

Case Report
Unraveling A Rare Neurological Emergency: Spontaneous Spinal Epidural Hematoma Leading to Paralysis-A Case Report and Literature Review
1 House Officer, PNS Shifa Hospital Karachi, Pakistan.
2 House Officer, Agha Khan University Hospital, Karachi, Pakistan.
3 Consultant Neurosurgeon, PNS Shifa Hospital Karachi, Pakistan.
4 M.D., Internal Medicine Department, Mirwais Regional Hospital, Pakistan.
5 House Officer, PNS Shifa Hospital Karachi, Pakistan.
*Corresponding Author: Kamil Ahmad Kamil,M.D., Internal Medicine Department, Mirwais Regional Hospital, Pakistan.
Citation: Kamil A Kamil, Anwar S, Hassan A, Ishfaq A, Aseef U Chaudhary, (2026). Unraveling A Rare Neurological Emergency: Spontaneous Spinal Epidural Hematoma Leading to Paralysis - A Case Report and Literature Review. International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 6(1):1-5. DOI: 10.59657/2837-8172.brs.26.085
Copyright: © 2026 Kamil Ahmad Kamil this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 06, 2026 | Accepted: January 20, 2026 | Published: February 06, 2026
Abstract
Spontaneous spinal epidural hematoma (SSEH) is an uncommon but potentially debilitating spinal cord compression disorder. As the name implies, it is an atraumatic neurological emergency characterized by the accumulation of blood within the spinal epidural space. It presents with symptoms associated with acute neurological deficits. Its etiology remains controversial, yet it is hypothesized to be mostly related to vascular pathologies. Other risk factors include anticoagulation therapy, coagulopathies, hypertension, cavernous angioma, and Paget's disease. MRI is considered the investigation modality of choice; urgent decompressive laminectomy with evacuation of hematoma is the definitive surgical intervention for prompt recovery.
Case presentation: We present a case of a 56-year-old male who presented with a sudden onset of pain followed by symptoms suggestive of acute neurological compromise. MRI revealed a cervical spine extradural hematoma at the C4-C6 level compressing the thecal sac and spinal cord. The patient was planned for urgent decompressive laminectomy and evacuation of hematoma.
Conclusion: Early assessment, prompt investigation, and timely surgical intervention are crucial in limiting the severity of SSEH and ensuring quick recovery.
Keywords: decompressive laminectomy; neurological deficits; spinal cord compression; spontaneous spinal epidural hematoma
Introduction
Spontaneous spinal epidural hematoma (SSEH) is a rare yet severe clinical condition characterized by the rapid accumulation of blood within the epidural space that leads to spinal cord compression [1]. Although its etiology remains unclear, it has been reported that SSEH is associated with some vascular abnormalities, anticoagulation therapy, and hypertension in some cases, while a large percentage of cases remain idiopathic [2]. Other reported causes of SSEH include cavernous angioma and Paget's disease[3][4]. This accumulation of blood results in the acute onset of pain and impairments in the sensory and motor systems of the body [5]. Magnetic resonance imaging (MRI) is considered the gold standard investigation for early detection and prompt treatment of this condition[6]. Treatment typically involves urgent decompressive laminectomy followed by evacuation of hematoma, particularly in patients presenting with severe neurological deficits [7] Conservative management is also considered in cases presenting with mild or non-progressive symptoms [2]. However, it carries the risk of deterioration of the symptoms as the hematoma can enlarge over time. Surgical intervention is the treatment of choice, especially in patients with significantly enlarged hematoma or severe onset of neurological deficiencies.
In this case report we present a similar case of SSEH who presented with severe neurological deficits and was surgically managed on an emergency basis.
Case Presentation
A 56-year-old married male, office worker from Karachi presented to the emergency department of PNS Shifa Hospital with primary complaints of neck pain associated with weakness and numbness in the right upper and lower limbs for the past three days. The neck pain was sudden in onset and was radiating to both shoulders. There was no episode of loss of consciousness or urinary incontinence. Initially, he took over-the-counter medications, but his symptoms worsened significantly, and over time his grip strength and sensation in both hands progressively weakened. He denied any accompanying symptoms including headache, fever, nausea, and vomiting. There was no history of hypertension or the use of any anticoagulants. His past medical and surgical history was unremarkable.
