

Research Article
The Role of Ultrasonography in The Diagnosis, Mapping, And Follow-Up of Endometriosis
- Nayab Mustansar *
Resident Radiology, CMH Peshawar, Pakistan.
*Corresponding Author: Nayab Mustansar, Resident Radiology, CMH Peshawar, Pakistan.
Citation: Mustansar N. (2025). The Role of Ultrasonography in The Diagnosis, Mapping, And Follow-Up of Endometriosis, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 8(6):1-3. DOI: 10.59657/2837-4681.brs.25.207
Copyright: © 2025 Nayab Mustansar, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 13, 2025 | Accepted: September 27, 2025 | Published: October 04, 2025
Abstract
Endometriosis is a chronic gynecological condition marked by the presence of endometrial- like tissue outside the uterus, causing pain and infertility. Early diagnosis is essential for effective management. This study evaluates the diagnostic, mapping, and follow-up role of ultrasonography in 250 patients clinically suspected of having endometriosis. Transvaginal ultrasonography (TVUS) and transabdominal ultrasonography (TAUS) were utilized. Results show a high correlation between ultrasound findings and surgical/histopathological confirmation, supporting its non-invasive, cost-effective role in endometriosis care.
Keywords: ultrasonography; diagnosis; mapping; endometriosis
Introduction
Endometriosis affects approximately 10% of reproductive-aged women globally. Symptoms include dysmenorrhea, chronic pelvic pain, dyspareunia, and infertility. Despite its prevalence, diagnosis is often delayed due to nonspecific symptoms and invasive confirmation methods such as laparoscopy. Ultrasonography, especially transvaginal ultrasound (TVUS), is increasingly recognized for its potential to diagnose and map endometriotic lesions.
This study investigates the efficacy of ultrasonography in diagnosing and monitoring endometriosis, offering an evidence-based perspective on its clinical utility.
Materials and Methods
Study Design and Population
A prospective observational study was conducted at a tertiary care hospital over 24 months.
Sample Size: 250 womenaged 18–45 years
Inclusion Criteria: Patientspresenting with pelvic pain, infertility, or menstrual irregularities suggestive of endometriosis.
Exclusion Criteria: Pregnancy, prior hysterectomy, or ovarian malignancy.
Ultrasonography Protocol
Initial Imaging:All patients underwentTVUS; TAUS was added in cases whereTVUS was not feasible.
Lesion Mapping:
Ultrasound findingswere classified as ovarian endometriomas, deep infiltrating endometriosis (DIE), or superficial peritoneal lesions (limited detectability).
Confirmatory Tests:
Laparoscopy with histopathological confirmation was performed in 180 cases.The remaining 70 were managed conservatively or declined surgery.
Follow-up:
Patients were re-evaluated with ultrasonography after 6 monthsof medical or surgical treatment.
Results
Demographics and Symptoms Mean Age: 31.4 ± 5.8 years Presenting Complaints:
Chronic pelvic pain: 78% Dysmenorrhea: 70%
Dyspareunia: 40%
Infertility: 52%
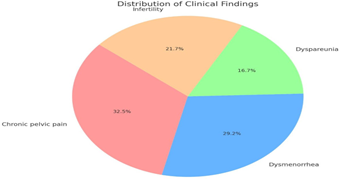
Figure: 1
Ultrasound Findings
Ovarian Endometriomas (unilocular cysts with ground-glass echogenicity): detected in 150/250 (60%).
Deep Infiltrating Endometriosis (DIE) (nodules in uterosacral ligaments, rectovaginal septum, bladder, or bowel): seen in 80/250 (32%).
Adhesions/Immobilized Ovaries: 30%.
Superficial Lesions: Not reliably visualized on US.
Diagnostic Accuracy (compared to laparoscopy): Sensitivity: 88%.
Specificity: 84%.
Positive Predictive Value (PPV): 91% Negative Predictive Value (NPV): 79% Overall accuracy: 86%.
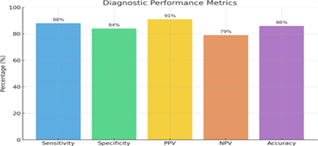
Figure: 2
Follow-up Findings (after 6 months)
Medical management (GnRH agonists or progestins): 65% showed lesion size reduction post-surgical cases: 80% had no recurrence or residual lesion on US.
Symptom correlation: 85% of those with improved US findings reported symptom relief.
Discussion
Ultrasonography, particularly TVUS, proved to be a valuable tool in the non-invasive diagnosis of endometriosis. The high sensitivity and specificity found in our study corroborate earlier research, Hudelist et al. (2011) showed TVUS has >85% sensitivity in detecting DIE, Guerriero et al. (2016) emphasized the role of expert sonographers in mapping rectosigmoid and bladder involvement.
Ovarian endometriomas are relatively easy to diagnose, whereas DIE requires a skilled operator familiar with pelvic anatomy and “sliding sign” techniques. The inability to reliably detect superficial peritoneal implants remains a limitation. However, ultrasonography offers real-time, repeatable, cost-effective imaging — especially valuable for post-treatment follow- up and mapping for surgical planning.
Our results reinforce the idea that ultrasonography, when performed by trained clinicians, can significantly reduce diagnostic delays and aid in comprehensive patient management.
Conclusion
Ultrasonography plays a crucial role in the diagnosis, mapping and follow-up of endometriosis. It provides a reliable, non-invasive method to assess and monitor disease progression, particularly in resource-limited settings. Integration into routine gynecologic evaluation can enhance early detection and tailored treatment strategies.
Recommendations
Training in advanced TVUS techniques should be integrated into gynecologic imaging programs.
Multidisciplinary approaches with sonographers, gynecologists, and radiologists improve mapping accuracy.
Future research should explore AI-assisted ultrasound interpretation for better detection of subtle lesions.
References
- Hudelist G, et al. (2011). Transvaginal sonography vs. clinical examination for preoperative diagnosis of deep infiltrating endometriosis. Ultrasound in Obstetrics & Gynaecology, 37(4):466–472.
Publisher | Google Scholor - Guerriero S, et al. (2016). Imaging techniques for the evaluation of deep endometriosis: a comparative study. Human Reproduction Update, 22(4):392–409.
Publisher | Google Scholor - Exacoustos C, et al. (2014). Ultrasound mapping system for the surgical management of deep infiltrating endometriosis. Fertility and Sterility, 102(1):143–150.
Publisher | Google Scholor - Bazot M, et al. (2012). Ultrasound assessment of uterine and pelvic endometriosis. Obstetrics and Gynecology Clinics, 38(4):703–726.
Publisher | Google Scholor - Van Holsbeke C, et al. (2010). Ultrasound diagnosis of endometriosis and the prediction of recurrence. BJOG, 117(10): 1207–1215.
Publisher | Google Scholor























