

Case Report
Use of Injectable Botulinum Toxin in Healing Postoperative: Case Report and Literature Review
- Raisa Lima Pinheiro Lopes *
Professor, IAAM/ASIME, Fortaleza, Ceara, Brazil.
*Corresponding Author: Raisa Lima Pinheiro Lopes, Professor, IAAM/ASIME, Fortaleza, Ceara, Brazil.
Citation: R.L.P. Lopes. (2025). Use of Injectable Botulinum Toxin in Healing Postoperative: Case Report and Literature Review, Clinical Case Reports and Studies, BioRes Scientia Publishers. 9(4):1-9. DOI: 10.59657/2837-2565.brs.25.230
Copyright: © 2025 Raisa Lima Pinheiro Lopes, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 28, 2025 | Accepted: February 11, 2025 | Published: February 18, 2025
Abstract
Scars are skin abnormalities resulting from trauma or incisions. When present in highly exposed areas, such as the face, they can cause social and psychological discomfort, resulting in a decrease in self-esteem. In surgical procedures, especially in surgeries with aesthetic objectives, efficient healing is essential for good results. In this context, botulinum toxin appears as an efficient adjuvant in attenuating the appearance of post-surgical scars. Due to its effect on reducing muscle tension around the scar and the modulation of some types of cells and cell signals, botulinum toxin presents an important improvement in the appearance of scars. In the present study, we present a case report describing the use of botulinum toxin in postoperative abdominoplasty scars in a patient with a strong tendency to form hypertrophic scars and keloids. Botulinum toxin proved to be an important adjuvant tool in the attenuation of scars, especially when associated with other therapeutic modalities and an adequate surgical technique.
Keywords: scars; skin abnormalities; trauma
Introduction
The wound healing process is one of the pillars of surgical therapy, however, hypertrophic scars or keloids can result in some situations. In the field of surgeries with aesthetic purpose and result, it is essential to obtain adequate healing with minimal apparent scars. In exposed areas such as the face, scars can result in social discomfort or self-esteem disorders in sufferers. Many studies have been proposed to find ways to prevent the formation of aesthetically unwanted scars in surgical procedures. In this context, botulinum toxin proved to be an excellent alternative in the treatment and prevention of post-surgical scars, hypertrophic scars or keloids. The present study aims to report a case in which botulinum toxin type A was used in the prevention of scars after cosmetic surgery and to discuss the subject based on the current literature. The literature search was carried out in the "PubMed" database in February 2023 using the descriptors: "botulinum toxin injection"; "botulinum toxin scar" "botulinum toxin postoperative". A total of 16 articles were included in the study, including systematic review articles with meta-analysis, randomized studies, and review articles, published in the last 17 years. Throughout this article we will address general concepts about botulinum toxin; definition of hypertrophic scars and keloids; the healing process and the use of this product in the prevention and treatment of scars, in addition to reporting the experience of a patient treated in our service with botulinum toxin to prevent post-surgical scars.
Case Report
Female patient, 41 years old, born and from Fortaleza, psychologist, Fitzpatrik II phototype, without excessive sun exposure, adept at routine use of photoprotection, with a significant previous history of hypertrophic scars and keloid formation. She underwent liposuction surgery with extended mini-abdominoplasty and resection of a previous cesarean scar in November 2022, with success. Still in the operating room, after the procedure, injections of botulinum toxin type A (Dysport 500UI) were performed with reconstitution diluted in 2 mL of sterile 0.9% saline solution and without preservatives to constitute a solution at a concentration of 5 IU/0.1 mL, applied at approximately 5 IU per 1.5cm of surgical wound, using 100 total units. Botulinum toxin type A was injected into the body of the surgical wound with the aid of a 24-gauge needle (0.3 mm × 0.8 mm) until a slight bleaching was visible. In the preoperative period, the Vancouver Scar Scale was applied, with a score of 11 for the previous cesarean scar. The patient was still being followed up postoperatively, with a report of satisfaction with the result still evolving, but already assigned a score of 3 on the Vancouver Scar Scale at the first return visit 7 days after the operation, with the following images. In addition to the surgical procedure combined with intraoperative application of botulinum toxin type A, the patient in question followed a strict and individualized protocol, prescribed by the surgical team: Dr. Raisa Lopes and Dr. Erik Nery, with a combination of technologies and procedures, including: fractional CO2 laser, biological dressings, compressive accessories, active ingredients for the treatment of post-inflammatory hyperpigmentation and physiotherapy, in addition to a specific surgical technique for the case.