On examination, the patient was alert, oriented, and appeared lean with a blood pressure of 128/77 mmHg, pulse rate of 88 beats per minute, respiratory rate of 17 breaths per minute, and was afebrile. Neurological examination revealed strength graded 0/5 per the Medical Research Council (MRC) scale in bilateral lower limbs and right upper limb, while strength in the left upper limb was 3/5. Upon sensory examination, there was marked numbness along the anterolateral aspect of the right arm and right thigh down to the knee. There was hyperreflexia in both knee jerk and extensor planter response. There was no clonus. There was no evidence of trauma or deformity in the spine. The perianal sensation was intact, though the cremasteric reflex was diminished. Other systemic examinations including respiratory, cardiac, and abdomen was unremarkable. His baseline laboratory investigations were within normal ranges.
An MRI of the cervical spine with contrast revealed cervical spine extradural compression extending from the C4-C6 level, a hypointense signal on the T1-weighted image, a hyperintense signal on T2-weighted imaging, and no contrast enhancement. There was significant compression of the thecal sac and spinal cord on the right side, extending along the exiting nerve root into the neural foramina evident at the C6 level, as shown in Figure 1.
Given the severe spinal cord compression associated with impaired sensory and motor functions, the patient was planned for emergency C4-C6 laminectomy along with evacuation of the hematoma. A well-circumscribed hematoma was identified in the epidural space compressing the thecal sac and spinal cord. The hematoma was evacuated relieving the pressure on the spinal cord. There was no other pathology identified intraoperatively. After the surgery, the patient was shifted to the surgical ICU for observation. The patient was hypotensive for which he was given ionotropic support.
A postoperative MRI performed two days later showed the removal of the posterior elements of C4-C6 with the resolution of extradural hematoma compression. However, as shown in Figure 2, there was a persistent T2 hyperintense signal in the spinal cord. The patient's hypotension was stabilized, and he was transferred back to the surgical ward for ongoing management.
The patient showed partial improvement and after one week of hospital stay, he was discharged with recommendations for outpatient follow-up in one month. He was referred to his nearby hospital for physiotherapy and further monitoring. Upon discharge, his pain was significantly better, but his strength was partially recovered with a power of 3/5 in all limbs.
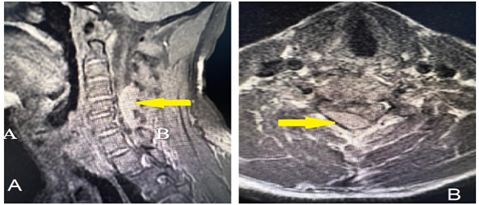
Figure 1: Preoperative MRI of cervical spine T2-weighted image with a hypertense signal in sagittal (A) and axial (B) cuts showing an extradural compression extending from the C4-C6 level as indicated by the yellow arrow.
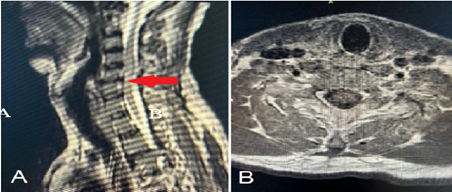
Figure 2: Postoperative sagittal (A) and axial (B) MRI images showing resolution of extradural hematoma compression with some residual edema at the C4-C6 level and a persistent T2-hyperintense signal in the spinal cord as indicated by the red arrow.
Timeline
The patient presented to PNS Shifa Hospital on 17-8-24 with complaints of cervicalgia and paraparesis. Contrast-enhanced MRI was performed the following day and C4-C6 decompressive laminectomy with the evacuation of the hematoma was done on 21-8-24. Two days later post-op CEMRI was done, and the patient was discharged after 1 week.
