a biological system. In this model, biology dictates what new technology and computational tools should be developed, and, once developed, these tools open new frontiers in biology for exploration. Thus, biology drives technology and computation, and, in turn, technology and computation revolutionize biology. Some of the areas of study are listed below, along with the associated 'OMICS. Globally, systems biology combines: genomics, proteins, metabolomics. Systems biology uses a wide range of quantitative experimental and computational methodologies to decode information flow from genes, proteins and other subcellular components of signaling, regulatory and functional pathways to control cell, tissue, organ and organismal level functions. The computational methods used in systems biology provide systems-level insights to understand interactions and dynamics at various scales, within cells, tissues, organs and organisms. In recent years, the systems biology framework has enabled research in quantitative and systems pharmacology and precision medicine for complex diseases. Systems biology is actively transforming the field of modern health care from symptom-based disease diagnosis and treatment to precision medicine in which patients are treated based on their individual characteristics. Development of high-throughput technologies such as high-throughout sequencing and mass spectrometry has enabled scientists and clinicians to examine genomes, transcriptomes, proteomes, metabolomes, and other omics information in unprecedented detail. This “omics” information leads to a global profiling of health and disease, and providing new approaches for personalized health monitoring and preventative medicine [48-51].
Integrative Medicine
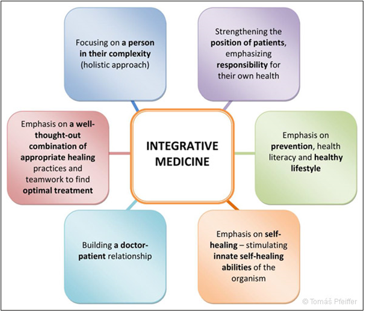
Figure 2C: Integrative medicine
Integrative medicine, as defined by the American Board of Integrative Medicine® (ABOIM) and the Consortium of Academic Health Centers for Integrative Medicine, is the practice of medicine that reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic approaches, healthcare professionals, and disciplines to achieve optimal health and healing. Integrative health and medicine have emerged as a movement that focuses on the whole person, considering the individual in its physical, psychological, spiritual, social and environmental context, and is inclusive of all professions and practices that use this approach. Integrative health and medicine stand for an evidence-informed integration of conventional biomedicine with traditional and complementary medicine (T&CM). All appropriate therapeutic approaches and healthcare disciplines are used to achieve optimal health and healing, while recognizing and respecting the unique contribution from many medical systems [52,53].
Biodesign-Driven Translational Research & Applications
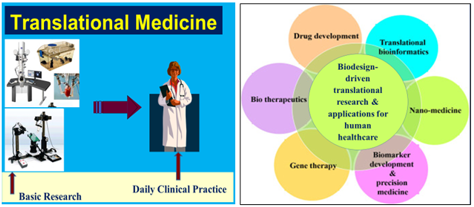
Figure 2D, E: Modern approaches towards biomedical translation: predicting translational progress in biomedical research & applications
The impact of systems biology & fundamental biological discoveries is not reaching the clinical setting at a pace that was expected. In order to bridge this gap, the focus of biomedical researchers has shifted from OMICS-driven discoveries to “translating” only clinically relevant biological information. The change in focus has redirected the field of design-driven biotechnology toward what “translational research,” which is the buzzword of the era. By definition, translational & applications are “an interdisciplinary branch of the biomedical field supported by three main pillars: bench-side, bedside, and community,” Stemming from translational biotechnology came system biology, bioengineering, and so on. Combining such biomedical information from different layers of OMICS-data can ultimately help us in revealing the landscape of molecular mechanisms involved in highly prevalent complex diseases like cancer.
Translational medicine (also referred to as translational science) is a discipline within biomedical and public health research that aims to improve the health of individuals and the community by “translating” findings into diagnostic tools, medicines, procedures, policies and education. Translational medicine, area of research that aims to improve human health and longevity by determining the relevance to human disease of novel discoveries in the biological sciences. Translational medicine seeks to coordinate the use of new knowledge in clinical practice and to incorporate clinical observations and questions into scientific hypotheses in the laboratory. Thus, it is a bidirectional concept, encompassing so-called bench-to-bedside factors, which aim to increase the efficiency by which new therapeutic strategies developed through basic research are tested clinically, and bedside-to-bench factors, which provide feedback about the applications of new treatments and how they can be improved. Translational medicine facilitates the characterization of disease processes and the generation of novel hypotheses based on direct human observation [54-56].
Whilst integrating platforms of OMICS-technologies
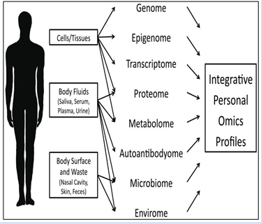
Figure 3B: Integrative Personal OMICS Profile Analysis (Multi-OMICS profiling)
Various types of systems data can be generated and integrated with the multi-OMICS integrative analysis. Multiomics is a new approach where the data sets of different OMICS groups are combined during analysis. The different OMICS strategies employed during multiomics are genome, proteome, transcriptome, epigenome, and microbiome. Development of high-throughput technologies such as sequencing and mass spectrometry has enabled scientists and clinicians to examine genomes, transcriptomes, proteomes, metabolomes, and other omics information in unprecedented detail. This “omics” information leads to a global profiling of health and disease, and providing new approaches for personalized health monitoring and preventative medicine. This approach is highly modular and can be tailored to meet specific needs of different studies [19-31, 57-59]. whose data is analyzed, integrated, mined and clinically interpreted by a set of algorithms and software of bioinformatics (Fig. 4A, B).

Figure 4A, B: PPM informatics & Big Data analytics
(G) Classification of enabling tools and techniques in three areas of PPM-driven informatics: clinical informatics, biomedical informatics, and participatory health informatics.
(H) Integrated Big Data accumulated from a variety of PPM-dependent sources, including OMICS data, social & behavioral data, environmental data and personal client data (including EMRs and disease story).
Nowadays, the increasing availability of OMICS and related data, due to both the advancements in the acquisition of translational application results and in systems biology simulation technologies, provides the bases for PPM. Success in PPM depends on the access to healthcare and biomedical data. To this end, the digitization of all clinical exams and medical records is becoming a standard in hospitals. The digitization is essential to collect, share, and aggregate large volumes of heterogeneous data to support the discovery of hidden patterns with the aim to define predictive models for biomedical purposes. Patients’ data sharing is a critical process. In fact, it raises ethical, social, legal, and technological issues that must be properly addressed. Meanwhile, fragmentation and heterogeneity of available data makes it challenging to readily obtain first-hand information regarding some particular diseases, drugs, genes and variants of interest. So, both medical professionals and IT experts across the globe have started to device computational infrastructural solutions to address the need of timely and precise decision on a patient health issue. It is a high time for both the informatics community and the medical community to collaborate with each other to make a combine effort for achieving the common goal of a better-quality patient care. To understand the IT-related viewpoint of how the PPM is implemented, we provided an overview of enabling tools and techniques in three potential areas: biomedical informatics, clinical informatics, and participatory health informatics. The integration of heterogeneous data sources allows to lay the foundations for a series of statistical assessments needed to answer more complex questions that can be used in a variety of fields, such as predictive and precision medicine. In particular, studying the clinical history of patients who have developed similar pathologies we could allow to predict or individuate marks allowing early diagnosis of possible illnesses [60-63]. Well, PPM is a goal of upgraded healthcare of the nearest future to come, in which diagnostic and treatment decisions are informed by each person's unique clinical, OMICS-based, healthcare bureaucracy (medical records, etc) (Fig. 5) and environmental (exposomics-related) (Fig. 6) information.

Figure 5: Electronic and Sensory Health Records in Clinical Practice and Health Management
Health care informatics focuses on collecting, using, and analyzing data and refers to using data and information technology to improve clinical outcomes and improve both the patient and provider experience. The new applications of public health informatics contribute to more timely and accurate data for disease surveillance. Examples include electronic laboratory reporting of notifiable diseases, aided by new data transmission standards and vocabularies; personal digital assistants or handheld computers to collect data in the field that can be downloaded into a database with no further data entry requirements; geographic information systems integrated with satellite images to provide information about the spread of diseases; use of mobile telephones to report surveillance data from the field; and use of the Internet as an effective way to share surveillance data with health care professionals [64-66].Figure 6: Exposome-driven human health
Human health is determined by the interaction of our environment with the genome and microbiome, which shape the transcriptomic, proteomic, and metabolomic landscape of cells and tissues. Precision environmental health is an emerging field leveraging environmental and system-level (‘omic) data to understand underlying environmental causes of disease, identify biomarkers of exposure and response, and develop new prevention and intervention strategies. The exposome is defined as the totality of internal and external exposures across the lifespan and their health effects. The external exposome includes diet, nutrients, water, chemicals, pollutants, toxins, and other environmental and geospatial exposures. The internal exposome can be measured by untargeted metabolomics, encompassing the small metabolites resulting from all the metabolic processes. Expo omics intended to give a better account of the complex relationships between genes and environmental factors. As a complement to OMICS data, studies on drug-exposome interactions holds immense potential to elevate PPM to an unprecedented level [64-67].
