

Case Report
Unilateral Proptosis in a Child: An Unusual Case of Orbital Hydatidosis
- S. Moujrid *
- A. CHafo
- M. Loudghiri
- W. Bijou
- Y. Oukessou
- S. Rouadi
- R. Abada
- M. Roubal
- M. Mahtar
Department of Otolaryngology, Head and Neck Surgery, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
*Corresponding Author: S. Moujrid, Department of Otolaryngology, Head and Neck Surgery, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
Citation: Moujrid S, Chafo A, Loudghiri M, Bijou W, Oukessou Y, et al. (2025). Unilateral Proptosis in à Child: An Unusual Case of Orbital Hydatidosis. Journal of Clinical Medicine and Practice, BioRes Scientia Publishers. 2(1):1-4. DOI: 10.59657/3065-5668.brs.25.017
Copyright: © 2025 S.Moujrid, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 22, 2025 | Accepted: February 04, 2025 | Published: February 11, 2025
Abstract
Hydatidosis, also known as echinococcosis, is a zoonotic disease caused by the larval stage of Echinococcus granulosus, a parasite with a cosmopolitan distribution. Orbital involvement is exceedingly rare, with a reported incidence ranging from 0.3% to 1.0% among patients with echinococcosis. Due to its rarity, the condition is often underdiagnosed. The most common clinical manifestations include non-pulsatile, non-reducible proptosis, chemosis, eyelid edema, visual impairment, and restricted extraocular motility. Diagnostic imaging modalities such as ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) play a pivotal role in identifying orbital hydatidosis. CT typically reveals a well-defined, low-attenuation lesion, while MRI shows characteristic hypointensity on T1-weighted images and hyperintensity on T2-weighted images. Definitive diagnosis, however, relies on histopathological examination of the excised cyst. Surgical excision remains the treatment of choice for orbital hydatidosis. The primary surgical challenge is to avoid cyst rupture, which can result in dissemination of scolices and potentially life-threatening complications such as anaphylactic shock. Advances in surgical techniques and preoperative planning have improved outcomes. We report the case of a 5-year-old child with no significant medical history, who presented with progressive proptosis over three months. Clinical examination revealed grade III non-reducible, non-painful proptosis, accompanied by papillary edema. Fundoscopy demonstrated papillary hyperemia. CT imaging identified a well-defined, contrast-enhancing orbital mass measuring approximately 3 cm, without evidence of globe invasion. MRI confirmed the presence of a benign hydatid cyst, showing typical signal characteristics. The patient underwent successful complete surgical excision of the lesion without significant complications. This case highlights the importance of early diagnosis and meticulous surgical management in rare presentations of orbital hydatidosis.
Keywords: hydatidurias; orbital cyst; orbital hydatidurias; proptosis; chemosis
Introduction
Hydatidosis, or echinococcosis, is a zoonotic disease caused by the larval stage of Echinococcus granulosus, a cosmopolitan parasite with widespread global distribution. The Maghreb region represents an intermediate transmission zone, with Morocco—due to its traditional livestock farming practices—ranking among the countries most affected by this parasitic disease. While hepatic and pulmonary localizations are the most common, hydatidosis can involve virtually any organ. Orbital involvement, however, is exceedingly rare, with only a few cases reported in the literature. The incidence of orbital hydatid disease has been estimated at 0.3% to 1.0% among patients with echinococcosis [1-3]. The primary clinical manifestation of orbital hydatid cysts is exophthalmos. Imaging modalities, particularly computed tomography (CT) and magnetic resonance imaging (MRI), play a crucial role in preoperative diagnosis. Serology is generally insufficient for definitive diagnosis, and treatment remains exclusively surgical [4, 5].
Case Report
We report the case of a 5-year-old child with no notable medical history, presenting with progressive exophthalmos over three months. Clinical examination revealed grade III irreducible, non-painful exophthalmos associated with papilledema. Fundus examination demonstrated papillary hyperemia, and visual acuity was 10/10 in both eyes.