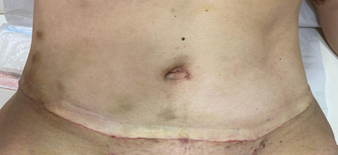
Figure 1
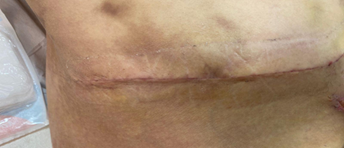
Figure 2
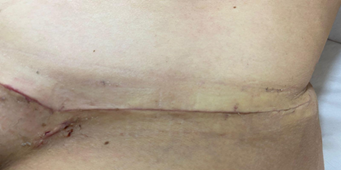
Figure 3
Images of the appearance of the surgical scar on the seventh postoperative day.
Background and General Concepts
In the late eighteenth and early nineteenth centuries, a series of fatal outbreaks took place in the ancient kingdom of Wurttemberg in present-day Germany. The cause of death was attributed to a toxin present in spoiled sausages. Botulus, means sausage in Latin. Around the same time, a young German physician suggested the supposed clinical utility of this toxin, however, the first documented therapeutic application of botulinum toxin occurred in 1977, when Dr. Alan Scott injected a purified botulinum toxin into extraocular muscles to treat strabismus. In 1989, botulinum toxin was licensed for use in the United States for the treatment of strabismus. Since then, there has been a wave of research on botulinum toxin, which has led to the addition of new formulations with an increasing range of indications. (CHOUDHURY, 2021).
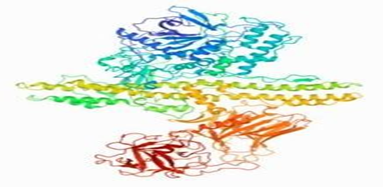
Figure 4: Crystalline structure of botulinum toxin type A.
The schematic representation shows that botulinum toxin type A has two peptide chains connected by a disulfide bridge. The heavy chain has two domains named according to their specific activity (linkage and translocation). The light chain is responsible for the catalytic breakdown of the target protein (CHOUDHURY, 2021).
Botulinum toxin is produced by Clostridium botulinum and consists of a neurotoxin composed of a heavy chain and a light chain joined by a single disulfide bond. It is synthesized as a relatively inactive single-stranded polypeptide with a molecular mass of approximately 150 kD. It is activated when the polypeptide chain is proteolytically cleaved into the 100 kD heavy chain and the 50 kD light chain. Botulinum neurotoxin exists in seven different serotypes (A, B, C, D, E, F, and G). Serotype A has been the most widely studied and used for therapeutic purposes. Its mechanism of action is based on the antagonism of cholinergic receptors. When botulinum toxin is injected into a target tissue, the botulinum neurotoxin heavy chain binds to structures such as glycoproteins found specifically in cholinergic nerve terminals (DRESSLER, 2005).
Its mechanism acts in the same way both in disease and in therapeutic applications. Botulinum toxin works by blocking the anchoring and function of soluble proteins N-ethylmaleimide receptor binding receptor (SNARE)-sensitive at the neuromuscular junction. SNARE proteins targeted by different subtypes of botulinum toxin (Type A and Type E) that cleave the synapsomal-associated protein (SNAP-25). Toxin types B, D, E, and G cleave synaptorevin-associated membrane protein or vesicle. Type C cleaves exclusively SNAP-25 and syntaxin. Joined by a disulfide bridge, the botulinum toxin heavy chain acts as the binding and translocation domain, while the toxin light chain acts as the catalytic domain. Botulinum toxin is very effective in blocking neuromuscular junctions when the target muscle is active, thus producing an autofocus effect. (ROSALES, 2006). Essentially, botulinum toxin blocks the release of acetylcholine from the motor terminals, and so skeletal muscles are unable to contract, although the action potentials continue to reach the motor plate. The duration of paralysis depends on the half-life of the light chain and the turnover time of SNARE proteins (CHOUDHURY, 2021).