As you might see from the above-mentioned, PPM is a form of the upgraded healthcare services that recognizes that individuals with the same condition may have different underlying factors and uses molecular information to provide tailored treatments. This approach can improve treatment outcomes and transform lives through favorable risk/benefit ratios, avoidance of ineffective interventions, and possible cost savings, as evidenced in the field of cancer and other oncology/therapeutic settings. However, the potential benefits of PPM and thus PPO have yet to be fully realized. The global goal of PPM is to combine current medicine with molecular breakthroughs to target patients individually and increase the efficacy and effectiveness of the therapeutic strategy. Meanwhile, to secure therapeutic targeting which is crucially important and valuable for the latter, whilst implementing the key PPM-related resources into clinical practice, there is a strong need to develop a principally new approach based on biomarkers-driven targeting aimed at subclinical and/or predictive recognition of biomarkers long before the illness (e.g., cancer) clinically manifests itself [68-74] (Fig. 7).

Figure 7: Disease Pathway Biomarkers
Molecular pathway maps indicate involvement of multiple molecular mechanisms, and selected biomarker candidates re-ported as associated with disease progression are identified for specific molecular processes and disease-related stages, including risk factors, screening and diagnosis, and prognosis covering the induction stage, latency (subclinical or pre-illness) and clinical manifestations [74-78]. This new biomarker-driven diagnostic and monitoring technology will create a full digital fingerprint of patient samples that will be able to connect genotype, phenotype, diagnosis, treatment, and outcome at the molecular level. Meanwhile, in PPO, one of the ways to improve the specificity is to move from a single to multiplex biomarkers, which can additionally provide significantly increased diagnostic, predictive and prognostic accuracy. Such multiplex biomarkers should include information from each level of systems biology bridging genomics, transcriptomics, proteomics and metabolomics. This approach would give a real opportunity to secure diagnostic, predictive, and prognostic manipulations (Fig. 8).
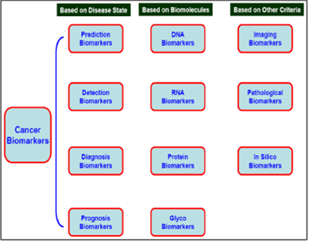
Figure 8: Various roles of biomarkers in cancer treatment
Cancer biomarkers are categorized into several segments based on their utility in various steps of oncology practice, including: (i) diagnostic: for a confirmed diagnosis of cancer and its extent (are also useful to differentiate between the types of tumors like benign or metastatic tumors, primary or secondary site tumors, etc.); (ii) prognostic: (help determine the aggressiveness of the detected tumor and how the tumor will respond to the selected therapy - helps physicians to plan and design a proper regimen for the patient); (iii) predictive: help in the screening of cancer in a healthy patient, and also could predict the risk of getting cancer in the future; (iv) pharmacodynamics: the circulating biomarkers access the drug response like its metabolism and deposition in the body during a treatment course, whilst helping to understand the optimum effective dose of the drug; (v) recurrence: are useful in predicting the recurrence of disease in patients who have undergone treatment and recovered from cancer - periodic screening using assays of the biomarkers helps understand the chances of disease recurrence; (vi) monitoring: the response of treatment cycles in killing tumor cells -it helps to treat physicians to design future treatment goals [78-81].
This new biomarker-driven diagnostic and monitoring technology will create a full digital fingerprint of patient samples that will be able to connect genotype, phenotype, diagnosis, treatment, and outcome at the molecular level. Meanwhile, in PPO, one of the ways to improve the specificity is to move from a single to multiplex biomarkers, which can additionally provide significantly increased diagnostic, predictive and prognostic accuracy. Such multiplex biomarkers should include information from each level of systems biology bridging genomics, transcriptomics, proteomics and metabolomics. This approach would give a real opportunity to secure diagnostic, predictive, and prognostic manipulations [82-87] (Fig. 9).
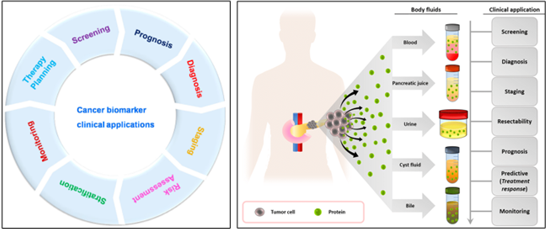
Figure 9: Cancer biomarker and their clinical applications
Cancer biomarkers are the key to unlocking the promise of PPO, selecting which patients will respond to a more personalized treatment while sparing non-responders the therapy-related toxicity. In cancer, a biomarker refers to a substance or process that is indicative of the presence of cancer in the body. A biomarker might be either a molecule secreted by a tumor or it can be a specific response of the body to the presence of cancer. Genetic, epigenetic, proteomic, and imaging biomarkers can be used for cancer diagnosis, prognosis and epidemiology. Cancer biomarkers must be embedded in the real world of oncology delivery. Cancer biomarkers belong to a variety of bio elements such as DNA, mRNAs, proteins, lnc RNAs, miRNAs, exosomes, cellular metabolites, and organic materials. Cancer patients and pre-cancer persons-at-risk must be placed firmly at the center of a cancer biomarker informed PPO-driven care agenda [88-93]. In this context, cancer biomarkers are any measurable molecular indicator of risk of cancer, occurrence of cancer, or patient outcome. They may include germline or somatic genetic variants, epigenetic signatures, transcriptional changes, and proteomic signatures. These indicators are based on biomolecules, such as nucleic acids and proteins, that can be detected in samples obtained from tissues through tumor biopsy or, more easily and non-invasively, from blood (or serum or plasma), saliva, buccal swabs, stool, urine, etc. And thousands of species of RNAs, proteins, and metabolites are suggested as candidate tumor biomarkers alone or as constituents of multiplex signatures. If the patient is already diagnosed with a certain cancer, RNA or protein biomarker signatures may help to select a specific therapy or to predict the probability of a relapse. Meanwhile, detection technologies have advanced tremendously over the last decades, including techniques such as next-generation sequencing, nanotechnology, or methods to study circulating tumor DNA/RNA or exosomes.
Clinical applications of biomarkers are extensive: much of the current PPM-related designed testing platforms are focused on the identification of protein biomarkers, which are distinct from genetic ones. They can be used as tools for cancer risk assessment, screening and early detection of cancer, accurate diagnosis, patient prognosis, prediction of response to therapy, and cancer surveillance and monitoring response. They have the advantage that they make up the actual molecular phenotype of disease, as they are at the end of the DNA-to-RNA-to-protein progression from genotype to phenotype [94-99]. In this context, novel technologies such as liquid biopsy and companion diagnostics (theranostics) accompanied evolving trends in PPO and prognostic and predictive markers such as minimal residual disease [100-102]. Therefore, they can help to optimize making decisions in clinical practice. Moreover, PPO is needed for newly developed targeted therapies, as they are functional only in patients with specific cancer genetic mutations, and biomarkers are the tools used for the identification of these subsets of patients. So, PPO emerged as a new field encompassing small molecular inhibitors and biologics.
Cancer is a multifaceted and complex disease that results from the disruption of genetic, epigenetic, and metabolic systems responsible for maintaining physiological conditions in the cell. And thus, cancer is characterized by uncontrollable overgrowth of usually one particular cell type, which becomes a cancer cell, and by spreading of these cancer cells to lymph nodes and other organs of the body, what is called metastatic disease. So, cancer heterogeneity provides a formidable obstacle to optimizing clinical protocols to achieve durable clinical responses. And the absence of reliable cancer-related biomarkers for the pre-early (subclinical) detection and progression monitoring results in the generation of complex cancer-related molecular pathways negatively impact anticancer immune-mediated responses. As a result, immunotherapy-based therapeutic modalities alone or in combination with other standard or targeted therapies provide limited clinical benefits for patients. Therefore, it is imperative to discover biomarkers suitable for selecting patients most likely to benefit from therapies [103-111]. Biomarkers are crucial for identifying the patients who are expected to derive greatest advantage from canonical targeted therapy, and pre-cancer persons-at-risk who do need a special approach, including preventive therapeutic modes. In case of cancer, tumor microenvironment plays a crucial role in the process of growth and spreading of cancer cells in the body. In this context, PPO describes a diverse set of strategies in cancer medicine tailored to the unique biology of a patient’s disease. This design of destroying cancer cells while leaving normal cells intact rapidly expanded to most of tumor types. And strategies range from the use of targeted and/or smart therapies to the use of data from genomic profiling to select treatments independent of cancer type and its microenvironment, and hence go beyond traditional organ-based oncology [112-119].