Discussion
Spontaneous spinal epidural hematoma (SSEH) is a rare clinical condition with a reported incidence of 0.1 per 100,000 patients annually[8]. SSEH typically affects adults in the age group between 40 to 60 years and often presents as severe pain with rapidly progressive neurological deterioration, overall presenting as an acute spinal cord compression syndrome[9]. The bimodal age distribution of SSEH shows peaks in the second and seventh decades of life. In our case, the patient presented with neck pain followed by progressive sensory and motor deficits, a presentation consistent with previously reported cases [10]. The spinal location of SSEH shows a bimodal distribution as well, with peaks at C6 and T12 levels[11].
The exact etiology of SSEH remains unclear, though some cases are associated with the use of anticoagulants, some coagulopathic conditions, and vascular anomalies [12]. In some cases, few authors have described the association of cavernous hemangioma and Paget’s disease with this disease[3][4]. However, in our patient, there was no identifiable cause which corresponds to the fact that 40-50% of cases are idiopathic[3]. In such cases where there is no history of trauma or use of anticoagulants, it is hypothesized that the origin of hematoma can be due to some rupture in vessels [13]. The origin of hematoma can be either arterial or venous[14], but it is mostly attributed to a venous cause because the venous plexus in the cervical and thoracic regions lacks valves[3]. Increased venous pressure in these areas can potentially rupture the corresponding vessels leading to bleeding and the formation of hematoma[13]. Increased venous pressure can be due to straining, coughing, sneezing, and constipation[3]. This may explain the occurrence of SSEH in otherwise healthy individuals, although further research is warranted to clarify the exact etiology.
Prompt diagnosis of SSEH is critical to execute early surgical intervention thus limiting the potential neurological complications[2]. Particularly in severe motor deficits, timely intervention is crucial for better neurological outcomes and uneventful recovery. MRI is recognized as the diagnostic modality of choice, as it accurately identifies the site and extent of hematoma[8]. In our patient, T2-weighted hyperintensity identified the presence of hematoma with significant spinal cord compression, supporting the urgency of surgical intervention. As seen in our patient with compression extending from C4 to C6, rapid MRI assessment and urgent laminectomy are considered crucial for the management of cases with severe neurological involvement [5].
The standard treatment for SSEH is urgent decompressive laminectomy and hematoma evacuation, especially in patients presenting with severe and progressive symptoms[7]. It has been reported that timely surgical intervention is associated with favorable outcomes and significant recovery[15]. However, cases with minimal symptoms can be managed conservatively but carry risks of permanent neurological impairment as the hematoma can enlarge over time[16]. Since our patient had hematoma associated with a rapidly progressive onset of symptoms and significant clinical deterioration, conservative management was not followed.
Many surgical cases report only partial recovery[7]. The likelihood of poor outcome of surgery depends upon the prognostic factors including the thoracic location, large size of the hematoma, poor neurological status of the patient at presentation, delayed surgery beyond 24 hours, and use of anticoagulants[1]. Our patient underwent C4-C6 decompressive laminectomy, and the hematoma was surgically evacuated relieving the pressure on the spinal cord. Even after the surgery, the patient had a post-operative hyperintense signal in the spinal cord with significant residual compression which is associated with the poor outcome. This highlights the importance of postoperative imaging in evaluating potential residual lesions or re-occurrence of hematoma.
In our case, the patient had poor prognostic factors including severe neurological symptoms on presentation, involvement of the cervical spine, large size of the hematoma, and delayed intervention due to presentation on the 3rd day of illness. Upon discharge, his pain had subsided with improvement in limb strength. Although the compression was relieved after surgery, there were persistent signal changes in the cord due to primary cord compression, resulting in compromised neurological recovery. This case emphasizes the role of post-operative care and monitoring as well as the importance of follow-up and rehabilitation plans. Based on the existing research, most of the reported cases of SSEH who underwent timely decompression and laminectomy showed quick recovery with complete neurological recovery [8].