Many treatments have been tried, with limited success, to reduce symptoms associated with abnormal scarring, such as redness, pain, itching, or functional limitations, and to improve clinical appearance. These treatments range from minimally invasive interventions (e.g., massages, moisturizing agents, pressure garments, and silicone covering) to topical or intralesional corticosteroids, surgical excision, or radiation therapy. In this context, botulinum toxin type A has been found to minimize scarring by reducing muscle tension in wound healing. In addition to altering the production of transforming growth factor (TGF-BETA 1) acting on fibroblasts. (SABRY, 2020).
Hypertrophic scars and keloids are fibroproliferative disorders in the reticular dermis layer: this layer has continuous inflammation, angiogenesis and abundant accumulation of collagen. Compared to classic hypertrophic scars, classic keloids spread aggressively, rarely resolve spontaneously, and at the histological level contain keloidal collagen, whereas hypertrophic scars have only nodules. However, many scars have the clinical and pathological characteristics of classic keloids and hypertrophic scars. This suggests that the classic hypertrophic scars and keloids are polar manifestations of the same skin disease, among which there is a spectrum of intermediate scars. The clinical and histological differences between classic hypertrophic scars and keloids probably reflect differences in the intensity and duration of inflammation of the reticular dermis. These differences, in turn, may reflect the presence and severity of local, systemic, genetic, and lifestyle risk factors.
Healing Process
The healing process is common to all wounds, regardless of the agent that caused it, it is systemic and dynamic and is directly related to the general conditions of the body. Wound healing consists of a perfect and coordinated cascade of cellular, molecular, and biochemical events that interact for tissue reconstitution to occur, and these mechanisms were described by Carrel in 1910, and later divided into five main elements: inflammation, cell proliferation, granulation tissue formation, contraction, and wound remodeling. Recently, Clark classified this process into three phases divided, didactically, into: inflammatory phase, proliferation or granulation phase, and remodeling or maturation phase.
Inflammatory Phase
This phase begins immediately after the injury, with the release of vasoconstrictor substances, mainly thromboxan A2 and prostaglandins, through cell membranes. The injured endothelium and platelets stimulate the coagulation cascade. Platelets play a fundamental role in healing. Aiming at hemostasis, this cascade is initiated and granules are released from platelets, the which contain growth factors, mainly TGF-β, which attract neutrophils to the wound. The clot is formed by collagen, platelets, and thrombin, which serve as a protein reservoir for the synthesis of cytokines and growth factors, increasing their effects. Thus, the inflammatory response begins with vasodilation and increased vascular permeability, promoting chemotaxis, that is, migration of neutrophils to the wound, which are the first cells to reach the wound, with a higher concentration 24 hours after the injury. Neutrophils produce free radicals that aid in bacterial destruction and are gradually replaced by macrophages, which migrate to the wound after 48 - 96 hours of injury, and are the main cells before fibroblasts migrate and begin replication. Macrophages act mainly in the transition to the proliferative phase: in the secretion of cytokines and growth factors, in addition to contributing to angiogenesis, fibroplasia, and extracellular matrix synthesis (BROUGHTON, 2006 and NAST, 2023).
Proliferative Phase
The proliferative phase consists of four fundamental stages: epithelialization, angiogenesis, granulation tissue formation, and collagen deposition. This phase begins around the 4th day after the injury and extends approximately until the end of the second week. Epithelialization occurs early. Angiogenesis is stimulated by tumor necrosis factor alpha (TNF-α), and is characterized by endothelial cell migration and capillary formation, which is essential for proper healing. The final part of the proliferative phase is the formation of granulation tissue. Fibroblasts and endothelial cells are the main cells of the proliferative phase, in addition to TGF-β, which stimulates fibroblasts to produce type I collagen and transform into myofibroblasts, which promote wound contraction (BROUGHTON, 2006 and NAST, 2023).
Maturation or Remodeling Phase
The most important feature of this phase is the deposition of collagen in an organized manner, which is why it is the most important clinically. The collagen initially produced is thinner than the collagen presents in normal skin, and has an orientation parallel to the skin. Over time, the initial collagen (type III collagen) is reabsorbed, and thicker collagen is produced and organized over the years. voltage lines. These changes are reflected in increased wound tensile strength. The reorganization of the new matrix is an important healing process. (BROUGHTON, 2006 and NAST, 2023).