So, cancer biomarkers are the key to unlocking the promise of PPO-guided trends, selecting which patients or pre-cancer persons-at-risk will respond to a more personalized treatment while sparing non-responders the therapy-related toxicity. We do emphasize the need for cancer biomarkers infrastructure to be embedded into PPM-driven and PPO-guided health systems of the next step generations. Cancer biomarkers must be embedded in the real world of PPO-guided delivery and testing must be implemented across the civilized medical systems, with the intended aim of narrowing, not widening the inequity gap for patients. And PPO is thus mostly based on the high-throughput molecular profiling of tumors which allows for the identification of genomic modifications spotlighting appropriate research and therapeutic targeting. A comprehensive understanding of the landscape of genetic alterations in tumors will certainly further advance our understanding of the dynamic interactions between tumor cells and immune subpopulations, resulting in the development of rational combinatorial therapies. In clinical settings, we need to timely model clinical and multi-OMICS data to find statistical patterns across millions of features to identify underlying cancer-related biologic pathways, modifiable cancer risk factors, and actionable information that support early detection and prevention of cancer and pre-cancer conditions, and development of new therapies for better cancer patient care and pre-cancer prevention. Moreover, we are witnessing the transition toward understanding cancer as a continuum by capturing spatial and temporal tumor heterogeneity [107-109, 120-127] (Fig. 10).
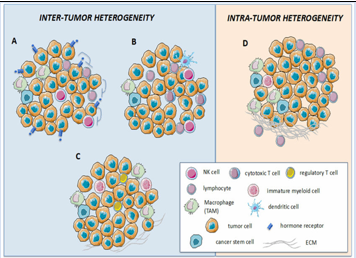
Figure 10: Inter-and intra-tumor heterogeneity dictates the response to HER2-targeted therapies
HER2+ breast cancers are characterized by a high degree of inter-(A-C) and intra-(D) tumor heterogeneity, both contributing to shaping the response to HER2-directed therapies. In the case of inter-tumor heterogeneity, differences may be detected at the level of tumor cells, such as the expression of an estrogen receptor (ER, panel A) that, upon HER2 inhibition, functions as an escape/survival pathway. Additionally, intra-tumor heterogeneity may rely on the different immune cell infiltration that may be enriched in effector T and NK cells, leading to a good response to treatment (panel B), or in immune-suppressive cells, such as T regulatory cells and tumor associate macrophages (TAMs), leading to poor response (panel C). Heterogeneity may also be detected among different regions of the same tumor, with specific areas enriched in the extracellular matrix and TAM/myeloid cells that support the development of micro-niches favoring the selection of resistant neoplastic clones (panel D).
Tumor heterogeneity is regarded as a major obstacle to successful PPM and PPO. The lack of reliable response assays reflective of in vivo tumor heterogeneity and associated resistance mechanisms hampers identification of reliable biomarkers. By contrast, oncogene addiction and paracrine signaling enable systemic responses despite tumor heterogeneity. This strengthens researchers in their efforts towards PPO. Given the fact that tumor heterogeneity is an integral part of cancer evolution, diagnostic tools need to be developed in order to better understand the dynamics within a tumor. Ultra-deep sequencing may reveal future resistant clones within a (liquid) tumor biopsy. On-treatment biopsies may provide insight into intrinsic or acquired drug resistance. Subsequently, upfront combinatorial treatment or sequential therapy strategies may forestall drug resistance and improve patient outcome. Finally, innovative response assays, such as organoid cultures or patient-derived tumor xenografts, provide an extra dimension to correlate molecular profiles with drug efficacy and control cancer growth.
During the course of disease, cancers generally become more heterogeneous. As a result of this heterogeneity, the bulk tumor might include a diverse collection of cells harboring distinct molecular signatures with differential levels of sensitivity to treatment. This heterogeneity might result in a non-uniform distribution of genetically distinct tumor-cell subpopulations across and within disease sites (spatial heterogeneity) or temporal variations in the molecular makeup of cancer cells (temporal heterogeneity). Heterogeneity provides the fuel for resistance; therefore, an accurate assessment of tumor heterogeneity is essential for the development of effective therapies. Multi-region sequencing, single-cell sequencing, analysis of autopsy samples, and longitudinal analysis of liquid biopsy samples are all emerging technologies with considerable potential to dissect the complex clonal architecture of cancers. In this Editorial, we discuss the driving forces behind intra-tumoral heterogeneity and the current approaches used to combat this heterogeneity and its consequences. We also explore how clinical assessments of tumor heterogeneity might facilitate the development of more-effective personalized therapies [128-130]. By integrating multiple data sources (multi-OMICS), each case of cancer can be approached as if it represents a separate disease. The notion of PPO takes on new meanings as new levels of data are added to the understanding of cancer, from complex biological, digital, clinical, behavioral, and environmental data.
Cancer induction and progression through the vies of PPO start from the symptoms and everything that can be seen with the doctor’s naked eye, and the resolution increases through the development of microscopy, biochemistry, cell biology, and the birth of pharmacogenetics. And the cancer-related disorder begins to be reclassified starting from molecules to symptoms; it is the stage in which the notions of biomarkers and targeted therapies gain momentum. Precision in this period is based on deciphering the structure of DNA and the early stages of biotechnology development. Later, PPO is dominated by the development of high-capacity genomic sequencing technologies, with comprehensive genomic profiling, shifting the gears toward genomic medicine and modern biotechnology, which today underpins the development of most drugs. And, finally, in the latest version of PPO, the characterization of cancer will be of very high resolution (single-cell multi-OMICS); it will be dynamic (the transition from pre-cancer to cancer will be predictable), comprehensive (multi-OMICS biomarkers, spatial genomics, functional tests, organoid-driven precision medicine, multi-target drugs, hybrid pharmacological constructs), and data-driven (network medicine, AI, machine learning-decision-making tools, human digital twins).
Meanwhile, establishing therapy options and managing cancer treatments in the context of data from multi-OMICS manipulations is believed to be urgently necessary, and this view accelerates the implementation of PPM-related resources in oncology, resulting in PPO [131]. On a clinical PPO-related perspective, integrative analysis of multiple OMICS data gives a focus to functional targets being highly valuable for clinical translation. The integration of multiple biological layers of OMICS data brought PPO to a new paradigm, from tumor site classification to pan-cancer molecular classification, offering new therapeutic opportunities for precision medicine. On a more basic point of view, integrative data analysis heightens the OMICS fields, enables the oncogenic processes to be comprehensively interrogated, leading to a broader understanding of tumor biology and opening the way to integrative tumor model development, whilst dramatically accelerating the identification of robust biomarkers toward the development of tailored cancer therapy. The latter is an effective strategy to fight cancers by bridging OMICS technologies, IT resources and drug discovery trends to provide specific treatment for patients and preventive prophylaxis for pre-cancer persons-at-risk (both with different genetic characteristics). And thus, not only efficacy but also the adverse effects of drugs on cancer patients or pre-cancer persons-at-risk should be taken into account during the treatment [132,133].
In this context, high-throughput OMICS technologies allow the retrieval of comprehensive and holistic biological information, whereas computational capabilities enable high-dimensional data modeling and, therefore, accessible and user-friendly visualization. Rapid advances in high-throughput technologies of biomedical informatics aspects such as database storage and big data management, integration of OMICS within EHR, and interoperability have the potential to increase the weight of PPO and PPM as a whole within clinical cancer practice. The proposed architecture could improve the potentialities of data routinely collected in many health information systems to form a patient-centered information environment [134,135]. Furthermore, bioinformatics has enabled comprehensive multi-OMICS and clinical data integration for insightful interpretation [134,136,137] cancer care, where the right cancer treatment is given to the right person at the right time determined by the use of specific biomarkers, targets, tests and targeted drugs, is predicted to lead to better outcomes and reduced risk of side effects for patients with cancer as well as reducing costs and improving efficiencies for healthcare systems.
