

Research Article
The Role of Multipurpose Community Health Workers in Zero-Dose Catch-Up: Experience from The Meningitis Vaccination Campaign in The North Region
- Bertin Jugnia *
- Gideon Ayoh
- Jeudi Debnet
Sub-Directorate of Vaccination, Ministry of Public Health, Yaounde, Cameroon.
*Corresponding Author: Bertin Jugnia, Sub-Directorate of Vaccination, Ministry of Public Health, Yaounde, Cameroon.
Citation: Jugnia B., Ayoh G., Debnet J. (2025). The Role of Multipurpose Community Health Workers in Zero-Dose Catch-Up: Experience from The Meningitis Vaccination Campaign in The North Region, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 3(6):1-5. DOI: 10.59657/2997-6103.brs.25.070
Copyright: © 2025 Bertin Jugnia, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 10, 2025 | Accepted: May 07, 2025 | Published: May 14, 2025
Abstract
Introduction: The large number of under-immunized and zero-dose children is a major challenge, so every opportunity that arises must be capitalized on. This study shares the experience of catch-up vaccination of these children by multipurpose community health workers (MCHWs) during a mass meningitis vaccination campaign in Cameroon.
Objective: The objective of this study is to highlight the roles of MCHWs in zero-dose catch-up during the meningitis vaccination campaign.
Methodology: We analysed and described the results obtained from a meningitis vaccination campaign conducted in two health districts from 12 to 16 June 2024.
Results: As part of the catch-up of zero-dose children, the MCHWs major role is to raise awareness about vaccination. These actors identified 1,527 zero-dose children and 289,139 people were reached. Finally, these community players took part in catch-up efforts to ensure that all these children were vaccinated. As a result, 565 children were vaccinated with PENTA-1 (37%).
Conclusion: Vaccination campaigns offer a considerable opportunity to catch up with zero-dose or under-immunized children. Micro-planning must always take into account the involvement of multipurpose community health workers in actively seeking out and possibly referring these children for vaccination.
Keywords: multipurpose community health workers; zero dose; PENTA-1; vaccination
Introduction
Vaccination is an essential component of primary healthcare. According to the World Health Organization (WHO), more than 20 potentially fatal diseases can now be prevented by vaccination [1]. The Immunization Agenda 2030 (IA2030) envisions ‘a world where every person, everywhere and at every age, benefits fully from vaccines for their health and well-being’ [2]. This programme is a global initiative led by the World Health Organization (WHO) and its partners, aimed at strengthening immunisation systems for the decade 2021-2030. Its main objective is to improve access to vaccines, strengthen immunisation and prevent vaccine-preventable diseases. More specifically, this will involve (i) improving equitable access to vaccines and ensuring that all populations, especially the most vulnerable, can benefit from immunisation; (ii) strengthening health systems and integrating immunisation services into health systems to ensure their sustainability; (iii) achieving ambitious immunisation coverage targets and reducing the gap between countries and increasing global immunisation coverage; (iv) promote innovation and research and encourage the development of new vaccines and improved delivery strategies; (v) prevent and respond to epidemics and strengthen capacity to detect and respond rapidly to outbreaks of preventable diseases; (vi) strengthen public confidence in immunisation and combat misinformation and raise community awareness of the importance of vaccines. As part of the coverage and equity objectives, this programme also emphasises the extension of immunisation services to regularly reach ‘zero-dose’ and under-vaccinated children and communities.
In 2023, the WHO estimates that 14.5 million children worldwide were not vaccinated - so-called ‘zero-dose’ children - indicating inadequate access to immunisation and other health services, and a further 6.5 million infants were only partially vaccinated [3]. According to UNICEF, strengthening primary healthcare systems is essential to treating and reaching zero-dose children. Training health workers and community health workers in digital technologies is essential to the success of these efforts [4].
In Cameroon, the Expanded Programme on Immunisation (EPI) manages to reach zero-dose children in unstable areas thanks to an approach based on the periodic intensification of routine immunisation with effective micro-planning and communication [5]. This intervention involves each health district team, usually a regional Expanded Programme on Immunisation manager and district medical officers, developing a microplan, recruiting Community Health Workers (CHWs) and health facility staff to go into communities to provide catch-up doses to children and adults, and liaising with community leaders who can advocate with families to participate in services [6].