Scar Formation
Scars form after the body is traumatized and then the skin protects the wound through nascent fibrin, resulting in wound healing by resolution rather than regeneration. In the healing process, granulation tissue and extracellular matrix are produced under regulation in a certain order as explained earlier. However, under the influence of external factors, this order can be broken, negatively affecting the balance between the production and degradation of these substances, this leads to the production of hypertrophic scars and possibly keloids. Insufficient reduction of incision tension and poor nutritional status are external factors that mainly alter this balance. In addition, tissue microtrauma caused by repeated activity or displacement of damaged tissue intensifies the inflammatory response and cellular metabolic activity in the incision area, resulting in increased extracellular collagen levels. (YUE, 2022) Several other factors contribute to an undesirable scar, including the patient's ethnic background, the anatomical location of the incision, the surgical techniques used, and postoperative infections. (KIM, 2019)
Wound healing is a complex process involving tissue regeneration, granulation tissue hyperplasia, and scar tissue formation, showing the synergistic effect of various processes. The scar growth process can be divided into the hyperplastic phase, stable phase, and atrophic phase. The key to preventing postoperative scar hyperplasia is the administration of treatment in the hyperplastic phase. The contractile force on both sides of the wound also plays a vital role in wound healing and scar growth. In general, scars are considered to be the result of abnormal, long-term healing, including excessive fibroblast production, accelerated angiogenesis, and excessive collagen accumulation. Pathological scars, such as hypertrophic scars and keloids, often occur in patients who they suffer burns, traumas and surgeries. It is important to note that the degree of injury and extent are directly proportional to the resulting scar. Although there are a wide variety of methods to prevent scarring, there is no standardized method to date. (ZHANG, 2020).
In addition to the concepts already employed, skin scars are generally differentiated from the surrounding normal skin by differences in color, thickness, contour, compliance, general cosmetics, and functional damage, such as contracture formation. Not only does disfigurement contribute to the undesirable appearance, but also to prolonged contracture, itching, or tingling that interferes with patients' daily lives.
Repeated cycles of microtrauma of the underlying muscles in skin wound healing are thought to play a role in prolonging the inflammatory phase and increasing collagen and glycosaminoglycan deposition in the wound, resulting in scar hypertrophy and hyperpigmentation. To reduce uncontrolled healing, several surgical concepts have been used, and although such techniques reduce tension, they do not eliminate it completely. The use of the temporary paralytic effect of botulinum toxin represents an interesting modality to reduce cycles of excessive microtrauma in the early stages of wound healing to improve overall scar quality. (AL-QATTAN, 2013).
Thus, botulinum toxin can theoretically reduce tension at the edges of the wound, helping to prevent more prominent scarring. (QIAO, 2021) Botulinum toxin type A can reduce muscle and skin tension during wound healing. This effect is called "chemomobilization" and helps to reduce the dynamic tension of wounds and improve the healing process. Botulinum toxin can also reduce inflammatory stimuli during wound healing, thereby reducing the negative impact of inflammatory stimuli on scar formation. (ZHANG, 2020).
Approach to The Prevention of Post-Surgical Scars
According to Nast A. et al, it is challenging to completely heal hypertrophic scars and keloids, as there is still no gold standard therapy available for these cases and most doctors rely on their clinical expertise when it comes to tailoring a therapeutic plan for a patient. It is essential to make a thorough assessment of the injury before treating it, this assessment should include the size and location of the injury, any associated pain or tenderness, and should also identify the expected results of the patient's treatment. A multidisciplinary therapeutic approach is preferred for some cases. Special care must be taken during and after surgery to prevent scarring. First, it is necessary to evaluate which patients are at higher risk for the formation of hypertrophic scars or keloids. Patients with a previous history of hypertrophic scarring and keloids are at high risk. Other risk factors include the site of the surgical wound. Locations often elongated by daily body movement, including the joints, anterior chest, scapula, and lower abdomen. On the other hand, hypertrophic scars and keloids rarely occur on the scalp and front of the leg, where the stretching stress is low. This is because the elongation of a wound prolongs and worsens its inflammation, causing hypertrophic scars or keloids. In addition, systemic factors include the female hormone estrogen and systemic arterial hypertension as risk factors, as well as classic keloids are strongly driven by genetics. This partly explains ethnic differences in susceptibility to keloids, which are more common in Africans (5 to 10 percent are affected), less common in Asians (0.1 to 1 percent), and rare in Europeans/North Americans (<0>
Specific Surgical Techniques and Apparatus
To prevent the formation of hypertrophic scars and keloids after surgery in susceptible body regions, surgical techniques that limit dermal tension should be used, such as: modern flaps; Z-plasties, W-plasties; subcutaneous sutures and deep fascial tension reduction; and barbed surgical threads, further releasing tension on the edges of the surgical wound. In addition, post-surgical wound elongation should be limited by fixation materials such as biological dressings, paper tape, gel sheets, gels, or bandages compression and clothing. All patients undergoing surgery on susceptible body areas should be closely monitored for hypertrophic scarring for 3 to 12 months (OGAWA, 2022).