OMICS-driven Resources to fight Cancer
The development of PPO-guided and OMICS-supported (Fig. 11).
Figure 11: OMICS technologies as a Grand Portfolio to get PPM and PPO Armed
In this context, genetic testing and enhanced genomic analysis have had a profound impact on the way in which tumors are evaluated and classified. For instance, in 2002 a mutation in the BRAF gene was identified and found to be present in around half of all metastatic melanomas leading to the overproduction and spread of cancer cells. A number of new drugs, including vemurafenib and dabrafenib, which target proteins that prevent the immune system attacking cancer cells, have been developed as a result of this discovery [138]. Among a variety of the alternative genetic tests, let me stress that predictive genetic testing is really a crucial and valuable type of testing used to look for inherited gene mutations that might put a person at higher risk of getting certain kinds of cancer. This type of testing might be suggested for: a person with a strong family history of certain types of cancer; a person already diagnosed with cancer; and family members of a person known to have an inherited gene mutation that increases their risk of cancer. Prognostic biomarkers associate host and tumor variables with clinical outcomes independent of treatment, showcasing how aggressive a tumor is likely to be [139-141]. These biomarkers have an impact on the prognosis of cancer patients or pre-cancer persons-at-risk regardless of treatment, predicting the mean clinical outcome of a patient. They can be used to stratify randomization by disease risk, thus minimizing heterogeneity within the subgroup and maximizing heterogeneity across subgroups; to identify potential treatment targets; and to direct treatment to specific patient subgroups.
After the genetic information obtained and thus is available, the client (cancer patient or pre-cancer person-at-risk) would contact genetic counseling service for making the final CD making. Before and after genetic testing, genetic counseling can help you understand what your test results might mean, your risk of developing cancer, and what you can do about this risk. Moreover, family cancer centers can advise you about your risk of developing cancer, provide genetic counselling and medical advice and, in some situations, comprehensive genetic testing. The implementation of PPO through OMICS-guided profiling technologies has increasingly been integrated with standard clinic-pathological evaluations to enhance diagnosis, prognostication, and prediction of clinical outcomes. And thus, the number of druggable tumor-specific molecular aberrations has grown substantially in the past decade, with a significant survival benefit obtained from biomarker matching therapies in several cancer types. Molecular pathology has therefore become fundamental not only to inform on tumor diagnosis and prognosis but also to drive therapeutic decisions in daily practice. In this context, pharmacogenomics (PGx) is one of the most important components of PPO, which focuses on the association between genetic variations and drug response. PGx can help oncologists decide drug selection, dose adjustment, and treatment period and prevent adverse drug reactions. Specific genetic variations have been related to clinically significant changes in drug disposition between individuals, including vulnerability to adverse drug responses and therapeutic response or efficacy. There is a substantial amount of scientific evidence supporting the utility of pharmacogenomics testing in cancer patient management [142-147]. PGx testing (Fig. 12A, 12B) is aimed at tailoring cancer drug therapy at a dosage that is most appropriate for an individual cancer patient or a pre-cancer person-at-risk, with the potential benefits of increasing the clinical efficacy and individualized safety.
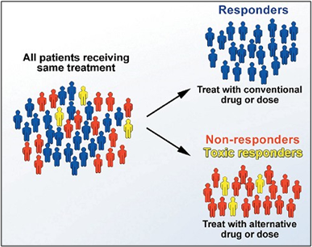
Figure 12A: Predictive DNA testing in can-cer practice
Pharmacogenomic tests can be used to predict and to target medicines to good responders or to identify whether an individual has an increased risk of a specific adverse drug reaction from a particular medicine.
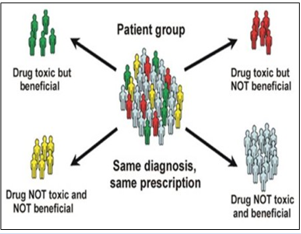
Figure 12B: Predictive DNA testing in cancer practice
Pharmacogenomic tests can be used to predict and to target medicines to good responders or to identify whether an individual has an increased risk of a specific adverse drug reaction from a particular medicine [142-147]. This scenario illustrates the fundamental idea behind PPM and PPO: coupling established clinical–pathological indexes with state-of-the-art molecular profiling to create diagnostic, prognostic, and therapeutic strategies precisely tailored to each patient’s requirements. Recent design-inspired biotechnological advances have led to an explosion of cancer-relevant molecular information, with the potential for greatly advancing patient care. In reality, PPO is an emerging approach for tumor treatment and prevention that takes into account inter- and intra-tumor variability in genes, tumor (immune) environment, and lifestyle and morbidities of each person diagnosed with cancer (including pre-cancer person-at-risk). PPM-driven PPO-armed cancer therapy have the potential to tailor therapy towards the oncogenic drivers of the tumor and modulate the tumor immune environment. Furthermore, PPO aims to optimize tumor response, thereby taking into account the therapy-induced toxicities for each specific patient. In this way, optimized tumor response is combined with the preservation of organ function and, thus, quality of life. Moreover, this ensures better patient care in the end, which is, of course, what it aims for.
One of the crucially valuable and innovation areas of PPO with the highest impact on the healthcare model that shows the earliest and greatest promise is molecular diagnostics and treatment of the next step generation – panels of upgraded tools (companion diagnostics and theranostics as tests and medicines) used to identify specific biomarkers and profiled targets of a disease, or disease susceptibility and aimed to lead us to the approach of PPO.
Moreover, PPO presents principally new opportunities for patients with cancer and pre-cancer persons-at-risk as well, whilst emerging as the tumor treatment and prevention that consider the cancer variability in terms of gene expression patterns, tumor specific (immune) microenvironment, and patients’ particular lifestyles and morbidities, covering huge Data Sets! So, as PPO introduces a Big Data analysis of PPO-guided OMICS approaches, there are still challenges in the translation of all these data into meaningful and equitable benefits to patients and health care. And thus, each patient presents its specific preferences, needs, tolerances, and unique tumor vulnerabilities even when suffering from very similar diseases or course of treatment, which demands and highlight the importance of the PPO approach and the personalized cancer or pre-cancer care. In reality, it is time to recognize the possibility that advanced computer implementation could generate real-world data that expand our understanding of cancer, rapidly identify new treatments, and create personalized drugs or immune therapies.
This perspective fosters the development of specialized treatments for each specific subtype of cancer, based on the measurement and manipulation of key patient OMICS data. And the field of systems biology, design-driven biotech and translational applications would thus aid in the development of diagnostic and therapeutic tools and medicines of the next step generation by analyzing data from preclinical and clinical studies. This approach is used to develop predictive and prognostic tools that replicate biological systems in order to characterize their behavior and response in the context of disease and drug development. This is particularly relevant to forthcoming cancer treatments, as a significant portion of oncology drugs in development are personalized medicines. PPM therapies that are currently being developed include cancer vaccines, mAbs, and CAR T-cells [148]. Meanwhile, a lack of medical guidelines has been identified by the majority of responders as the predominant barrier for adoption, indicating a need for the development of best practices and guidelines to support the implementation of PPO! Implementation of the latter, being paired and integrated in one and new entity, require a lot before the current model “physician-patient” could be gradually displaced by a new model “medical advisor-healthy person-at-risk”. This is the reason for developing global scientific, clinical, social, and educational projects in the area of PPM to elicit the content of the new branch.
A major challenge in PPO lies in establishing the relationship between biological data, disease, design-driven biotech and clinical translation: how can we interpret “Big Data,” referring to the greater collection of healthcare data across thousands of patients and pre-cancer persons-at-risk, involving the tracking of various medical indicators and biomarkers (primarily clinical and OMICS data). collected to make meaningful medical decisions? High-throughput data collection enables researchers, bio designers and bioengineers to screen tissues for thousands of molecular targets, effectively capturing the response of a complex system over time. Statistically interpreting trends from Big Data is a discipline unto itself and is necessary for predictive modeling and clinical decision support [149-157]. PPO as the trend toward PPM in oncology continues, coordination of all health care stakeholders has become more important than ever. Oncologists, pathologists, and payers must work with pharmaceutical, biotech and diagnostic companies to develop products, services, and coverage policies that improve patient outcomes and, as we have begun to see, lower overall health care costs for institutions that put personalized regimens in place.
References
- van Renterghem AWJ, van de Haar J, Voest EE. (2023). Functional precision oncology using patient-derived assays: bridging genotype and phenotype. Nat Rev Clin Oncol. 20(5):305-317.
