

Research Article
Utilization Patterns and Determinants of Levonorgestrel-Based Emergency Contraception (Postinor) Use Among Women of Reproductive Age
1 Department of Obstetrics and Gynaecology, Abia State University Teaching Hospital, Aba, Nigeria.
2 Babcock University Teaching Hospital, Ilishan-Remo, Ogun, Nigeria.
3 Department of Obstetrics and Gynaecology, Rhema University Teaching Hospital, Aba, Abia, Nigeria.
4 Department of Biochemistry, Lead City University, Ibadan, Oyo, Nigeria.
*Corresponding Author: Emmanuel M. Akwuruoha, Department of Obstetrics and Gynaecology, Abia State University Teaching Hospital, Aba, Nigeria.
Citation: Emmanuel M. Akwuruoha, David O. Akwuruoha, Chisara C. Umezurike, Augustine I. Airaodion. (2026). Utilization Patterns and Determinants of Levonorgestrel-Based Emergency Contraception (Postinor) Use Among Women of Reproductive Age, Clinical Obstetrics and Gynecology Research, BioRes Scientia Publishers. 5(1):1-11. DOI: 10.59657/2992-9725.brs.26.028
Copyright: © 2026 Emmanuel M. Akwuruoha, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 14, 2026 | Accepted: June 10, 2026 | Published: June 25, 2026
Abstract
Background: Emergency contraception, particularly levonorgestrel-based products such as Postinor, plays a critical role in preventing unintended pregnancies. Despite its availability, patterns of use and the factors influencing utilization among women in Nigeria remain uneven and not fully understood. This study assessed the utilization patterns and determinants of Postinor use among women of reproductive age in Aba, Abia State.
Materials and Methods: A descriptive cross-sectional study was conducted among 375 women aged 15–49 years using a multistage sampling technique. Data were collected with a structured, pre-tested questionnaire covering socio-demographic characteristics, patterns of Postinor use, knowledge, accessibility, and influencing factors. Descriptive statistics summarized the data, while chi-square tests and logistic regression were used to examine associations and predictors. Statistical significance was set at p < 0.05.
Results: The mean age distribution was skewed toward younger women, with the highest proportion aged 25–29 years (25.9%). Overall, 71.5% of respondents reported having ever used Postinor, and 69.8% of users had used it within the past 12 months. Most users reported occasional use (51.5%), although 29.1% identified as regular or repeated users, and 35.8% reported multiple use within the same menstrual cycle. The most common reasons for use were unprotected intercourse (67.9%) and fear of pregnancy (58.2%). Pharmacies (51.1%) and patent medicine vendors (30.6%) were the primary sources, with 79.8% reporting easy or very easy access. Significant associations were observed between Postinor use and age (p = 0.005), marital status (p = 0.001), education (p = 0.001), and occupation (p = 0.029). Knowledge (r = 0.42), accessibility (r = 0.36), and peer influence (r = 0.31) showed positive correlations with use, while fear of side effects (r = -0.28) and cost (r = -0.33) were negatively correlated. Key predictors of use included age 20–29 years (OR = 1.84), tertiary education (OR = 2.31), easy access (OR = 2.67), and good knowledge (OR = 1.92), whereas fear of side effects reduced the likelihood of use (OR = 0.63).
Conclusion: Postinor use is widespread among women in Aba, with notable patterns of repeated and occasional use. Utilization is strongly influenced by knowledge, accessibility, and socio-demographic factors. Addressing misconceptions about side effects, improving education on appropriate use, and promoting consistent contraceptive practices are essential to optimize safe and effective use.
Keywords: emergency contraception; postinor; utilization patterns; reproductive health; levonorgestrel
Introduction
The issue of unintended pregnancy remains a major public health concern globally, particularly in low- and middle-income countries where access to effective and consistent contraceptive methods is often limited [1]. Emergency contraception (EC), especially levonorgestrel-based formulations such as Postinor, plays a critical role as a “last-resort” intervention to prevent pregnancy following unprotected sexual intercourse, contraceptive failure, or sexual assault. Levonorgestrel emergency contraceptive pills (LNG-ECPs) act primarily by delaying or inhibiting ovulation when taken within a specified time window, typically within 72 hours, although some effectiveness may extend up to 120 hours post-exposure [2]. Their availability without prescription in many settings has positioned them as a vital component of reproductive health services, particularly among women of reproductive age.