Although surgeons make every effort to prevent the enlargement, hypertrophy, hypo or hyperpigmentation of scars, in some specific situations, such as extensive massive trauma or burns, especially in contexts where there is a risk to life, the aesthetic purpose is left in the background.
Scarring increases when opposing forces that tend to separate suture lines are applied to the newly formed collagen before it reaches final maturity, a process that can take several months before completion. Tension exacerbates inflammation and leads to increased collagen synthesis and glycosaminoglycan deposition, while prolonging erythema. Increased local metabolic activity can intensify hypertrophic scarring. (LEE, 2018) Thus, another important factor in good healing is the direction in which the incision is made in the body. When the wound direction is perpendicular to the underlying muscle, muscle contraction produces tension at the incision edge, which increases the risk of an enlarged scar and hypertrophic scar formation. (YUE, 2022) This concept refers to the tension lines of the relaxed skin, which are perpendicular to the tension vector of muscle contraction: scars aligned with the tension lines are subject to reduced tension and heal well, while scars oriented against the tension lines are subject to repeated tension and result in scar hypertrophy (LEE, 2018).
Botulinum Toxin And its Mechanisms
The mechanism of botulinum toxin in the treatment of scars has not been fully understood. Botulinum toxin is now most widely recognized for its tension-reducing effects. (PAN, 2022) Some studies have analyzed the possible mechanisms involving botulinum toxin in preventing scar formation: 1) Botulinum toxin can inhibit fibroblast proliferation, promote their apoptosis, and inhibit their differentiation into myofibroblasts; 2) Botulinum toxin. It can inhibit the expression and secretion of fibrosis-related factors. 3) At the same time, botulinum toxin can alter collagen deposition and induce collagen remodeling to a certain extent, reducing tension. To be specific, botulinum toxin type A may function as a downstream regulator of TGF-BETA 1 secreted by macrophages, which may reduce the expression of connective tissue growth factor. And botulinum toxin type A acts via TGF-BETA 1/SMAD at the molecular level, thus inhibiting scars formed by fibroblasts. (CHEN, 2021) Therefore, early postoperative injection of botulinum toxin increases the inhibition of scar hyperplasia and improves scar appearance (YUE, 2022).
Commercially, botulinum toxin type A is available in a range of products on the market, depending on your laboratories. In the present case report, we used the Dysport toxin from the Galderma laboratory, with excellent results described all over the world. Botulinum toxin can also be used in combination with triamcinolone acetonide, 5-Fluorouracil and laser therapies, achieving good results and serious side effects, such as skin atrophy and telangiectasias, are rare. (PAN, 2022)
A randomized study published in 2020, compared the efficacy and safety of intralesional versus topical botulinum toxin type A combined with fractional CO2 laser in the treatment of keloid hypertrophic scars, with a total of 20 patients evaluated. For hypertrophic scars, there was a significant improvement in all scar characteristics after completion of treatment with both methods, however, the score on the Vancouver scale was significantly higher after fractional CO2 laser combined with topical botulinum toxin A than after intralesional botulinum toxin A. For keloids, there was improvement in all scar characteristics in both treatment groups, except for pigmentation in the injection group and except for pigmentation and vascularization in the laser group. The percentage of improvement in vascularity and malleability was significantly higher in the group that used intralesional toxin. Regarding adverse effects, most patients reported minimal symptoms such as pain and pruritus, which did not differ significantly before and after treatment (SABRY, 2020).