According to the WHO, Community Health Workers (CHWs) can help to increase access to healthcare and improve its quality, particularly in the context of achieving universal health coverage between 2016 and 2030, the period of the Sustainable Development Goals (SDGs) [7]. In Cameroon, community involvement in the implementation of healthcare activities takes place through Multipurpose Community Health Workers (MCHWs), Dialogue Structures, Community-based Organisations (CBOs) and Decentralised Territorial Collectivities (DTCs) [8]. In recent years, however, community participation has evolved through the involvement of CHWs in the implementation and delivery of health services and care, including immunisation.
Multi-purpose community health workers are widely used to solve a range of health problems. However, little is known about the effectiveness of their interventions. The main objective of this article is to share an experience on the role of multipurpose community health workers in the effort to identify, sensitise and ensure the catch-up of zero-dose children during the meningitis vaccination campaign implemented from 12 to 16 June 2024 in two health districts in the North region of Cameroon.
Methodology
The methodology of this study is based on the presentation of the data (nature and sources) and the description of the analysis approach. This study focuses on the two health districts (Lagdo and Ngong) that were the subject of a preventive vaccination campaign against meningococcal meningitis ACYW-135 in the North region. The campaign ran from 12 to 16 June 2024.
Cameroon, and more specifically the northern region, is one of the areas that make up the meningitis belt, with more cases diagnosed. To prevent the severe form of the disease, WHO Afro donated more than 227,647 doses of MenACYW-135 vaccine to Cameroon. Given the limited number of doses, the health districts of Lagdo and Ngong in the North region were given priority for the distribution of MenACYW-135 vaccines.
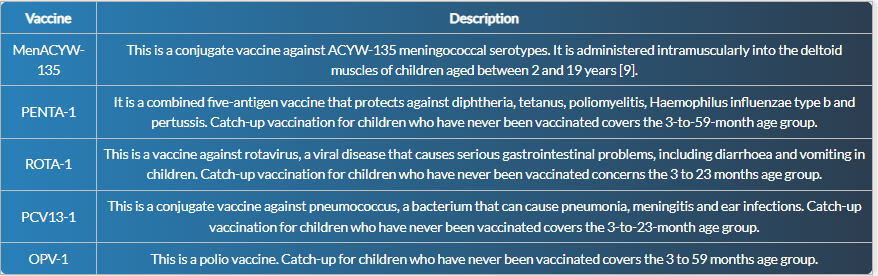
In 2012, a mass vaccination campaign against meningococcal A was carried out in the Extreme North, North, Adamaoua and North-West regions of the country. Considering that child born after this campaign had not been vaccinated, the Ministry of Public Health and partners decided to include children aged 2 to 15 in the main intervention, vaccination against meningitis. In addition to the main intervention, which focused on vaccination against meningitis, this activity also included another intervention to vaccinate zero-dose children and the under-vaccinated. In Cameroon, a zero-dose child is a child who has not been vaccinated with PENTA-1, even though he or she is eligible. As part of this intervention, children not vaccinated with OPV-1, ROTA-1 and PCV13-1 were also included.
Table 1: Description of the vaccines used during the campaign.
The data collected and used during this vaccination campaign is quantitative and from primary sources. It comes from the health areas of the districts concerned. In these areas, the Multipurpose Community Health Workers are acting as social mobilisers.
- Community Health Worker (CHW): A man or woman belonging to a community, chosen and supported by the community, and trained for a short period to deal with its health problems under the supervision of the health services [10].
- Multipurpose Community Health Worker (MCHW): Community Health Worker trained and able to implement interventions from several programmes within the same community [10].