Publisher | Google Scholor - Yoon H, Lee S. (2021). Integration of Genomic Profiling and Organoid Development in Precision Oncology. Int J Mol Sci. 23(1):216.
Publisher | Google Scholor - Letai A, Bhola P, Welm AL. (2022). Functional precision oncology: Testing tumors with drugs to identify vulnerabilities and novel combinations. Cancer Cell. 40(1):26-35.
Publisher | Google Scholor - Brown NA, Elenitoba-Johnson KSJ. (2020). Enabling Precision Oncology Through Precision Diagnostics. Annu Rev Pathol. 15:97-121.
Publisher | Google Scholor - Fujiwara Y, Kato S, Kurzrock R. (2024). Evolution of Precision Oncology, Personalized Medicine, and Molecular Tumor Boards. Surg Oncol Clin N Am. 33(2):197-216.
Publisher | Google Scholor - Incorvaia L, Russo A, Cinieri S. (2022). The molecular tumor board: a tool for the governance of precision oncology in the real world. Tumori. 108(4):288-290.
Publisher | Google Scholor - Bilkey GA, Burns BL, Coles EP, Mahede T, Baynam G, et al. (2019). Optimizing Precision Medicine for Public Health. Front Public Health. 7:42.
Publisher | Google Scholor - Weeramanthri TS, Dawkins HJS, Baynam G, Bellgard M, Gudes O, et al. (2018). Editorial: precision public health. Front Public Health. 6:121.
Publisher | Google Scholor - Martin-Sanchez F, Lázaro M, López-Otín C, Andreu AL, Cigudosa JC, et al. (2023). Personalized Precision Medicine for Health Care Professionals: Development of a Competency Framework. JMIR Med Educ. 9:e43656.
Publisher | Google Scholor - Alvarez, M.J.R. (2022). Precision Public Health Perspectives. In: Hasanzad, M. (eds) Precision Medicine in Clinical Practice. Springer, Singapore.
Publisher | Google Scholor - Traversi D, Pulliero A, Izzotti A, Franchitti E, Iacoviello L, et al. (2021). Precision Medicine and Public Health: New Challenges for Effective and Sustainable Health. J. Pers. Med. 11:135.
Publisher | Google Scholor - Stefanicka-Wojtas D, Kurpas D. (2023). Personalised MedicineImplementation to the Healthcare System in Europe (Focus Group Discussions). Journal of Personalized Medicine. 13:380.
Publisher | Google Scholor - Ahmed Z. (2020). Practicing precision medicine with intelligently integrative clinical and multi-omics data analysis. Hum Genomics. 14:35.
Publisher | Google Scholor - McAlister FA, Laupacis A, Armstrong PW. (2017). Finding the right balance between precision medicine and personalized care. CMAJ. 189(33):E1065-E1068.
Publisher | Google Scholor - Delpierre C, Lefèvre T. (2023). Precision and personalized medicine: What their current definition says and silences about the model of health they promote. Implication for the development of personalized health. Front Sociol. 8:1112159.
Publisher | Google Scholor - Nielsen J. (2017). Systems Biology of Metabolism: A Driver for Developing Personalized and Precision Medicine. Cell Metab. 25(3):572-579.
Publisher | Google Scholor - Hoeben A, Joosten EAJ, van den Beuken-van Everdingen MHJ. (2021). Personalized Medicine: Recent Progress in Cancer Therapy. Cancers (Basel). 13(2):242.
Publisher | Google Scholor - Larance M & Lomond AI. (2015). Multidimensional proteomics for cell biology. Nat. Rev. Mol. Cell. Biol 16:269-280.
Publisher | Google Scholor - Han XM, Aslanian A & Yates JR Mass spectrometry for proteomics. Curr. Opin. Chem. Biol. 12:483-490.
Publisher | Google Scholor - Duarte TT & Spencer CT. (2016). Personalized proteomics: The future of precision medicine. Proteomes. 4.
Publisher | Google Scholor - Gregorich ZR & Ge Y. (2014). Top-down proteomics in health and dis-ease: Challenges and opportunities. Proteomics. 14:1195-1210.
Publisher | Google Scholor - Sidoli, S., Lu, C., Coradin, M. et al. (2017). Metabolic labeling in middle-down proteomics allows for investigation of the dynamics of the histone code. Epigenetics & Chromatin. 10:34.
Publisher | Google Scholor - Monteiro MS, Carvalho M, Bastos ML & Guedes de Pinho P. (2013). Metabolomics analysis for biomarker discovery: Advances and challenges. Curr. Med. Chem. 20:257-271.
Publisher | Google Scholor - Roessner U & Bowne J. (2009). What is metabolomics all about? Biotechniques. 46:363.
Publisher | Google Scholor - Everett JR, Loo RL & Pullen FS. (2013). Pharmacometabonomics and personal-ized medicine. Ann. Clin. Biochem. 50:523.545.
Publisher | Google Scholor - Luvhengo TE, Bombil I, Mokhtari A, Moeng MS, Demetriou D, et al. (2023). Multi-Omics and Management of Follicular Carcinoma of the Thyroid. Biomedicines. 11(4):1217.
Publisher | Google Scholor - Medori MC, Micheletti C, Gadler M, Benedetti S, Guerri G, et al. (2023). Omics sciences and precision medicine in prostate cancer. Clin Ter. 174(Suppl 2(6)):95-103.
Publisher | Google Scholor - Lai B, Fu J, Zhang Q, Deng N, Jiang Q, Peng J. (2023). Artificial intelligence in cancer pathology: Challenge to meet increasing demands of precision medicine. Int J Oncol. 63(3):107.
Publisher | Google Scholor - Jose A, Kulkarni P, Thilakan J, Munisamy M, Malhotra AG, et al. (2024). Integration of pan-omics technologies and three-dimensional in vitro tumor models: an approach toward drug discovery and precision medicine. Mol Cancer. 23(1):50.
Publisher | Google Scholor - Dar MA, Arafah A, Bhat KA, Khan A, Khan MS, et al. (2023). Multiomics technologies: role in disease biomarker discoveries and therapeutics. Brief Funct Genomics. 22(2):76-96.
Publisher | Google Scholor - Nafees A, Khan M, Chow R, Fazelzad R, Hope A, et al. (2023). Evaluation of clinical decision support systems in oncology: An updated systematic review. Crit Rev Oncol Hematol. 192:104143.
Publisher | Google Scholor - Beeler PE, Bates DW, Hug BL. (2014). Clinical decision support systems. Swiss Med Wkly. 144:w14073.
Publisher | Google Scholor - Mukherjee T, Pournik O, Lim Choi Keung SN, Arvanitis TN. (2023). Clinical Decision Support Systems for Brain Tumour Diagnosis and Prognosis: A Systematic Review. Cancers (Basel). 15(13):3523.
Publisher | Google Scholor - Syrowatka A, Motala A, Lawson E, Shekelle P. (2024). Computerized Clinical Decision Support to Prevent Medication Errors and Adverse Drug Events: Rapid Review. 2024 Feb. In: Making Healthcare Safer IV: A Continuous Updating of Patient Safety Harms and Practices. Rockville (MD): Agency for Healthcare Research and Quality (US).
Publisher | Google Scholor - Hendriks MP, Jager A, Ebben KCWJ, van Til JA, Siesling S. (2024). Clinical decision support systems for multidisciplinary team decision-making in patients with solid cancer: Composition of an implementation model based on a scoping review. Crit Rev Oncol Hematol. 195:104267.
Publisher | Google Scholor - Kohut K, Morton K, Turner L, Shepherd J, Fenerty V, et al. (2023). Patient decision support resources inform decisions about cancer susceptibility genetic testing and risk management: a systematic review of patient impact and experience. Front Health Serv. 3:1092816.
Publisher | Google Scholor - McAlister FA, Laupacis A, Armstrong PW. (2017). Finding the right balance between precision medicine and personalized care. CMAJ. 189(33):E1065-E1068.
Publisher | Google Scholor - Palsson, B. (2015). Systems biology. Cambridge university press.
Publisher | Google Scholor - Trewavas A. (2006). A brief history of systems biology. Every object that biology studies are a system of systems. The Plant Cell, 18(10):2420-2430.
Publisher | Google Scholor - Galas, David. (2015). Systems Biology. Encyclopedia Britannica.
Publisher | Google Scholor - Iman Tavassoly, Joseph Goldfarb, Ravi Iyengar; (2018). Systems biology primer: the basic methods and approaches. Essays Biochem; 62 (4):487-500.