Conclusion
Spontaneous spinal epidural hematoma (SSEH) should be considered in the differentials of compressive lesions, even when there is no history of trauma. This case underscores the critical importance of adequate assessment, early diagnosis, and timely surgical intervention in patients diagnosed with SSEH. It further demonstrates the need for postoperative monitoring and imaging to optimize neurological recovery and functional improvements.
Declarations
Conflict of Interest Disclosure
We declare that we have no conflicts of interest related to this case report.
Financial Interests
None
Funding Disclosure
No funding was received for this study or for any part of the work associated with this case report.
Institutional Affiliations
No institutional or organizational affiliations have an interest in the outcome of this study.
Patient Consent and Ethical Approval
Informed consent was obtained from the patient for the publication of this case report. Ethical approval was not required for this case report.
References
- Hsu CJ, Liao PZ, Jeng DT, et al., (2024). Prognostic factors and treatment efficacy in spontaneous spinal epidural hematoma: a single-center experience and literature review. Int J Anticancer Res. 38(5):2415-2424.
Publisher | Google Scholor - Dziedzic T, KPKPMA. (2015). Management and neurological outcome of spontaneous spinal epidural hematoma. J Clin Neurosci.22(4):726-729.
Publisher | Google Scholor - Gopalkrishnan CV, Dans S. (2012). Spontaneous cervical epidural hematoma of idiopathic etiology: case report and review of literature. J Spinal Cord Med.35(2):113-117.
Publisher | Google Scholor - Lee KS, JMMJNA. (1988). Spinal epidural hematoma associated with Paget’s disease. Surg Neurol. 30(2):131-134.
Publisher | Google Scholor - Bathini A, DSHMAMKMSZH. (2008). Spontaneous spinal epidural hematoma in the setting of uncontrolled hypertension and hypertensive emergency. Interdiscip Neurosurg.26:101292.
Publisher | Google Scholor - Baek BS, HJKKLH. (2008). Spontaneous spinal epidural hematoma. J Korean Neurosurg Soc. 44(1):40-42.
Publisher | Google Scholor - Shin JJ, KSCYSmossehESJ. (2008). Surgical management of spontaneous spinal epidural hematoma. Eur Spine J.15(6):998-1004.
Publisher | Google Scholor - Zhu DP, MYaTLaKYaYMaXHaGYaY. (2022). Prognostic factors and treatment efficacy in spontaneous spinal epidural hematoma. Neurology.99(8): e843-e850.
Publisher | Google Scholor - Ali SS, PNGP. (2021). A rare case of spontaneous spinal epidural hematoma in a 43-year-old man. J Am Coll Emerg Physicians Open.2(4): e12532.
Publisher | Google Scholor - Salehpour F, MFKMAS. (2019). Spontaneous epidural hematoma of cervical spine. Int J Spine Surg.12(1):26-29.
Publisher | Google Scholor - Kreppel D, AGSW. (2003). Spinal hematoma: a literature survey with meta-analysis of 613 patients. Neurosurg Rev.26(1):1-49.
Publisher | Google Scholor - Abu-Abaa M, JOMAAQG. (2023). A spontaneous spinal epidural hematoma secondary to long-term low-dose aspirin and clopidogrel use: a case report. Cureus.15(2): e34537.
Publisher | Google Scholor - Unnithan A. (2019). A brief review of literature of spontaneous spinal epidural hematoma in the context of an idiopathic spinal epidural hematoma. Egypt J Neurosurg.34:1-6.
Publisher | Google Scholor - Awada A, RNaFNNRaKH. (1988). Spontaneous cervical epidural hematoma: case report. Spinal Cord.36(1):71-72.
Publisher | Google Scholor - Raasck K, HA, AAea. (2017). Spontaneous spinal epidural hematoma management: a case series and literature review. Spinal Cord Ser Cases.3:16043.
Publisher | Google Scholor - Tamaki Y. (2024). Comparison of conservative and surgical treatments for spontaneous spinal extradural hematoma. J Spine Res.15(9):1202-1207.
Publisher | Google Scholor