Social mobilisation is a process aimed at raising awareness, informing and mobilising communities, families and individuals to take an active part in the vaccination campaign. Three days before the actual start of the vaccination campaign, the social mobilisers visited households in the targeted health zones, mainly to pass on general messages about vaccination, and more specifically to inform people that vaccinators would be visiting soon, to mark the homes of the targeted populations to guide the vaccinators, and to orientate the targeted people and/or their guardians and maintain order in the vaccination posts. The social mobilisers also acted as town criers, using a megaphone to announce the activities. A social mobiliser was identified as any volunteer who was polite, literate, familiar with the areas of the community in which he/she worked and culturally able to interact easily with the community. It is important to note that these health workers, also known as Multipurpose Community Health Workers, are already known in all the health districts of Cameroon.
In addition to social mobilisation, the Multipurpose Community Health Worker also carries out case studies. The head of the health area uses the register of routine vaccinations to sort out the children who have started vaccination and who have been lost to follow-up. In each area covered by the MCHW, a list is drawn up by the head of the health area and given to the MCHW to actively look for children in the community. Once the children have been identified, they are directed and monitored by the MCHW to the nearest vaccination site or post to receive the missing vaccine(s). On arrival at the vaccination post, the vaccination team checks the child's vaccination record to see which vaccine he or she is due to receive at that age. Once the vaccine has been administered and the appropriate documentation has been drawn up, the MCHW contacts the parents and ensures the child's subsequent and ongoing follow-up.
To respond to our problem, the analysis approach is based on a descriptive analysis of the data relating to the performance indicators of the social mobilisation and vaccination activities. It will highlight the efforts of the Multipurpose Community Health Workers in improving immunisation coverage, by ensuring that children missed or not reached by the usual health services are included in the immunisation campaign.
Results and Discussion
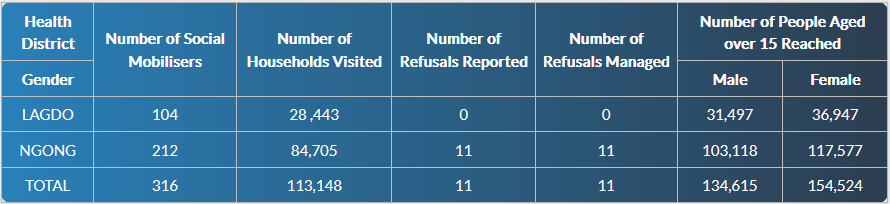
As part of the catch-up of zero-dose children, the first role of the Multipurpose Community Health Worker was to identify these children, particularly through home visits and by identifying areas where vaccination services may be less accessible. The vaccination campaign as a whole mobilised 316 multi-purpose community health workers: 104 in the Lagdo health district and 212 in Ngong. Household visits resulted in 113,148 households being visited in the two health districts. The aim of these visits was to raise awareness in households about meningitis vaccination and also about the importance of vaccinating children aged 0-59 months who had never been in contact with vaccination. In addition, all reported cases of refusal were managed by community players. This shows the effort made by these Multipurpose Community Health Workers to establish a relationship of trust with families, understand their concerns and respond to them in an empathetic and respectful manner. In addition, awareness-raising was not limited to households; a total of 289,139 people were reached.
Table 2: Results of social mobilisation for the vaccination campaign.
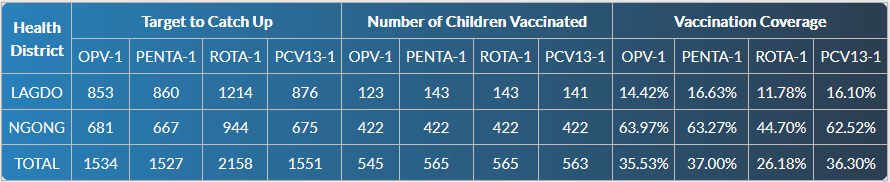
As part of the catch-up programme for zero-dose children, Multipurpose Community Health Workers had identified 1,527 children aged 0-59 months who had not received their first dose of pentavalent vaccine in the two districts prior to the campaign. In addition, these community players organised local campaigns to encourage parents to have their children vaccinated. The Multipurpose Community Health Workers also directed parents wishing to have their children vaccinated to fixed vaccination posts. By the end of the campaign, 565 children under the age of 5 had been vaccinated with PENTA-1, representing 37% coverage of the target to be caught up. For antigens administered in conjunction with PENTA-1, 545, 565 and 563 children were vaccinated with OPV-1, ROTA-1 and PCV13-1 respectively.