Publisher | Google Scholor - Gonzalez-Angulo AM, Hennessy BT, Mills GB. (2010). Future of personalized medicine in oncology: a systems biology approach. J Clin Oncol. 28(16):2777-2783.
Publisher | Google Scholor - Mambetsariev I, Fricke J, Gruber SB, Tan T, Babikian R, et al. (2023). Clinical Network Systems Biology: Traversing the Cancer Multiverse. J Clin Med. 2(13):4535.
Publisher | Google Scholor - Turanli B, Karagoz K, Gulfidan G, Sinha R, Mardinoglu A, et al. (2018). A Network-Based Cancer Drug Discovery: From Integrated Multi-Omics Approaches to Precision Medicine. Curr Pharm Des. 24(32):3778-3790.
Publisher | Google Scholor - Fawaz A, Ferraresi A, Isidoro C. (2023). Systems Biology in Cancer Diagnosis Integrating Omics Technologies and Artificial Intelligence to Support Physician Decision Making. J Pers Med. 13(11):1590.
Publisher | Google Scholor - Najarian, K., Najarian, S., Gharibzadeh, S., & Eichelberger, C. N. (2009). Systems biology and bioinformatics: a computational approach. CRC Press.
Publisher | Google Scholor - Klipp E, Herwig R, Kowald A, Wierling C & Lehrach H. (2005). Systems biology in practice: concepts, implementation and application, Wiley.
Publisher | Google Scholor - John Wiley & Sons, Chen R, Snyder M. (2021). Systems biology: personalized medicine for the future? Curr Opin Pharmacol. 12(5):623-628.
Publisher | Google Scholor - Rees L, Weil A. (2001). Integrated medicine. BMJ. 322(7279):119-120.
Publisher | Google Scholor - David P. Rakel, Vincent Minichiello. (2022). Traditional, Complementary and Integrative Medicine (TCI); Integrative Medicine, 5th Edition-Elsevier.
Publisher | Google Scholor - Debleena Guin, Sarita Thakran, Pooja Singh, S. Ramachandran, Yasha Hasija, et al, (2021). Chapter 1 - Translational biotechnology: A transition from basic biology to evidence-based research, Editor(s): Yasha Hasija, Translational Biotechnology, Academic Press, 3-24.
Publisher | Google Scholor - Lindahl, Sten and Marincola, Francesco. (2023). Translational medicine. Encyclopedia Britannica.
Publisher | Google Scholor - Padilla-Cabello J, Santisteban-Espejo A, Heradio R, Cobo MJ, Martin-Piedra MA, et al. (2022). Methods for identifying biomedical translation: a systematic review. Am J Transl Res. 14(4):2697-2708.
Publisher | Google Scholor - Ahmed, Z. (2020). Practicing precision medicine with intelligently integrative clinical and multi-omics data analysis. Hum Genomics, 14:35.
Publisher | Google Scholor - Tebani A, Afonso C, Marret S, Bekri S. (2016). Omics-Based Strategies in Precision Medicine: Toward a Paradigm Shift in Inborn Errors of Metabolism Investigations. Int J Mol Sci. 17(9).
Publisher | Google Scholor - Kun-Hsing Yu, Michael Snyder, (2016). Omics Profiling in Precision Oncology, Molecular & Cellular Prote-omics, 15(8),2525-2536.
Publisher | Google Scholor - M. Afzal, S. M. Riazul Islam, M. Hussain and S. Lee, (2020). Precision Medicine Informatics: Principles, Prospects, and Challenges, in IEEE Access, 8:13593-13612.
Publisher | Google Scholor - Ying Yu, Yunjin Wang, Zhaojie Xia, Xiangyu Zhang, Kailiang Jin, et al, (2019). PreMedKB: an integrated precision medicine knowledgebase for interpreting relationships between diseases, genes, variants and drugs. Nucleic Acids Research, 47(D1,08):D1090-D1101.
Publisher | Google Scholor - Moscatelli M, Manco-ni A, Pessina M. et al. (2018). An infrastructure for precision medicine through analysis of big data. BMC Bioinformatics. 19(Suppl 10):351.
Publisher | Google Scholor - Bjerrum A, Lassen U. (2023). Putting data to work for precision medicine. Cell Rep Med. 4(7):101090.
Publisher | Google Scholor - Simoes E. (2015). Health information technology advances health care delivery and enhances research. Mo Med. 112(1):37-40.
Publisher | Google Scholor - Fraser HSF, Zahiri K, Kim N, Kim C, Craig S. (2023). The Glob-al Health Informatics landscape and JAMIA. J Am Med Inform Assoc. 30(4):775-780.
Publisher | Google Scholor - Aneja S, Avesta A, Xu H, Machado LO. (2023). Clinical Informatics Approaches to Facilitate Cancer Data Sharing. Yearb Med Inform. 32(1):104-110.
Publisher | Google Scholor - Pristner M, Warth B. (2020). Drug-Exposome Interactions: The Next Frontier in Precision Medicine. Trends Pharmacol Sci. 41(12):994-1005.
Publisher | Google Scholor - Baccarelli A, Dolinoy D.C & Walker C.L. (2023). A precision environmental health approach to prevention of human disease. Nat Commun. 14:2449.
Publisher | Google Scholor - van Harten AM, Brakenhoff RH. (2021). Targeted Treatment of Head and Neck (Pre)Cancer: Preclinical Target Identification and Development of Novel Therapeutic Applications. Cancers (Basel). 13(11):2774.
Publisher | Google Scholor - Röcken C. (2023). Predictive biomarkers in gastric cancer. J Cancer Res Clin Oncol. 149(1):467-481.
Publisher | Google Scholor - Pessoa LS, Heringer M, Ferrer VP. (2020). ctDNA as a cancer biomarker: A broad overview. Crit Rev Oncol Hematol. 155:103109.
Publisher | Google Scholor - Wallington-Beddoe CT, Mynott RL. (2021). Prognostic and predictive biomarker developments in multiple myeloma. J Hematol Oncol. 14(1):151.
Publisher | Google Scholor - Tarighati E, Keivan H, Mahani H. (2023). A review of prognostic and predictive biomarkers in breast cancer. Clin Exp Med. 23(1):1-16.
Publisher | Google Scholor - Yu D, Li Y, Wang M, Gu J, Xu W, et al. (2022). Exosomes as a new frontier of cancer liquid biopsy. Mol Cancer. 21(1):56.
Publisher | Google Scholor - Zhang F, Chen J.Y. (2010). Discovery of pathway biomarkers from coupled proteomics and systems biology methods. BMC Ge-nomics. 11(Suppl 2):S12.
Publisher | Google Scholor - Chen H, Zhu Z, Zhu Y, Wang J, Mei Y, et al. (2015). Pathway mapping and development of dis-ease-specific biomarkers: protein-based network biomarkers. J Cell Mol Med. 19(2):297-314.
Publisher | Google Scholor - Sheng M, Xie X, Wang J, Gu W. (2019). A Pathway-Based Strategy to Identify Biomarkers for Lung Cancer Diagnosis and Prognosis. Evolutionary Bioinformatics, 15.
Publisher | Google Scholor - Ben-Hamo R, Jacob Berger A, Gavert N, et al. (2020). Predicting and affecting response to cancer therapy based on pathway-level biomarkers. Nat Commun. 11:3296.
Publisher | Google Scholor - Rapisuwon S, Vietsch EE, Wellstein A. (2016). Circulating biomarkers to monitor cancer progression and treatment. Comput Struct Biotechnol J. 14:211-222.
Publisher | Google Scholor - Purkayastha K, Dhar R, Pethusamy K, Srivastava T, Shankar A, et al. (2023). The issues and challenges with cancer biomarkers. Cancer Res Ther. 19(Supplement):S20-S35.
Publisher | Google Scholor - Wang Z, Li R, Yang G, Wang Y. (2024). Cancer stem cell biomarkers and related signaling pathways, J Drug Target. 32(1):33-44.
Publisher | Google Scholor - Chakrabortty A, Patton DJ, Smith BF, Agarwal P. (2023). miRNAs: Potential as Biomarkers and Therapeutic Targets for Cancer. Genes (Basel). 14(7):1375.
Publisher | Google Scholor - Sheng W, Zhang C, Mohiuddin TM, Al-Rawe M, Zeppernick F, et al. (2023). Multiplex Immunofluorescence: A Powerful Tool in Cancer Immunotherapy. Int J Mol Sci. 24(4):3086.
