

Case Report
A Novel Technique of Spatially Fractionated Radiotherapy (SFRT) as Boost Radiation Therapy Treatment for Cervical Cancer in a Resource Limited Setting in Sub Saharan Africa
- Paul N Mobit 1,6*
- MosseB. A. Wilfried 1
- Farzaneh Mirkhaghani Haghighi
- Ngo Tega 1,5
- Edmund Folefac 4
- Mouelle Sone 1
- Waleed Mourad 3
1Cameroon Oncology Center, Douala, Cameroon.
2Cameroon Cancer Foundation, Douala, Cameroon.
3Department of Radiation Medicine, University of Kentucky Medical Center, KY, United States.
4Department of Medical Oncology, The James Comprehensive Cancer Center, Ohio State University, Columbus-Ohio, United States.
5The Yaoundé Gynaecology, Obstetrics and Paediatrics Hospital(HCOPY), Yaounde Cameroon.
6University of Mississippi Medical Center, Department of Radiation Oncology, Jackson-MS, United States.
*Corresponding Author: Paul N Mobit, University of Mississippi Medical Center, Department of Radiation Oncology, Jackson-MS, United States.
Citation: Paul N. Mobit, M.B.A. Wilfried, Farzaneh M. Haghighi, Tega N, Folefac E, et al. (2024). A Novel Technique of Spatially Fractionated Radiotherapy (SFRT) as Boost Radiation Therapy Treatment for Cervical Cancer in a Resource Limited Setting in Sub Saharan Africa. Journal of Cancer Management and Research, BioRes Scientia Publishers. 2(2):1-4. DOI: 10.59657/2996-4563.brs.24.015
Copyright: © 2024 Paul N Mobit, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 25, 2024 | Accepted: June 10, 2024 | Published: June 18, 2024
Abstract
Cervical cancer is one of top cancers affecting women in resource poor countries or areas. This is because absent effective screening protocol most of cervical cancers in these settings are diagnosed at an advanced stage. Cameroon Oncology Center is an independent and so that revenue neutral radiotherapy center located in the coastal city of Douala in the Republic of Cameroon, Central Africa. It is the only institution in the country and indeed in the sub region with a medical linear accelerator and offer radiotherapy services for patients not only from Cameroon but from the Central African sub region including Nigeria, Gabon, Chad. Cervical cancer remains a formidable health challenge in Cameroon and other resource poor settings, necessitating concerted efforts to improve access to screening, HPV vaccination and treatment services. The case highlights the challenges faced in the diagnosis, treatment and management of cervical cancer in resource poor settings and emphasizes the importance of multidisciplinary care and patient education.
Keywords: cervical cancer; cameroon oncology center; screening, multidisciplinary care; HPV
Case Presentation
The patient is a 66-year-old female admitted to Cameroon Oncology Center with a three months history of vaginal bleeding. The gynecological examination revealed globular and friable mass in the cervix and bilateral parametrial infiltration to the pelvic wall. A uterine cervical biopsy specimen revealed a moderately differentiated invasive adenocarcinoma of the cervix. The patient’s MRI revealed a heterogeneous uterine mass measuring 88 mm x103 mm x132 mm. The vaginal wall was not thickened and the ovaries could not be visualized but numerous uterine myomas. The patient was staged as a case of FIGO stage IIIB. Whole blood count, kidney and liver function tests were normal. A contrast enhanced CT scan of the thorax, abdomen and pelvis (TAP) was done and did not reveal any distance metastasis. Due to non-availability of nuclear medicine equipment in Cameroon, no other diagnostic imaging such as PET scans was done.
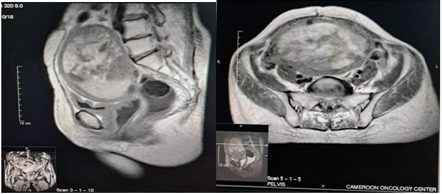
Figure 1: MRI of the pelvis showing the sagittal and axial view and showing the huge fibroid which has almost engulf the pelvic cavity and pushing other structures from their normal position in the body.
After the multi-disciplinary tumor board review, it was decided that the patient should undergo a definitive radio-chemotherapy based on cisplatin 40 mg/m2/weekly as treatment. The case report is about the radiation treatment planning of the patient’s cervical cancer.