Table 3: Zero-dose children caught up with vaccinations.
The catch-up of zero-dose children during the meningitis vaccination campaign in the Nord region was a significant public health intervention aimed at preventing infectious diseases and reducing morbidity in children under the age of 5. This intervention was one of the objectives of the campaign. The data from this vaccination campaign show that the Multipurpose Community Health Workers played a key role in reducing the number of zero-dose children, thanks in particular to their proximity to households and their awareness-raising efforts. These observations corroborate Benin's experience, which has shown that CHWs also play a key role in strengthening the Expanded Programme on Immunisation (EPI), in particular by encouraging routine immunisation, especially for zero-dose children [11].
During this vaccination campaign, there was a low coverage of zero-dose children (37%). This can be explained by the fact that this event mainly targeted children aged between 2 and 15 who wanted to be vaccinated against meningitis. The catch-up of zero-dose children was only a secondary intervention. The Big Catch-up is the main intervention in which the Government, through the Ministry of Public Health, aims to catch up children who have missed their routine immunisation. It would be useful to use the experience of the Big Catch-up to extend the analysis carried out in this study to a wider population and to carry out longitudinal studies to assess the impact of catch-up strategies over the long term.
Conclusion
Vaccination is a simple, safe, and effective way of protecting people against harmful diseases, before they come into contact with them. It uses your body's natural defences to build resistance to specific infections and makes your immune system stronger. One of the goals of the Immunization Agenda 2030 is that everyone is protected by full immunization, regardless of location, age, socioeconomic status or gender-related barriers.
Zero-dose children and the under-vaccinated must not be sidelined. To achieve these targets, the country will be able to rely on the Multipurpose Community Health Workers who operate in the various health districts. Their efforts have been essential in improving zero-dose immunisation coverage and protecting children against preventable diseases. Their work also helps to build confidence in local health systems. During the meningitis vaccination campaign conducted from 12 to 16 June 2024, catch-up vaccination of zero-dose children was included and 37% of these children were vaccinated with PENTA-1 in the Lagdo and Ngong health districts.
Vaccination campaigns offer a considerable opportunity to catch up with zero-dose or under-immunised children. Micro-planning must always take into account the involvement of multi-purpose community health workers in actively seeking out and possibly referring these children for vaccination.
References
- WHO. Vaccines and Immunization. World Health Organization.
Publisher | Google Scholor - Immunization Agenda 2030: A Global Strategy to Leave no one Behind. (2020). World Health Organization.
Publisher | Google Scholor - WHO. (2024). Vaccination Coverage. World Health Organization.
Publisher | Google Scholor - UNICEF. (2024). Digital for Zero-Dose: Harnessing AI for Global Health Equity.
Publisher | Google Scholor - Njoh, A. A., Saidu, Y., Bachir, H. B., Ndoula, S. T., Mboke, E., et al. (2022). Impact of Periodic Intensification of Routine Immunization Within an Armed Conflict Setting and COVID-19 Outbreak in Cameroon in 2020. Conflict and Health, 16(1):29.
Publisher | Google Scholor - Silva CD. (2023). Cameroon Increases Reach to Zero Doses in Children Through Micro-Planning and Communication.
Publisher | Google Scholor - World Health Organization. (2017). Community Health Worker Programmes in The WHO African Region: Evidence and Options-Policy Brief.
Publisher | Google Scholor - Minsante. 2021-2025 National Strategic Plan for Community Health in Cameroon.
Publisher | Google Scholor - World Health Organization. (2024). Meningococcal Vaccines: WHO Position Paper on The Use of Multivalent Meningococcal Conjugate Vaccines in Countries of The African Meningitis Belt, January 2024. Weekly Epidemiological Record, 12.
Publisher | Google Scholor - Minsante. (2024). Community Health the Revised Guide to Community-Directed Interventions in Cameroon.
Publisher | Google Scholor - Community Health Workers on The Frontline Against Vaccine-Preventable Diseases in Benin. VaccinesWork. (2024).
Publisher | Google Scholor