In Nigeria, the burden of unintended pregnancy is notably high, driven by low contraceptive prevalence, inconsistent use of regular contraceptive methods, and sociocultural barriers to family planning [3,4]. Evidence suggests that only a small proportion of sexually active women consistently use modern contraceptives, contributing to high rates of unsafe abortion and associated maternal morbidity and mortality [5]. Emergency contraception therefore serves as an important backup method in preventing unintended pregnancies in contexts where regular contraceptive use is inadequate or unreliable. Despite its clinical effectiveness, utilization of levonorgestrel-based emergency contraception remains suboptimal in many parts of Nigeria.
Several studies conducted among Nigerian women have revealed relatively low levels of awareness and utilization of emergency contraception, including Postinor. For instance, a study among university students reported that only 17.6% of respondents had ever used levonorgestrel-based emergency contraception, despite a higher proportion engaging in unprotected sexual activity [6]. This gap between sexual risk exposure and EC utilization highlights persistent barriers such as misinformation, stigma, fear of side effects, and limited access to accurate reproductive health information. Misconceptions about the safety of Postinor, including beliefs that it may cause infertility or long-term reproductive harm, continue to influence attitudes and discourage appropriate use.
Beyond awareness, multiple socio-demographic and behavioral factors have been shown to influence the utilization of levonorgestrel emergency contraception. These include age, level of education, marital status, socioeconomic status, and knowledge of the correct timing and mechanism of action of EC. Research indicates that awareness of EC, perception of pregnancy risk, and educational level are significantly associated with its use [7]. Younger women, particularly adolescents and university students, may exhibit higher awareness but not necessarily higher correct usage, often resorting to inappropriate alternatives such as non-emergency contraceptive pills or traditional concoctions due to misinformation or accessibility issues [8].
Cultural and religious norms also play a significant role in shaping contraceptive behaviors in Nigeria. In many communities, discussions around sexuality and contraception remain sensitive, limiting open access to reproductive health education. Women may face judgment or stigma when seeking emergency contraception, especially unmarried women, thereby influencing their decision-making and utilization patterns. In addition, health system factors such as availability of EC products, affordability, quality of counselling services, and attitudes of healthcare providers further determine access and proper use.
In the context of Abia State, these challenges may be even more pronounced due to variations in urban–rural distribution, healthcare infrastructure, educational attainment, and cultural practices [9]. While urban areas such as Aba may have relatively better access to pharmacies and health facilities where Postinor is available, rural communities may experience significant barriers, including limited availability, poor health literacy, and reliance on informal sources of reproductive health information. Furthermore, the widespread availability of levonorgestrel-based EC over the counter has led to concerns about misuse, repeated use without proper guidance, and substitution with ineffective or unsafe alternatives.
Understanding the utilization patterns and determinants of Postinor use among women of reproductive age in Abia State is therefore essential for designing targeted interventions aimed at improving reproductive health outcomes. Such understanding will provide insights into who uses emergency contraception, under what circumstances, and the factors influencing their decisions. It will also help identify gaps in knowledge, misconceptions, and systemic barriers that need to be addressed through policy, education, and health service delivery.
Given the critical role of emergency contraception in reducing unintended pregnancies and unsafe abortions, there is a need for context-specific evidence that reflects the realities of women in Abia State. This study is therefore justified in its attempt to explore the patterns of use and determinants of levonorgestrel-based emergency contraception (Postinor), with the ultimate goal of informing public health strategies, improving access to accurate information, and promoting safe and effective contraceptive practices among women of reproductive age.
Materials and Methods
Study Design
A descriptive cross-sectional study design was adopted. This approach allowed for the systematic assessment of utilization patterns, knowledge, attitudes, and determinants of Postinor use among women of reproductive age at a single point in time. The design was considered appropriate for identifying associations between socio-demographic, behavioral, and accessibility factors and the use of emergency contraception.
Study Area
The study was conducted in Aba, a major commercial hub located in southeastern Nigeria. Aba is characterized by a dense population, vibrant informal and formal economic activities, and a mix of urban and semi-urban settlements. The city hosts a wide range of healthcare facilities, including public hospitals, private clinics, pharmacies, and Patent Medicine Vendors (PMVs), which serve as common sources of reproductive health services and emergency contraceptives. Its cosmopolitan nature and active reproductive-age population make it a suitable setting for assessing patterns of emergency contraceptive use.