Radiation Treatment Planning
Given the advanced stage of the disease and the limited treatment options including the huge fibroid which the surgical team did not want to remove. There were also difficulties determining where the tumor ends superiorly so a decision was taken to treat the cervix including the huge fibroid since it could not be differentiated from the true cervix. The treatment regimen included whole pelvis radiotherapy 2 Gy x 23 fractions for a total of 46 Gy. This was followed by a boost radiotherapy to the cervix of 30 Gy in 10 fractions. The whole pelvis plan was a 7 fields Intensity Modulated Radiation Therapy (IMRT) generated using the Eclipse Treatment Planning System (version 15.6.8). The major constraints were to ensure that 95% of PTV46 gets 95% of the prescribed dose and allow the center of the PTV46 to get maximum dose of up 20% rather than the typical 5-10% hot spot in most IMRT plans. We also limit D2cc for the rectum, sigmoid, bowel space to be less than 43Gy. For the boost plan, PTV76, which is the boost volume (cervix +5mm margin) was divided into 2 additional boost volumes, PTV76-1cm (negative margin of 1 cm from PTV76 to form PTV81Gy and PTV86Gy which is PTV76-2cm. The boost plan was also generated with the Eclipse Treatment Planning System with a 5 fields IMRT technique. The clinical radiotherapy planning objectives for PTV76 and OARs was to limit D2cc for the rectum, sigmoid, bowel space to be less than 27Gy so that D2cc for the rectum, sigmoid and small bowels for the whole pelvis and boost irradiation was not more than 75Gy (EQD2). It is important to note that the boost plan was generated with a second CT scan which was acquired 4 weeks after the commencement of the external beam radiation for the whole pelvis IMRT. The old images were fused with new images and relevant structure copied onto the new CT scan and modified as necessary.
Results
Figure 2 shows the color wash of the total dose distribution and the dose volume histogram. The physical dose received by the patient is 46Gy (2Gy x 23) for the whole pelvis dose plus 30 Gy (3 Gy x 10) for a total of 76Gy to PTV76. But in terms EQD2, the calculated value for the PTV76 is D95=78Gy as shown in Table 1. D2cc for the rectum, sigmoid and bladder were 70.6, 59.6 and 90.6 respectively. Because the tumor had invaded the bladder, we allow the posterior bladder wall to receive a higher dose and this resulted into EQD2 of 90.4Gy above 0.4Gy above the tolerance suggested by the American Brachytherapy society.
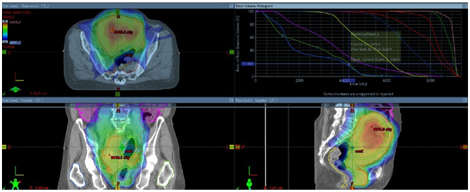
Figure 2: Total dose distribution (whole pelvis plus cervix boost)
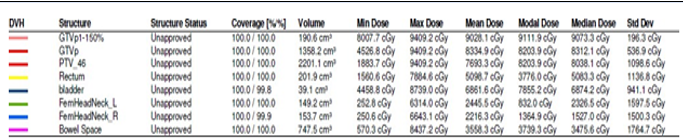
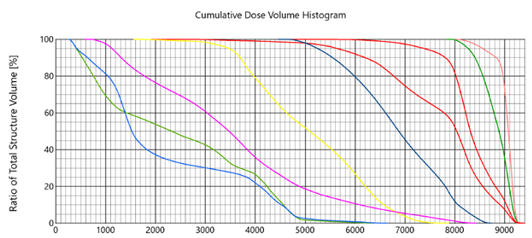
Figure 3: Dose volume histogram for total dose (whole pelvis plus cervix boost)
Table 1: shows the numerical analysis of the plans for this patient
| Organ | Physical dose | α/β ratio | EQD2 | Total |
| PTV46 | 2 Gy x23 = 46Gy | 10 | 46 Gy | 46 Gy |
| PTV76 | 3 Gy x10 = 30 | 10 | 32 Gy | 78 Gy |
| PTV76-1cm | 3.3Gy x 10 | 10 | 35.8 Gy | 81 Gy |
| PTV76-2cm | 3.7 Gy x10 | 10 | 40.1 Gy | 86 Gy |
| D2cc for organ at risks | ||||
| Sigmoid | 1.7Gyx23(whole pelvis) | 3 | 36.8 | 59.6 (EQD2) |
| Sigmoid | 2.2 Gy x10(boost plan) | 3 | 22.8 | |
| Rectum | 1.8 Gy x 23(whole pelvis) | 3 | 39.8 | 70.6 (EQD2) |
| Rectum | 2.7Gy x10 (boost plan) | 3 | 30.8 | |
| Bladder | 2.2 Gy x 23 (whole pelvis) | 3 | 52.6 | 90.4 (EQD2) |
| Bladder | 3.1 Gy x 10 (boost plan) | 3 | 37.8 | |
Outcome and Follow-up
Throughout the treatment course, the patient did not experience any significant side effects but did have grade 1 dermatitis, grade 1 cystitis, and grade 1 proctitis but did not miss treatment because of side effects issue. The patient came for 1 month post radiotherapy follow-up visit and was doing well total hysterectomy was performed by a gynecologist at another medical institution before her scheduled 3 months follow up with us. Postoperative histopathology revealed complete response to therapy (pT0N0), she continues to follow up with us for post treatment surveillance and survivorship visits, regular scans are done to monitor disease recurrence/progression, manage treatment-related complications, and provide supportive care.