Publisher | Google Scholor - Tan WCC, Nerurkar SN, Cai HY, Ng HHM, Wu D, et al. (2020). Overview of multiplex immunohistochemistry/immunofluorescence techniques in the era of cancer immunotherapy. Cancer Commun (Lond). 40(4):135-153.
Publisher | Google Scholor - Harms PW, Frankel TL, Moutafi M, Rao A, Rimm DL, et al. (2023). Multiplex Immunohistochemistry and Immunofluorescence: A Practical Update for Pathologists. Mod Pathol. 36(7):100197.
Publisher | Google Scholor - Lewis SM, Asselin-Labat ML, Nguyen Q, Berthelet J, Tan X, et al. (2021). Spatial omics and multiplexed imaging to explore cancer biology. Nat Methods. 18(9):997-1012.
Publisher | Google Scholor - Van Gool A, Corrales F, Čolović M, Krstić D, Oliver-Martos B, et al. (2020). Analytical techniques for multiplex analysis of protein biomarkers. Expert Rev Proteomics. 17(4):257-273.
Publisher | Google Scholor - Hickey JW, Neumann EK, Radtke AJ, Camarillo JM, Beuschel RT, et al. (2022). Spatial mapping of protein composition and tissue organization: a primer for multiplexed antibody-based imaging. Nat Methods. 19(3):284-295.
Publisher | Google Scholor - Normanno N, Apostolidis K, de Lorenzo F, Beer PA, Henderson R, et al. (2022). Cancer Biomarkers in the era of precision oncology: Addressing the needs of patients and health systems. Semin Cancer Biol. 84:293-301.
Publisher | Google Scholor - Normanno N, Apostolidis K, Wolf A, Al Dieri R, Deans Z, et al. (2022). Access and quality of biomarker testing for precision oncology in Europe. Eur J Cancer. 176:70-77.
Publisher | Google Scholor - Mishra A, Verma M. (2010). Cancer Biomarkers: Are We Ready for the Prime Time? Cancers, 2:190-208.
Publisher | Google Scholor - Rao Bommi J, Kummari S, Lakavath K, Sukumaran R.A, Panicker L.R, et al. (2023). Recent Trends in Biosensing and Diagnostic Methods for Novel Cancer Biomarkers. Biosensors, 13:398.
Publisher | Google Scholor - Sarhadi VK, Armengol G. (2022). Molecular Biomarkers in Cancer. Biomolecules. 12(8):1021.
Publisher | Google Scholor - GARCÍA-CLOSAS, MONTSERRAT, and others, (2009). Application of Biomarkers in Cancer Epidemiology, in David Schottenfeld, and Joseph F. Fraumeni (eds), Cancer Epidemiology and Prevention, 3rd edition.
Publisher | Google Scholor - Liu D. (2019). Cancer biomarkers for targeted therapy. Biomark Res, 7:25.
Publisher | Google Scholor - Shinozuka T, Kanda M, Kodera Y. (2023). Site-specific protein biomarkers in gastric cancer: a comprehensive review of novel biomarkers and clinical applications. Expert Rev Mol Diagn. 23(8):701-712.
Publisher | Google Scholor - Matsuoka T, Yashiro M. (2023). Novel biomarkers for early detection of gastric cancer. World J Gastroenterol. 29(17):2515-2533.
Publisher | Google Scholor - Scholl S, Roufai DB, Chérif LL, Kamal M. (2023). RAIDS atlas of significant genetic and protein biomarkers in cervical cancer. J Gynecol Oncol. 34(5):e74.
Publisher | Google Scholor - Das S, Dey MK, Devireddy R, Gartia MR. (2023). Biomarkers in Cancer Detection, Diagnosis, and Prognosis. Sensors (Basel). 24(1):37.
Publisher | Google Scholor - Pabst L, Lopes S, Bertrand B, Creusot Q, Kotovskaya M, et al. (2023). Prognostic and Predictive Biomarkers in the Era of Immunotherapy for Lung Cancer. Int J Mol Sci. 24(8):7577.
Publisher | Google Scholor - Umapathy VR, Natarajan PM, Swamikannu B. (2023). Review Insights on Salivary Proteomics Biomarkers in Oral Cancer Detection and Diagnosis. Molecules. 28(13):5283.
Publisher | Google Scholor - Aboagye EO, Barwick TD, Haberkorn U. (2023). Radiotheranostics in oncology: Making precision medicine possible. CA Cancer J Clin. 73(3):255-274.
Publisher | Google Scholor - van Renterghem AWJ, van de Haar J, Voest EE. (2023). Functional precision oncology using patient-derived assays: bridging genotype and phenotype. Nat Rev Clin Oncol. 20(5):305-317.
Publisher | Google Scholor - Pomykala KL, Hadaschik BA, Sartor O, Gillessen S, Sweeney CJ, et al. (2023). Next generation Radiotheranostics promoting precision medicine. Ann Oncol. 34(6):507-519.
Publisher | Google Scholor - Lin X, Zong C, Zhang Z, Fang W, Xu P. (2023). Progresses in biomarkers for cancer immunotherapy. MedComm. 4(5):e387.
Publisher | Google Scholor - Zhao Z, Li T, Yuan Y, Zhu Y. (2023). What is new in cancer-associated fibroblast biomarkers? Cell Commun Signal. 21(1):96.
Publisher | Google Scholor - Saoudi González N, Salvà F, Ros J, Baraibar I, Rodríguez-Castells M, et al. (2023). Unravelling the Complexity of Colorectal Cancer: Heterogeneity, Clonal Evolution, and Clinical Implications. Cancers (Basel). 15(16):4020.
Publisher | Google Scholor - Lim YX, Mierzwa ML, Sartor MA, D'Silva NJ. (2023). Clinical, morphologic and molecular heterogeneity of HPV-associated oropharyngeal cancer. Oncogene. 42(40):2939-2955.
Publisher | Google Scholor - Chen W, Xu D, Liu Q, Wu Y, Wang Y, et al. (2023). Unraveling the heterogeneity of cholangiocarcinoma and identifying biomarkers and therapeutic strategies with single-cell sequencing technology. Biomed Pharmacother. 162:114697.
Publisher | Google Scholor - Megyesfalvi Z, Gay CM, Popper H, Pirker R, Ostoros G, et al. (2023). Clinical insights into small cell lung cancer: Tumor heterogeneity, diagnosis, therapy, and future directions. CA Cancer J Clin. 73(6):620-652.
Publisher | Google Scholor - Li J, Li L, You P, Wei Y, Xu B. (2023). Towards artificial intelligence to multi-omics characterization of tumor heterogeneity in esophageal cancer. Semin Cancer Biol. 91:35-49.
Publisher | Google Scholor - Yu X, Liu R, Gao W, Wang X, Zhang Y. (2023). Single-cell omics traces the heterogeneity of prostate cancer cells and the tumor microenvironment. Cell Mol Biol Lett. 28(1):38.
Publisher | Google Scholor - Wen R, Zhou L, Peng Z, Fan H, Zhang T, et al. (2023). Single-cell sequencing technology in colorectal cancer: a new technology to disclose the tumor heterogeneity and target precise treatment. Front Immunol. 14:1175343.
Publisher | Google Scholor - Yang P, Yang W, Wei Z, Li Y, Yang Y, et al. (2023). Novel targets for gastric cancer: The tumor microenvironment (TME), N6-methyladenosine (m6A), pyroptosis, autophagy, ferroptosis and cuproptosis. Biomed Pharmacother. 163:114883.
Publisher | Google Scholor - Xu X, Zhou N, Lan H, Yang F, Dong B, et al. (2022). The Ferroptosis Molecular Subtype Reveals Characteristics of the Tumor Microenvironment, Immunotherapeutic Response, and Prognosis in Gastric Cancer. Int J Mol Sci. 23(17):9767.
Publisher | Google Scholor - Yang R, Yu Y. (2023). Patient-derived organoids in translational oncology and drug screening. Cancer Lett. 562:216180.
Publisher | Google Scholor - Gu Y, Fang Y, Wu X, Xu T, Hu T, et al. (2023). The emerging roles of SUMOylation in the tumor microenvironment and therapeutic implications. Exp Hematol Oncol. 12(1):58.
Publisher | Google Scholor - Tian X, Wang T, Shen H, Wang S. (2023). Tumor microenvironment, histone modifications, and myeloid-derived suppressor cells. Cytokine Growth Factor Rev. 74:108-121.