Study Population
The study population comprised women of reproductive age (15–49 years) residing in Aba. Eligible participants included sexually active women within this age range who were present in selected communities or health-related outlets during the study period. Women who were severely ill, unwilling to participate, or unable to provide informed consent were excluded.
Sample Size Determination
The sample size was determined using Cochran's formula for estimating population proportions, as outlined by Akwuruoha et al. [10]:
n = 
The formula components are defined as follows:
n represents the minimum required sample size.
Z is set at 1.96, corresponding to a 95% confidence level.
P denotes the estimated proportion of awareness of emergency contraception in Nigeria.
e signifies the allowable margin of error, fixed at 5% (0.05).
q = 1 - p
A recent study conducted by Adewale et al. [11] reported the estimated proportion of awareness of emergency contraception in Nigeria as 33.3%
P = 33.3% = 0.333
q = 1 – 0.333
= 0.667
n = 
n = 
n =  = 341.30
= 341.30
To account for non-response and incomplete questionnaires, an additional 10% was added, bringing the total sample size to approximately 375 respondents.
Sampling Technique
A multistage sampling technique was employed to ensure representativeness. In the first stage, Aba was stratified into its major local government areas (Aba North and Aba South). In the second stage, selected communities and wards were randomly chosen from each LGA. The third stage involved purposive selection of locations with high female patronage, such as markets, schools, healthcare facilities, pharmacies, and PMV outlets. Finally, eligible respondents were selected using systematic or convenience sampling, depending on the flow of participants at each site.
Study Instrument
Data were collected using a structured, pre-tested questionnaire developed specifically for this study. The instrument was designed in English and structured into eleven sections (A–K), covering:
Socio-demographic characteristics
Prevalence of Postinor use
Frequency and patterns of use
Indications for use
Accessibility and sources
Knowledge about Postinor
Social and behavioral influences
Attitudes toward use
Barriers and predictors
Reproductive history
Overall perception
The questionnaire included both closed-ended questions and Likert-scale items to capture nuanced responses. It was self-administered for literate participants, while trained research assistants assisted respondents with limited literacy through interviewer administration.
Validity and Reliability of Instrument
Content validity was ensured through expert review by professionals in public health, reproductive health, and epidemiology. Their input helped refine the clarity, relevance, and comprehensiveness of the instrument.
A pilot study was conducted among approximately 10% of the sample size in a similar population outside the selected study areas. Feedback from the pilot informed necessary adjustments. The reliability of the questionnaire was assessed using Cronbach’s alpha for Likert-scale items, yielding a coefficient of ≥0.7, indicating acceptable internal consistency.
Data Collection Procedure
Data collection was carried out over a period of 4–6 weeks by trained research assistants. Prior to data collection, assistants underwent training on the study objectives, ethical considerations, and administration of the questionnaire.
Participants were approached in selected locations, the purpose of the study was explained, and informed consent was obtained. Questionnaires were then administered in a private and confidential manner to encourage honest responses. Completed questionnaires were checked daily for completeness and consistency.
Study Variables
Dependent Variable: Utilization of Postinor (ever use, recent use, frequency, and pattern of use).
Independent Variables: Socio-demographic factors (age, education, income, marital status), knowledge, accessibility, cost, social influences (peer, partner, healthcare providers), attitudes, reproductive history, and perceived barriers.
Data Management and Analysis
Data were coded, entered, and analyzed using Statistical Package for the Social Sciences (SPSS) version 25. Descriptive statistics such as frequencies, percentages, means, and standard deviations were used to summarize the data. Inferential statistics were applied to determine associations between variables. Chi-square test was used to examine relationships between categorical variables. Logistic regression analysis was performed to identify independent predictors of Postinor use. Statistical significance was set at p < 0>
Ethical Considerations
Permission was also sought from relevant local authorities and facility managers where applicable. Participation was entirely voluntary, and informed consent was obtained from all respondents before data collection. For participants aged 15–17 years, assent was obtained alongside parental or guardian consent where required. Confidentiality and anonymity were strictly maintained. No personal identifiers were collected, and all data were used solely for research purposes.
Limitations of the Study
The cross-sectional nature of the study limits the ability to establish causality. Responses were self-reported and may be subject to recall bias or social desirability bias, particularly given the sensitive nature of contraceptive use. However, efforts such as ensuring anonymity and privacy during data collection helped minimize these limitations.