Discussion
Using the treatment planning described here which is based on creating sub PTV (PTV76-1cm) and PTV76-2cm) within the main PTV. Using inverse optimization, the dose in the core of the tumor is increase between 20 and 30% and at the same limit not exceeding the tolerance doses for the risk organs. Such technique is designed to increase cancer disease control rate and at the same time limit morbidity. The patient completed treatment without stopping but later underwent a total hysterectomy with total appendectomy. The case highlights the complexities associated with managing cervical cancer in resource-limited settings like Cameroon where there is no active brachytherapy program. Limited access to screening programs, diagnostic facilities, and specialized treatment modalities poses significant challenges to early detection and optimal management. It has been observed that more than half of our cervical cancer patients were not screened, never even with had Pap smear. Multidisciplinary collaboration, patient education, and integration of palliative care are essential components of a comprehensive approach to cervical cancer care in such settings. Cervical cancer management often involved the use of high dose rate brachytherapy to boost cervix after external beam to the entire pelvis but Cameroon does not have any high dose rate brachytherapy system and Cameroon Oncology Center does not have access any Low Dose rate brachytherapy System. Cameroon Oncology Center has over the past 5 years developed a cervical cancer radiation boost techniques to increase the dose to the cervix after whole pelvis irradiation. This technique often involves creating high dose region within the cervix but at the same time keeping the risk organ doses below common standard dose restriction use around the world where the D2cc for all the risk organs (rectum, bladder, sigmoid) is below 75Gy and the bladder dose below 90Gy. (EQD2). With this particular patient, we were able to achieve an overall D90 of the cervix of 80Gy.
The incorporation of this planning technique of making the center of the tumor hotter dosimetrically than the periphery can be considered a form of “fractionated” spatially fractionated radiotherapy which is based on creating regions of cold and hot spot with the tumor volume. Our technique is instead based on creating two zones of 120% and 133% of the prescription dose within the tumor volume especially in the core where the cells are likely necrotic and likely radio- resistant. This radiation treatment planning technique mimic what happens with brachytherapy plans where the dose near the applicator is very high with significant volume of the tumor closer to the applicator receiving a dose that is up to 4 times higher than the prescription dose.
Conclusion
Cervical cancer remains a formidable health challenge in Cameroon and other resource limited settings, necessitating concerted efforts to improve access to screening, HPV vaccination, and treatment services. The case underscores the importance of a multidisciplinary approach, patient- centered care, and resource optimization in addressing the burden of cervical cancer and improving patient outcomes at the Cameroon Oncology Center and similar facilities worldwide.
Declarations
Funding
Nil, no funding required.
Availability of data and materials
Can be shared from patient file, if required.
Competing interests
The authors declare that they have no competing interests.
References
- Cervical cancer: Epidemiology, risk factors and screening – PMC.
Publisher | Google Scholor - Cancer cervix: Epidemiology and disease burden – PMC.
Publisher | Google Scholor - Cervical cancer screening prevalence and its correlates in Cameroon: secondary data analysis of the 2018 demographic and health surveys, BMC Public Health.
Publisher | Google Scholor - A scoping review of facilitators and barriers to implementation and uptake of screening – PMC.
Publisher | Google Scholor - A Case Report of Advanced Cervical Cancer in a Patient Non-compliant With Age- Appropriate Screening – PMC.
Publisher | Google Scholor - Risk Factors of Cervical Cancer: A Case-Control Study – PMC.
Publisher | Google Scholor - Assessment of the current state of knowledge and risk factors of cervical cancer among women in the Buea Health District, Cameroon – PMC.
Publisher | Google Scholor - Viswanathan, et al. (2012). The American Brachytherapy Society Treatment Recommendations for Locally Advanced Carcinoma of the Cervix Part II: High Dose-Rate Brachytherapy. Brachytherapy. 11(1):47-52.
Publisher | Google Scholor