Orbital CT and MRI were performed
CT imaging revealed a well-defined mass, approximately 3 cm in size, enhanced by contrast, causing grade III exophthalmos without globe invasion or evidence of bone erosion. MRI showed a well-demarcated left intraorbital lesion, hypointense on T1-weighted images and hyperintense on T2-weighted images, suggestive of a benign hydatid cyst. The patient underwent surgical excision of the lesion. Histopathological analysis confirmed the diagnosis of a hydatid cyst. Postoperative clinical evolution of the left eye was marked by a gradual resolution of inflammatory signs and regression of the exophthalmos.

Figure 1: photos of the patient before (left) and after (right) the removal of the orbital cyst
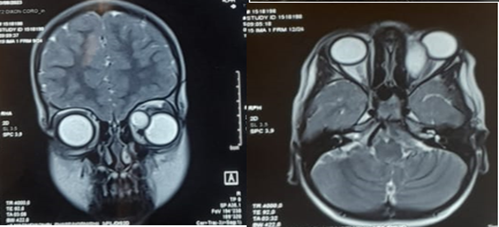
Figure 2: Axial and frontal section of T2 MRI showing the orbital cyst
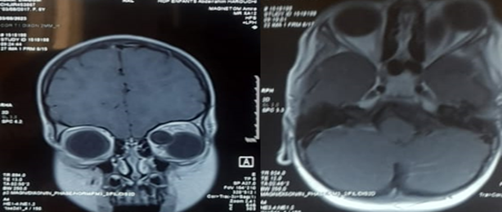
Figure 3: Axial and frontal section of T1 MRI showing the orbital cyst
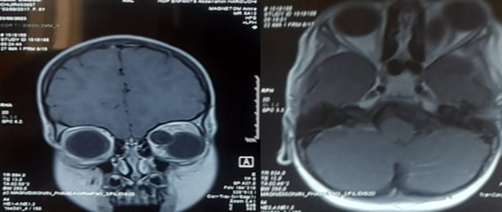
Figure 4: Axial and coronal section of facial CT scan showing the orbital cyst
Discussion
Hydatidosis is a zoonotic disease caused by the parasitic tapeworm Echinococcus, which can affect nearly all organs and tissues through both the portal and systemic circulations. The disease is endemic in regions with significant sheep and cattle farming, such as Australia, East Africa, South America, Eastern Europe, and the Middle East. Orbital hydatid cysts are exceedingly rare, accounting for only 0.3% to 2% of all hydatid disease cases. While these cysts can occur at any age, they are more frequently reported in children, reflecting the higher likelihood of exposure to endemic environments [3, 6]. The most common clinical manifestations of orbital hydatid cysts include irreducible, non-pulsatile exophthalmos, chemosis, eyelid edema, visual deterioration, and restricted extraocular motility. These non-specific symptoms make imaging an essential tool for accurate diagnosis. Orbital ultrasonography, CT, and MRI are the main diagnostic modalities. CT typically reveals a well-defined, cystic intraorbital lesion with regular margins, often causing bony remodeling or thinning, such as the characteristic "water lily" sign. MRI provides superior soft tissue contrast, with lesions appearing hypointense on T1-weighted images and hyperintense on T2-weighted images, often demonstrating peripheral ring enhancement. Fat suppression techniques on MRI are particularly useful in delineating the cyst capsule and assessing intraconal involvement.
Differential diagnosis for orbital hydatid cysts includes dermoid and epidermoid cysts, chronic hemorrhagic orbital cysts, orbital abscesses, congenital cysts, mucoceles, lymphangiomas, teratomas, and other orbital cystic lesions. A thorough radiological evaluation is crucial for narrowing the differential and planning appropriate surgical intervention [7-9]. Surgical excision is the cornerstone of treatment for orbital hydatidosis. Depending on the cyst's size and location, various surgical approaches may be employed, including fronto-orbital, lateral orbitotomy (Kronlein-Berke approach), transconjunctival, inferior orbitotomy, lateral rhinotomy, percutaneous, or transmaxillary routes [10-12]. The key surgical objective is to achieve complete cyst removal without rupture to prevent complications such as dissemination of scolices, implantation of secondary cysts, or anaphylactic shock. Histopathological evaluation following surgical excision confirms the diagnosis. Clinicians should maintain a high index of suspicion for orbital hydatidosis in patients presenting with exophthalmos, particularly in endemic regions. Due to the limited space within the orbital cavity, even slow-growing cysts can exert a mass effect, compromising the optic nerve and leading to irreversible visual loss. Early diagnosis and prompt surgical management are therefore critical to preserving visual function and preventing complications [6, 8]. Although rare, orbital hydatid cysts represent an important differential diagnosis in endemic areas. This case highlights the importance of integrating clinical, radiological, and surgical expertise in the management of such challenging cases.