Results
The socio-demographic profile of respondents shows that the largest proportion were aged 25–29 years (25.9%), followed by those aged 20–24 years (22.9%), while the least represented group was 45–49 years (4.8%). Most respondents were single (44.8%) or married (39.7%). In terms of education, a higher proportion had tertiary education (42.1%), followed by secondary education (37.9%). Students constituted the largest occupational group (29.9%), and the majority identified as Christians (71.5%) (Table 1).
Regarding Postinor use, a substantial proportion of respondents (71.5%) reported ever using it, with most initiating use between ages 18–24 years (48.1%). Among users, 69.8% had used Postinor within the last 12 months (Table 2). Patterns of use indicate that most respondents used Postinor rarely (36.2%) or occasionally (27.2%), while 14.9% reported frequent use. In the last six months, the majority used it 1–2 times (38.8%), and over half classified their usage as occasional (51.5%). Additionally, 35.8% reported multiple use within the same menstrual cycle (Table 3).
The most common reasons for use included unprotected intercourse (67.9%), fear of pregnancy (58.2%), and condom failure (45.1%), while fewer respondents reported use following sexual assault (4.1%) (Table 4). Confidence levels in using Postinor were generally high, with 34.3 % being very confident and 38.8% confident, whereas a smaller proportion expressed uncertainty or lack of confidence (Figure 1). Pharmacies were the main source of Postinor (51.1%), followed by patent medicine vendors (30.6%). Most respondents indicated that a prescription was not required (65.7%), and access was largely perceived as easy or very easy (79.8%) (Table 5).
Peer influence appeared notable, with over half of respondents either agreeing (32.3%) or strongly agreeing (23.2%) that peers influenced their use, while fewer disagreed (Figure 2). Key barriers identified included fear of side effects (43.5%), cost (38.4%), and lack of knowledge (25.9%), alongside other factors such as partner disapproval and cultural norms (Table 6).
In terms of reproductive characteristics, 60.3% of respondents had ever been pregnant, and 36.8% reported unintended pregnancy. Regular contraceptive use varied, with 24.0% always using contraceptives and 25.6% never using them (Table 7). Statistical analysis revealed significant associations between Postinor use and age group, marital status, education, and occupation (p < 0.05), while religion showed no significant association (Table 8).
Correlation analysis demonstrated moderate positive relationships between knowledge and frequency of use (r = 0.42), as well as positive associations with accessibility and peer influence. Negative correlations were observed with fear of side effects and cost (Table 9). Logistic regression identified age (20–29 years), tertiary education, ease of access, and good knowledge as significant predictors of Postinor use, while fear of side effects was associated with reduced likelihood of use (Table 10). Cross-tabulation showed increasing Postinor use with higher levels of education, with the highest usage observed among respondents with tertiary education (79.1%) and the lowest among those with no formal education (42.9%) (Table 11).
Table 1: Socio-Demographic Characteristics of Respondents
| Variable | Frequency (n) | Percentage (%) |
| Age Group | ||
| 15–19 years | 42 | 11.2 |
| 20–24 years | 86 | 22.9 |
| 25–29 years | 97 | 25.9 |
| 30–34 years | 63 | 16.8 |
| 35–39 years | 41 | 10.9 |
| 40–44 years | 28 | 7.5 |
| 45–49 years | 18 | 4.8 |
| Marital Status | ||
| Single | 168 | 44.8 |
| Married | 149 | 39.7 |
| Cohabiting | 29 | 7.7 |
| Divorced/Separated | 17 | 4.5 |
| Widowed | 12 | 3.2 |
| Educational Level | ||
| No formal education | 21 | 5.6 |
| Primary | 54 | 14.4 |
| Secondary | 142 | 37.9 |
| Tertiary | 158 | 42.1 |
| Occupation | ||
| Student | 112 | 29.9 |
| Unemployed | 47 | 12.5 |
| Self-employed | 86 | 22.9 |
| Civil servant | 51 | 13.6 |
| Private sector | 62 | 16.5 |