There are several standardized ways used in studies to evaluate the effectiveness of the methods used in reducing scars. In this study, we applied the Vancouver Scar Scale (fig), which evaluates: The four components of melanin pigmentation (0-3 points), scar height (0-3 points), vascularization (0-3 points) and malleability (0-5 points), with a maximum score of 14 points that indicates the most severe scar formation.

Figure 5
Li et al, published in 2022, a systematic review with meta-analysis of randomized studies that investigated the efficacy of botulinum toxin type A injections in scars. Assessment methods included the Vancouver Scar Scale, Stony Brook Scar Rating Scale, Visual Analog Scale for Appearance Assessment, Visual Analog Scale for Scar Pain Assessment, and Scar Width were extracted for subgroup analysis. Twenty-one randomised controlled trials were included. The group of patients treated with botulinum toxin had scars with significantly smaller width than the group control, however, had a lower score on the pain scale than the group treated with steroids. On the Vancouver scale, the group treated with botulinum toxin obtained a higher score than the group submitted to steroids. In general, the group that used botulinum toxin showed more efficacy than the group that used saline solution, although steroids may have greater potency. Therefore, it may be considered as an alternative in patients not amenable to steroid treatment. (LI, 2022)
The toxin has a reversible paralytic effect that usually peaks around 1 to 2 weeks after injection. Neuronal activity begins to return about 3 months after injection. Factors affecting recovery include neuronal budding and molecular turnover within the neuromuscular junction. Permanent effects may occur in the injected muscle after repetitive treatment, but these effects are minor and do not significantly affect overall muscle function. (AL-QATTAN, 2013)
Gassner et al. conducted a blinded, prospective, randomized clinical trial to evaluate the use of botulinum toxin to improve the healing of facial lacerations. For evaluation, the visual analog scale was used in thirty-one patients with traumatic forehead lacerations or those who underwent elective excisions of forehead masses. The overall median visual analog scale score for the botulinum toxin-treated group was 8.9 compared to 7.2 for the placebo group, indicating improved healing. (GASSNER, 2006)
In 2019, Kim et al. conducted a randomized double-blind clinical trial to evaluate the efficacy of botulinum toxin type A injection in reducing scarring in patients with frontal laceration. Forty-five patients with forehead laceration were included in this study and randomized into 2 groups with or without botulinum toxin type A injection. When patients presented to the clinic to have the stitches removed, botulinum toxin type A was injected in 24 patients and saline solution was injected in 21 patients in the control group. The toxin was injected into the dermal layer with 5 IU/cm. After that, follow-up was done at 1,3 and 6 months. Scars were analyzed with the Patient and Observer Scar Rating Scale, Stony Brook Scar Rating Scales (SBSESs) and visual analogue scale (VAS) and analyzed with independent T-test, together with clinical photographs, cutometer and biopsy. In all scar scales, the highest scores were for the group that used botulinum toxin, showing statistical significance. The biopsy showed less collagen deposition in the dermal layer in the toxin group. Thus, botulinum toxin can be used with good results to prevent hypertrophic scars after trauma, burns or operations. (KIM, 2019)
In 2022, Han published a study with 49 patients comparing the isolated application of botulinum toxin A versus the application of the toxin combined with "W-plasty". W-plasty, or W-plasty, is a surgical technique performed by surgeons trained in plastic surgery that consists of excision of the old scar with wound closure by reapproximating the small interdigitated edges created, producing a zigzag pattern. The study showed superior results for the combination of botulinum toxin type A with W-plasty compared to the use of the toxin alone. Thus, it is expected to be a useful method to improve scars. (HAN, 2022)
Side Effects and Contraindications
One of the most common side effects of botulinum toxin is the diffusion of the toxin from the treated muscle to other neighboring muscle groups with unwanted paralytic effects. Other minor complications include pain, edema, erythema, ecchymosis, and hyperesthesia. The use of botulinum toxin is contraindicated in patient populations with known neuromuscular disorders such as myasthenia gravis, Lambert-Eaton syndrome, and multiple sclerosis. In these conditions, the toxin can aggravate muscle weakness. In addition, patients with a history of allergic process to the components, pregnant or breastfeeding women, as well as the concomitant use of aminoglycosides, calcium channel blockers, cyclosporine, and cholinesterase inhibitors should be avoided, as these drugs can potentiate the paralytic effect of the toxin (AL-QATTAN, 2013).