Conclusion
Intraorbital localization of hydatid cysts is extremely rare, and the clinical presentation is often nonspecific. Radiological evaluation plays a pivotal role in diagnosis, with MRI and orbital CT providing detailed characterization of the lesion. The treatment is exclusively surgical, with careful attention to avoid cyst rupture. Early diagnosis and management significantly improve the prognosis, preventing visual field abnormalities and blindness. Orbital hydatid cysts should be considered in the differential diagnosis of unilateral proptosis, particularly in patients residing in endemic regions.
References
- B. E. Mansouri, M. Laboudi, A. Sadak, et M. Rhajaoui, L’hydatidose humaine dans la région de Rabat (Maroc): Etude de prévalence et apport du diagnostic sérologique.
Publisher | Google Scholor - BCHIR. (1988). Epidémiologie de l’hydatidose chez l’enfant et l’adolescent tunisiens, Epidémiologie Hydatidose Chez Enfant Adolesc. Tunis, 45(2):111-114.
Publisher | Google Scholor - Y. Jeblaoui, J. Bouguila, K. Yacoub, H. Bouguila, N. Ben Neji, et al. (2008). G. Besbes, Kyste hydatique de lobate, Rev. Stomatol. Chir. Maxillofac, 109(2):117-119.
Publisher | Google Scholor - Gomez Morales, J. O. Croxatto, L. Crovetto, et R. Ebner. (1988). Hydatid Cysts of the Orbit, Ophthalmology, 95(8):1027-1032.
Publisher | Google Scholor - Karan M, A. Yashant, H. Priya, et S. Pragati A. (2015). Isolated primary orbital hydatid disease presenting as multiple cystic lesions: a rare cause of proptosis, Ann. Parasitol, 193-195.
Publisher | Google Scholor - N. Albab. (2020). A Rare Case of Orbital Hydatid Cyst, Adv. Surg. Sci, 8(1):11.
Publisher | Google Scholor - F. Héran, Imagerie des masses orbitaires, Neurochirurgie, 56(2‑3):89‑120.
Publisher | Google Scholor - Debela, K. Abore, A. Worke, et S. Wendimagegn. (2024). Primary Intra-Orbital Hydatid Cyst: A Case Report of a Rare Cause of Exophthalmos, Int. Med. Case Rep, 17:89-92.
Publisher | Google Scholor - M. Kumar, V. Harsh, A. Prakash, C. B. Sahay, et A. Kumar. (2022). Neglected Case of Primary Intraorbital Hydatid Cyst, Neurol. India, 70(1):337-339.
Publisher | Google Scholor - M. Hammoud. (2020). Fronto orbital approach for primary orbital hydatid cyst: Case report, J. Neurol. Stroke, 10(1).
Publisher | Google Scholor - M. Abouassi, M. Aloulou, N. Hawa, T. Toutounji, et S. Alyousef. (2020). Successful eradication of a large orbital hydatid cyst without rupture using fronto-orbitozygomatic approach, the first case reported from Syria , J. Surg. Case Rep, 10:357.
Publisher | Google Scholor - K. Chtira, L. Benantar, H. Aitlhaj, H. Abdourafiq, Y. Elallouchi, et al. (2019). The surgery of intra-orbital hydatid cyst: a case report and literature review , Pan Afr. Med, 33.
Publisher | Google Scholor