| Other | 17 | 4.5 |
| Religion | ||
| Christianity | 268 | 71.5 |
| Islam | 89 | 23.7 |
| Traditional | 11 | 2.9 |
| Other | 7 | 1.9 |
Table 2: Prevalence of Postinor Use
| Variable | Frequency (n) | Percentage (%) |
| Ever used Postinor | ||
| Yes | 268 | 71.5 |
| No | 107 | 28.5 |
| Age at first use (n = 268) | ||
| <18> | 46 | 17.2 |
| 18–24 years | 129 | 48.1 |
| 25–30 years | 71 | 26.5 |
| >30 years | 22 | 8.2 |
| Used in last 12 months (n = 268) | ||
| Yes | 187 | 69.8 |
| No | 81 | 30.2 |
Table 3: Frequency and Patterns of Use (n = 268)
| Variable | Frequency (n) | Percentage (%) |
| Frequency of use | ||
| Once ever | 58 | 21.6 |
| Rarely (1–2/year) | 97 | 36.2 |
| Occasionally (3–5/year) | 73 | 27.2 |
| Frequently (>5/year) | 40 | 14.9 |
| Use in last 6 months | ||
| 0 times | 61 | 22.8 |
| 1–2 times | 104 | 38.8 |
| 3–4 times | 66 | 24.6 |
| ≥5 times | 37 | 13.8 |
| Self-classification of use | ||
| One-time | 52 | 19.4 |
| Occasional | 138 | 51.5 |
| Regular/Repeated | 78 | 29.1 |
| Multiple use in same cycle | ||
| Yes | 96 | 35.8 |
| No | 172 | 64.2 |
Table 4: Indications for Use (Multiple responses)
| Variable | Frequency (n) | Percentage (%) |
| Unprotected intercourse | 182 | 67.9 |
| Condom failure | 121 | 45.1 |
| Missed pills | 74 | 27.6 |
| Sexual assault | 11 | 4.1 |
| Miscalculation of safe period | 98 | 36.6 |
| Fear of pregnancy | 156 | 58.2 |
| Partner refusal | 63 | 23.5 |
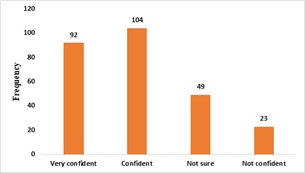
Figure 1: Confidence in use of Postinor (n = 268)
Table 5: Accessibility and Sources
| Variable | Frequency (n) | Percentage (%) |
| Source of Postinor | ||
| Pharmacy | 137 | 51.1 |
| PMV | 82 | 30.6 |
| Hospital | 21 | 7.8 |
| Friends | 18 | 6.7 |
| Online | 10 | 3.7 |
| Prescription required | ||
| Yes | 47 | 17.5 |
| No | 176 | 65.7 |
| Not sure | 45 | 16.8 |
| Ease of access | ||
| Very easy | 121 | 45.1 |
| Easy | 93 | 34.7 |
| Neutral | 28 | 10.4 |
| Difficult | 19 | 7.1 |
| Very difficult | 7 | 2.6 |
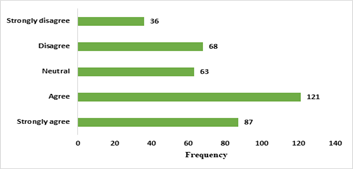
Figure 2: Social (Peer) Influence on Postinor Usage
Table 6: Barriers to using Postinor (Multiple responses)
| Variable | Frequency (n) | Percentage (%) |
| Cost | 144 | 38.4 |
| Lack of access | 79 | 21.1 |
| Fear of side effects | 163 | 43.5 |
| Religious beliefs | 61 | 16.3 |
| Cultural norms | 74 | 19.7 |
| Partner disapproval | 88 | 23.5 |
| Lack of knowledge | 97 | 25.9 |
Table 7: Reproductive and Contraceptive Characteristics of Respondents
| Variable | Response Option | Frequency (n) | Percentage (%) |
| Ever pregnant | Yes | 226 | 60.3 |
| No | 149 | 39.7 | |
| Unintended pregnancy | Yes | 138 | 36.8 |
| No | 237 | 63.2 | |
| Use of regular contraceptive | Never | 96 | 25.6 |
| Rarely | 54 | 14.4 | |
| Sometimes | 46 | 12.3 | |
| Often | 89 | 23.7 | |
| Always | 90 | 24.0 |
Table 8: Association between Socio-demographic variables and Postinor Use
| Variable | χ² | df | p-value | Interpretation |
| Age group vs Use | 18.72 | 6 | 0.005 | Significant |
| Marital status vs Use | 22.91 | 4 | 0.001 | Significant |
| Education vs Use | 16.38 | 3 | 0.001 | Significant |
| Occupation vs Use | 12.44 | 5 | 0.029 | Significant |
| Religion vs Use | 5.83 | 3 | 0.120 | Not significant |
Table 9: Correlation Analysis
| Variables | r-value | p-value | Interpretation |
| Knowledge vs Use frequency | 0.42 | 0.001 | Moderate positive |
| Accessibility vs Use | 0.36 | 0.002 | Positive |
| Peer influence vs Use | 0.31 | 0.004 | Positive |
| Fear of side effects vs Use | -0.28 | 0.006 | Negative |
| Cost vs Use | -0.33 | 0.003 | Negative |
Table 10: Logistic Regression (Predictors of Postinor Use)
| Variable | Odds Ratio (OR) | 95% CI | p-value |
| Age (20–29) | 1.84 | 1.21–2.79 | 0.003 |
| Tertiary education | 2.31 | 1.48–3.62 | 0.001 |
| Easy access | 2.67 | 1.73–4.11 | 0.000 |
| Good knowledge | 1.92 | 1.28–2.88 | 0.002 |
| Fear of side effects | 0.63 | 0.41–0.97 | 0.036 |
Table 11: Cross-Tab: Education Vs Postinor Use
| Education | Used (%) | Not Used (%) |
| No formal | 9 (42.9) | 12 (57.1) |