References
- Al-Qattan, M. M., Al-Shanawani, B. N., & Alhomer, F. (2013). Botulinum toxin type A: Implications in wound healing, facial cutaneous scarring, and cleft lip repair. Annals of Saudi Medicine, 5:482-488.
Publisher | Google Scholor - Broughton, G., Janis, J. E., & Attinger, C. E. (2006). The basic science of wound healing. Europe PMC, 117:12S–34S.
Publisher | Google Scholor - Chen, Z., Chen, Z., Pang, R., Wei, Z., Zhang, H., Liu, W., & Li, G. (2021). The effect of botulinum toxin injection dose on the appearance of surgical scar. Scientific Reports.
Publisher | Google Scholor - Choudhury, S., Baker, M. R., & Chatterjee, S. (2021). Botulinum toxin: An update on pharmacology and newer products in development. Toxins.
Publisher | Google Scholor - Dressler, D., Saberi, F. A., & Barbosa, E. R. (2005). Botulinum toxin: Mechanisms of action. Arquivos de Neuro-Psiquiatria.
Publisher | Google Scholor - Gassner, H. G., Brissett, A. E., Otley, C. C., Boahene, D. K., Boggust, A. J., Weaver, A. L., & Sherris, D. A. (2006). Botulinum toxin to improve facial wound healing: A prospective, blinded, placebo-controlled study. Mayo Clinic Proceedings.
Publisher | Google Scholor - Han, C.-H. (2022). Combination of W-plasty and botulinum neurotoxin type A injection for preventing rhytidectomy scar in Asians. Aesthetic Plastic Surgery.
Publisher | Google Scholor - Kim, S. H., Lee, S. J., Lee, J. W., Jeong, H. S., & Suh, I. S. (2019). Clinical trial to evaluate the efficacy of botulinum toxin type A injection for reducing scars in patients with forehead laceration: A double-blinded, randomized controlled study. Medicine (Baltimore), 98.
Publisher | Google Scholor - Lee, S. H., Min, H. J., Kim, Y. W., & Cheon, Y. W. (2017). The efficacy and safety of early postoperative botulinum toxin A injection for facial scars. Aesthetic Plastic Surgery, 42:530-537.
Publisher | Google Scholor - Li, M.-Y., Chiu, W.-K., Wang, H.-J., Chen, I. F., Chen, J.-H., Chang, T.-P., Ko, Y., & Chen, C. (2022). Effectiveness of botulinum toxin type A injection on scars: A systematic review and meta-analysis of randomized controlled trials. Plastic and Reconstructive Surgery.
Publisher | Google Scholor - Nast, A., et al. (2012). German S2k guidelines for the therapy of pathological scars (hypertrophic scars and keloids). J Dtsch Dermatol Ges, 10:747-762.
Publisher | Google Scholor - Ogawa, R. (2021). The most current algorithms for the treatment and prevention of hypertrophic scars and keloids: A 2020 update of the algorithms published 10 years ago. Plastic and Reconstructive Surgery, 149(1):79-94.
Publisher | Google Scholor - Pan, L., Qin, H., Li, C., Yang, L., Li, M., Kong, J., Zhang, G., & Zhang, L. (2021). Safety and efficacy of botulinum toxin type A in preventing and treating scars in animal models: A systematic review and meta-analysis. International Wound Journal.
Publisher | Google Scholor - Rosales, R. L., Bigalke, H., & Dressler, D. (2008). Pharmacology of botulinum toxin: Differences between type A preparations. European Journal of Neurology, 13(1):2-10.
Publisher | Google Scholor - Qiao, Z., Yang, H., Jin, L., Li, S., & Wang, X. (2021). The efficacy and safety of botulinum toxin injections in preventing postoperative scars and improving scar quality: A systematic review and meta-analysis. Aesthetic Plastic Surgery, 45:2350-2362.
Publisher | Google Scholor - Zhang, W., Li, X., & Li, X. (2020). Efficacy and safety of botulinum toxin type A in preventing postoperative scars and improving the cosmetic appearance of scars: A systematic review and meta-analysis. Journal of Cutaneous Medicine and Surgery, 24(6).
Publisher | Google Scholor