Publisher | Google Scholor - Chen Y, Li H, Fan Y. (2023). Shaping the tumor immune microenvironment of SCLC: Mechanisms, and opportunities for immunotherapy. Cancer Treat Rev. 120:102606.
Publisher | Google Scholor - Li W, Zhou Z, Zhou X, Khoo BL, Gunawan R, et al. (2023). 3D Biomimetic Models to Reconstitute Tumor Microenvironment In Vitro: Spheroids, Organoids, and Tumor-on-a-Chip. Adv Healthc Mater. 12(18):e2202609.
Publisher | Google Scholor - Zhang J, Liu S, Chen X, Xu X, Xu F. (2023). Non-immune cell components in tumor microenvironment influencing lung cancer Immunotherapy. Biomed Pharmacother. 166:115336.
Publisher | Google Scholor - Dagogo-Jack, I., Shaw, A. (2018). Tumour heterogeneity and resistance to cancer therapies. Nat Rev Clin Oncol, 15:81-94.
Publisher | Google Scholor - Cirkel GA, Gadellaa-van Hooijdonk CG, Koudijs MJ, Willems SM, Voest EE. (2014). Tumor heterogeneity and personalized cancer medicine: are we being outnum-bered? Future Oncol. 10(3):417-428.
Publisher | Google Scholor - Duojiao Wu, Diane C. Wang, Yunfeng Cheng, Mengjia Qian, Miaomiao Zhang, Qet al, (2017). Roles of tumor heterogeneity in the development of drug resistance: A call for precision therapy, Seminars in Cancer Biology. 42:13-19.
Publisher | Google Scholor - Guofeng Ma, Xuecheng Yang, Ye Liang, Liping Wang, Dan Li, et al, (2018). Precision medicine and bladder cancer heterogeneity. Bulletin du Cancer, 105(10):925-931.
Publisher | Google Scholor - Tomasik B, Garbicz F, Braun M, Bieńkowski M, Jassem J. (2024). Heterogeneity in precision oncology. Cambridge Prisms: Precision Medicine. 2:e2.
Publisher | Google Scholor - Jialing Zhang, Stephan Stanislaw Späth, Sadie L Marjani, Wengeng Zhang, Xinghua Pan, (2018). Characterization of cancer genomic heterogeneity by next-generation sequencing advances precision medicine in cancer treatment, Precision Clinical Medicine, 1(1):29-48.
Publisher | Google Scholor - Marina Danilenko, Steven C. Clifford, Edward C. Schwalbe, (2021). Inter and intra-tumoral heterogeneity as a platform for personalized therapies in medullo-blastoma, Pharmacology & Therapeutics, 228:107828.
Publisher | Google Scholor - Dagogo-Jack, I., Shaw, A. (2018). Tumour heterogeneity and resistance to cancer thera-pies. Nat Rev Clin Oncol, 15:81-94.
Publisher | Google Scholor - Cirkel GA, Gadellaa-van Hooijdonk CG, Koudijs MJ, Willems SM, Voest EE. (2014). Tumor heterogeneity and personalized cancer medicine: are we being outnumbered? Future Oncol. 10(3):417-428.
Publisher | Google Scholor - Ahmed, Z. (2020). Practicing precision medicine with intelligently integrative clinical and multi-omics data analysis. Hum Genomics, 14:35.
Publisher | Google Scholor - Yijun Liu, Fuhu Song, Zhi Li, Liang Chen, Ying Xu, et al. (2023). A comprehensive tool for tumor precision medicine with pharmaco-omics data analysis. Front. Pharmacol., 14:1-9.
Publisher | Google Scholor - Maggi N, Gazzarata R, Ruggiero C, Lombardo C, Giacomini M. (2019). Cancer precision medicine today: Towards omic information in healthcare systems. Tumori Journal. 105(1):38-46
Publisher | Google Scholor - Dilara Akhoundova, Mark A. Rubin, (2022). Clinical application of advanced multi-omics tumor pro-filing: Shaping precision oncology of the future. Cancer Cell, 40(9):920-938.
Publisher | Google Scholor - Tebani A, Afonso C, Marret S, Bekri S. (2016). Omics-Based Strategies in Precision Medicine: Toward a Paradigm Shift in Inborn Errors of Metabolism Investigations. Int J Mol Sci. 17(9):1555.
Publisher | Google Scholor - Hayes, D.F. (2013). OMICS-based personalized oncology: if it is worth doing, it is worth doing well! BMC Med, 11:221.
Publisher | Google Scholor - Su, M. Y. & Fisher, D. E. (2016). Immunotherapy in the Precision Medicine Era: Melanoma and Be-yond. PLoS Med. 13.
Publisher | Google Scholor - Kosorok, M. R. & Laber, E. B. (2019). Precision Medicine. Annu. Rev. Stat. its Appl. 6:263-286.
Publisher | Google Scholor - Salgado, R. et al. (2019). Addressing the dichotomy between individual and societal approaches to personalised medicine in oncology. Eur. J. Cancer. 114:128-136.
Publisher | Google Scholor - Halabi, S. & Niedzwiecki, D. (2019). Advancing Precision Oncology Through Biomarker-Driven Trials: Theory vs. Practice. Chance. 32:23.
Publisher | Google Scholor - Sadee W, Wang D, Hartmann K, Toland AE. (2023). Pharmacogenomics: Driving Personalized Medicine. Pharmacol Rev. 75(4):789-814.
Publisher | Google Scholor - Moore C, Lazarakis S, Stenta T, Alexander M, Nguyen RP, et al. (2023). A systematic review of knowledge, attitude and practice of pharmacogenomics in pediatric oncology patients. Pharmacol Res Perspect. 11(6):e01150.
Publisher | Google Scholor - Lim CX, Bozkurt A, Chen ZY, Hird A, Wickens J, et al. (2023). Healthcare professionals' and consumers' knowledge, attitudes, perspectives, and education need in oncology pharmacogenomics: A systematic review. Clin Transl Sci. 16(12):2467-2482.
Publisher | Google Scholor - de Joode K, Heersche N, Basak EA, Bins S, van der Veldt AAM, et al. (2024). Review - The impact of pharmacogenetics on the outcome of immune checkpoint inhibitors. Cancer Treat Rev. 122:102662.
Publisher | Google Scholor - Tremmel R, Pirmann S, Zhou Y, Lauschke VM. (2023). Translating pharmacogenomic sequencing data into drug response predictions-How to interpret variants of unknown significance. Br J Clin Pharmacol.
Publisher | Google Scholor - Bonetti G, Madeo G, Michelini S, Ricci M, Cestari M, et al. (2023). Omics sciences and precision medicine in breast and ovarian cancer. Clin Ter. 174(Suppl 2(6)):104-118.
Publisher | Google Scholor - Maciejko L, Smalley M & Goldman A. (2017). Cancer immunotherapy and personalized medicine: Emerging technologies and biomarker-based approaches. J. Mol. Biomark. 8.
Publisher | Google Scholor - Lee CH & Yoon HJ. (2017). Medical big data: Promise and challenges. Kidney Res. Clin. Pract, 36:3-11.
Publisher | Google Scholor - Babu E, Sen S. (2024). Explore & actuate: the future of personalized medicine in oncology through emerging technologies. Curr Opin Oncol. 36(2):93-101.
Publisher | Google Scholor - Pfohl U, Pflaume A, Regenbrecht M, Finkler S, Graf Adelmann Q, et al. (2021). Precision Oncology Beyond Genomics: The Future Is Here-It Is Just Not Evenly Distributed. Cells. 10(4):928.
Publisher | Google Scholor - Aguiar PN, Matsas S, Dienstmann R, Ferreira CG. (2023). Challenges and opportunities in building a health economic framework for personalized medicine in oncology. Per Med. 20(5):453-460.
Publisher | Google Scholor - Pandiella A, Calvo E, Moreno V, Amir E, Templeton A, et al. (2023). Considerations for the clinical development of immuno-oncology agents in cancer. Front Immunol. 14:1229575.
Publisher | Google Scholor - De Pauw T, De Mey L, Debacker JM, Raes G, Van Ginderachter JA, et al. (2023). Current status and future expectations of nanobodies in oncology trials. Expert Opin Investig Drugs. 32(8):705-721.
Publisher | Google Scholor - Parkinson JF, Ospina PA, Round J, McNeely ML, Jones CA. (2023). Generic Health Utility Measures in Exercise Oncology: A Scoping Review and Future Directions. Curr Oncol. 30(10):8888-8901.
Publisher | Google Scholor