| Primary | 31 (57.4) | 23 (42.6) |
| Secondary | 103 (72.5) | 39 (27.5) |
| Tertiary | 125 (79.1) | 33 (20.9) |
Discussion
Emergency contraception, particularly levonorgestrel-based formulations such as Postinor, plays a critical role in preventing unintended pregnancies. Despite its availability in Nigeria, patterns of use and the factors influencing its utilization remain insufficiently explored, especially in rapidly urbanizing settings like Aba, Abia State. This study assessed the utilization patterns and determinants of Postinor use among women of reproductive age in Aba, Abia State, Nigeria.
The socio-demographic profile of respondents (Table 1) shows a predominance of young adults, especially those aged 20–29 years, with relatively high levels of education and a substantial proportion being single. This aligns closely with earlier Nigerian studies which consistently report that emergency contraceptive use is highest among younger, unmarried, and educated women. For instance, a study among university students in Nigeria found that emergency contraception uptake increased with age and educational level, reflecting greater exposure to reproductive health information and autonomy in decision-making [6]. The high proportion of respondents with tertiary education in the present study may partly explain the relatively high utilization observed, as education has been repeatedly shown to enhance awareness, comprehension, and acceptance of contraceptive methods.
A striking finding in this study is the high prevalence of Postinor use (71.5%) (Table 2), which is substantially higher than figures reported in earlier Nigerian studies. Previous research documented much lower usage rates, such as 17.6% among university students and 31% in another cohort of undergraduates [6]. Even broader reviews across sub-Saharan Africa suggest that emergency contraceptive use rarely exceeds 54% [12]. The markedly higher prevalence observed in this study likely reflects increasing awareness, improved availability, and normalization of emergency contraception in recent years. It may also indicate a shift in reproductive behaviour, where women are becoming more proactive in preventing unintended pregnancies following unprotected intercourse. The increased usage of postinor and other contraceptives might be responsible for the reduction in the rate of unwanted pregnancy in Nigeria in recent times. For example, in 2015 Lamina [13] reported the prevalence of unwanted pregnancy as 35.9%, while in 2024, Ashimi et al. [14] reported a prevalence of 10.0%.
The age at first use, predominantly between 18 and 24 years, is consistent with findings from previous studies that identify late adolescence and early adulthood as critical periods for sexual debut and contraceptive experimentation. This reinforces the importance of targeting reproductive health education at younger populations before or during this transition phase. Additionally, the high proportion of respondents who reported using Postinor within the last 12 months suggests that emergency contraception is not only known but actively utilized when needed, contrasting with earlier reports where awareness did not necessarily translate into practice [2].
Patterns of use (Table 3) indicate that while most respondents classify their use as occasional, a notable proportion engage in repeated or frequent use, including multiple uses within the same menstrual cycle. This finding is particularly important because earlier qualitative studies in Nigeria have highlighted misuse and alternative uses of Postinor, including attempts to induce menstruation or terminate pregnancy [15]. Although the present study does not directly assess misuse, the observed frequency patterns raise concerns about potential reliance on emergency contraception as a substitute for regular contraceptive methods. This is further supported by the reproductive characteristics data, where a considerable proportion of respondents reported inconsistent or non-use of regular contraception.
The indications for use (Table 4), dominated by unprotected intercourse, fear of pregnancy, condom failure, and miscalculation of the safe period, are consistent with established literature. Previous Nigerian studies have similarly identified condom failure and missed pills as major triggers for emergency contraceptive use, reflecting gaps in consistent contraceptive practice [16]. The relatively low proportion reporting use following sexual assault is also consistent with other studies, although this may be influenced by underreporting due to stigma and cultural barriers.
Confidence in the use of Postinor (Figure 1) appears relatively high, with over 70% of users expressing confidence or strong confidence. This contrasts with earlier findings where misconceptions about timing, effectiveness, and safety were widespread. For example, previous research found that many women lacked accurate knowledge of the correct timeframe for emergency contraception use [2]. The higher confidence observed in this study may reflect improved health communication and peer-to-peer information sharing.
Accessibility findings (Table 5) reveal that pharmacies and patent medicine vendors (PMVs) are the primary sources of Postinor, and that the majority of respondents perceive access as easy and not requiring a prescription. This aligns with existing evidence that emergency contraceptive pills in Nigeria are widely available over the counter [8]. While this ease of access likely contributes to the high utilization observed, it also raises concerns about unsupervised use and the potential for misinformation, especially in informal settings such as PMVs.
The role of peer influence (Figure 2) is also noteworthy, with over half of respondents acknowledging its impact on their use of Postinor. This finding is consistent with earlier studies where peers were identified as major sources of information and influence regarding contraceptive use [2]. The positive correlation between peer influence and use frequency (Table 9) further underscores the importance of social networks in shaping reproductive health behaviours.
Barriers identified in this study (Table 6), particularly fear of side effects, cost, and lack of knowledge, are consistent with previous literature. Fear of adverse effects has long been recognized as a major deterrent to contraceptive use in Nigeria, often fueled by misconceptions about infertility and long-term health consequences [17]. The negative correlation between fear of side effects and use frequency reinforces the need for accurate, evidence-based education to dispel myths and improve informed decision-making.
The reproductive profile of respondents reveals a relatively high prevalence of unintended pregnancy (36.8%), which is consistent with national concerns about unintended pregnancies and their associated health risks. Earlier studies have linked low regular contraceptive use and high rates of contraceptive failure to the persistent burden of unintended pregnancies in Nigeria [16]. The coexistence of high emergency contraceptive use and substantial unintended pregnancy rates suggests that emergency contraception is being used reactively rather than as part of a comprehensive contraceptive strategy.
The association analysis (Table 8) shows that age, marital status, education, and occupation are significant determinants of Postinor use, while religion is not. These findings are largely consistent with previous studies, which have identified socio-demographic factors, particularly education and age, as key predictors of contraceptive use. The lack of association with religion may indicate a gradual shift away from religious constraints in contraceptive decision-making, or it may reflect the overriding influence of practical considerations such as access and perceived risk.
The correlation and regression analyses (Tables 9 and 10) provide further insight into the determinants of use. The positive influence of knowledge, accessibility, and peer influence aligns with existing evidence, while the negative impact of cost and fear of side effects highlights persistent structural and perceptual barriers. The strong predictive effect of tertiary education, good knowledge, and easy access is consistent with findings from other Nigerian studies that emphasize the role of education and information in shaping contraceptive behaviour [6].
The cross-tabulation between education and use (Table 11) demonstrates a clear gradient, with higher levels of education associated with increased use of Postinor. This reinforces the central role of education in empowering women to make informed reproductive health decisions and aligns with broader evidence from sub-Saharan Africa that links educational attainment with improved contraceptive uptake [12].
Conclusion
This study highlights a notable increase in the utilization of levonorgestrel-based emergency contraception in Abia State compared to earlier Nigerian studies, alongside evolving patterns of use and persistent barriers. The findings suggest that while access and awareness have improved, there remains a need to promote appropriate use, integrate emergency contraception within a broader contraceptive framework, and address misconceptions that continue to influence utilization behaviours.
References
- Ezirim, E. O., Akwuruoha, E. M., Amah, C. I., Onyemereze, C. O., & Airaodion, A. I. (2025). Knowledge, attitude and perception towards premature ovarian insufficiency among Nigerian women. International Journal of Clinical Gynaecology and Obstetrics, 5(1):1–7.
Publisher | Google Scholor - Awoleke, J. O., Adanikin, A. I., Awoleke, A., & Odanye, M. (2015). Awareness and practice of emergency contraception at a private university in Nigeria. BMC Research Notes, 8:215.
Publisher | Google Scholor - Ezirim, E. O., Omole, O. R., Akwuruoha, E. M., Ejikem, P. I., & Airaodion, A. I. (2023). Factors influencing family planning services among rural women in Nigeria. International Journal of Research and Reports in Gynaecology, 6(1):54–66.
Publisher | Google Scholor - Ezebuiro, E. I., Abali, I. O., Akenroye, S. G., Onyemereze, C. O., & Airaodion, A. I. (2025). The role of male involvement in family planning and contraceptive use in Nigeria. Journal of Counselling and Family Therapy, 7(1):30–37.
Publisher | Google Scholor - Dada, O. A., Godfrey, E. M., Piaggio, G., & Von Hertzen, H. (2010). A randomized, double-blind, noninferiority study to compare two regimens of levonorgestrel for emergency contraception in Nigeria. Contraception, 82(4):373-378.
Publisher | Google Scholor - Ajayi, A. I., Nwokocha, E. E., Adeniyi, O. V., Goon, D. T., & Akpan, W. (2017). Unplanned pregnancy—Risks and use of emergency contraception: A survey of two Nigerian universities. BMC Health Services Research, 17:382.
Publisher | Google Scholor - Arowojolu, A. O., Okewole, I. A., & Adekunle, A. O. (2002). Comparative evaluation of the effectiveness and safety of two regimens of levonorgestrel for emergency contraception in Nigerians. Contraception, 66(4):269–273.
Publisher | Google Scholor - Ajayi, A. I., Nwokocha, E. E., Akpan, W., & Adeniyi, O. V. (2016). Use of non-emergency contraceptive pills and concoctions as emergency contraception among Nigerian University students: results of a qualitative study. BMC public health, 16(1):1046.
Publisher | Google Scholor - Akwuruoha, E. M., Ezirim, E. O., Onyemereze, C. O., Abali, I. O., & Airaodion, A. I. (2025). Awareness and acceptance of hyoscine N-butylbromide in the management of labor among expectant mothers in Abia State University Teaching Hospital. International Journal of Studies in Midwifery and Women’s Health, 6(3):1–9.
Publisher | Google Scholor - Akwuruoha, E. M., Ezirim, E. O., Amah, C. I., Onyemereze, C. O., & Airaodion, A. I. (2025). Prevalence and awareness of premature ovarian insufficiency among Nigerian women. Journal of Women Health Care and Gynecology, 5(5):1–8.
Publisher | Google Scholor - Adewale, F. B., Adekanye, A. O., Erinle, S. A., Nwosu, I. C., & Nwosu, A. E. (2025). Awareness and use of emergency contraception among women attending antenatal clinic in a tertiary hospital in Nigeria. Journal of the Turkish German Gynecological Association, 26(4):246–255.
Publisher | Google Scholor - Kwame, K. A., Bain, L. E., Manu, E., & Tarkang, E. E. (2022). Use and awareness of emergency contraceptives among women of reproductive age in sub-Saharan Africa: A scoping review. Contraception and Reproductive Medicine, 7(1):1.
Publisher | Google Scholor - Lamina, M. A. (2015). Prevalence and Determinants of Unintended Pregnancy Among Women in South-Western Nigeria. Ghana Medical Journal, 49(3):187.
Publisher | Google Scholor - Ashimi, A. O., Riyad, M., Aminu, M. B., Michael, G. C., & Akande, T. S. (2024). Prevalence and determinants of unintended pregnancy among women attending antenatal clinics in a semi-rural community in Northern Nigeria. West African Journal of Obstetrics and Gynaecology, 1(1):11–14.
Publisher | Google Scholor - Renne, E. P. (1998). Postinor use among young women in Southwestern Nigeria: A research note. Reproductive Health Matters, 6(11):107-114.
Publisher | Google Scholor - Dada, O. A., Godfrey, E. M., Piaggio, G., & von Hertzen, H. (2010). A randomized, double-blind, noninferiority study to compare two regimens of levonorgestrel for emergency contraception in Nigeria. Contraception, 82(4):373–378.
Publisher | Google Scholor - Ikeme, A. C., Ezegwui, H. U., & Uzodimma, A. C. (2005). Knowledge, attitude and use of emergency contraception among female undergraduates in Eastern Nigeria. Journal of obstetrics and gynaecology: the journal of the Institute of Obstetrics and Gynaecology, 25(5):491–493.
Publisher | Google Scholor























