

Case Report
Technical Note on Humeral Head Reconstruction for Large Reverse Hill Sachs Lesions
- Y.V. Kleinlugtenbelt MD PhD
- Koen Philippe van den Berg MD *
- S. Grewal MD PhD
- I. Kilsdonk MD
- E. Landman PhD
Department of Orthopaedic and Trauma Surgery, Deventer Ziekenhuis, GC Deventer, The Netherlands.
*Corresponding Author: Koen Philippe van den Berg MD, Department of Orthopaedic and Trauma Surgery, Deventer Ziekenhuis, GC Deventer, The Netherlands.
Citation: Kleinlugtenbelt Y.V., Van den Berg. K.P. MD, Grewal S., Kilsdonk I., Landman E. (2026). Technical Note on Humeral Head Reconstruction for Large Reverse Hill Sachs Lesions, Clinical Case Reports and Studies, BioRes Scientia Publishers. 12(1):1-5. DOI: 10.59657/2837-2565.brs.26.298
Copyright: © 2026 Koen Philippe van den Berg, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 24, 2025 | Accepted: January 07, 2026 | Published: January 14, 2026
Abstract
Posterior locked shoulder dislocation is a rare injury and can result in an anteromedial humeral head impression fracture called a reverse Hill Sachs defect. Reconstruction of the humeral head using osteochondral allograft transplantation is a recognized treatment option for moderate to large defects. However, it is challenging to exactly create and adjust the segment according to the dimensions of the defect. We report a novel technique to increase accuracy in measuring the size of the allograft and obtain optimal fitting of the reverse Hill Sachs defect.
Keywords: posterior shoulder dislocation fracture; reverse hill-sachs lesion; anatomical reconstruction; allograft
Introduction
Posterior shoulder dislocation is a rare injury and accounts for 5% of all shoulder dislocations [1]. An extreme muscle contraction (seizures or electric shock), a direct or indirect trauma that occurs with flexion, adduction and internal rotation of the affected arm, is pathognomonic for the posterior shoulder dislocation [2, 3]. Through a mechanism similar to that first characterized by Hill and Sachs, posterior shoulder dislocations have the potential to result in impaction fractures of the anterior aspect of the humeral head, so-called reverse Hill-Sachs or McLaughlin lesions [4-6]. Reverse Hill-Sachs lesions are estimated to occur in 86% of acute traumatic posterior shoulder dislocations and are often clinically significant, giving rise to persistent shoulder instability in approximately 35% of the cases [4, 7]. Previous studies have suggested surgical reconstruction in cases with >20% loss of the articular surface [8]. Segmental allograft reconstruction has been described in several studies. To yield the necessary interference fit, this technique requires the creation of a cylindrical site on the humeral head into which a similarly shaped graft is press-fit. It is noted that sometimes the allograft may not be shaped good enough to precisely fill the entirety of the bony defect. The present study demonstrates a relatively simple addition to the existing surgical technique to overcome this problem and more accurately shape the allograft.
Case Series
The present study describes the novel technique performed in 4 patients (mean age 29 years) with a chronic posterior locked shoulder dislocation, including 1 patient with a bilateral posterior locked shoulder dislocation. Two patients presented with a concurrent fracture of the proximal humerus, in which the posterior shoulder dislocation was initially missed. In all patients, physical examination of the upper extremities elicited shoulder pain with limited passive range of motion. Neurovascular examination was otherwise normal. Radiographs and computed tomography (CT) scan were obtained in our standard preoperative work-up, and indicated a posterior locked shoulder dislocation with a medium size reverse Hill-Sachs lesion (impaction of 25%-40% of the humeral head articular surface) (Figure 1).
Approval by the institutional review board was waived due to the retrospective design of this study.
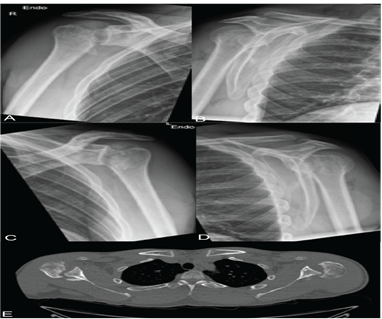
Figure 1: Radiographs of the right (A-B) and left (C-D) shoulder of a 28-year-old patient with a bilateral posterior locked glenohumeral dislocation, showing the humeral head articular surface projected beyond the glenoid edge. Computed tomography (CT) confirming posterior dislocation of the humeral head with impaction on the glenoid resulting in a reverse Hill Sachs lesion (E).
Methods (surgical technique)
General anesthesia and an interscalene block were provided in all patients. The surgery was performed in beach-chair position and a deltopectoral approach was used to reach the shoulder joint and visualize the head defect. The longer the shoulder remains dislocated, the harder it is to relocate due to muscular spasm and capsular tightening. Furthermore, heavy callus formation was observed at the posterior margin of the glenoid fossa in all our patients (Figure 1), obstructing the reposition. General anesthesia combined with muscle relaxant followed by tenotomy of the subscapularis tendon and a gentle use of a Fukuda retractor together aided in reposition the humeral head. Following repositioning the humeral head, the Hill-Sachs lesion was exposed and debrided (Figure 2A-B). The impressed cartilage with adjacent cortical and spongiotic bone was removed and sharp edges were created using an oscillating saw (Figure 2C). The lesion was estimated to involve at least 25% of the articular surface of the humeral head in all patients. Appreciation of the measurements and hence accurate restoration of the original shape of the humeral head is difficult. Senior author Y.V.K. uses a novel technique overcoming this problem to create an optimal fitting of the allograft. After protecting the surface of the bone defect, such as with a plastic paper, it is filled with bone cement (Figure 2D). The cement is adapted as exactly as possible to the bony defect situation. This method of creating a three-dimensional figure of bone cement is helpful in more accurately predicting the measurements and shape of the allograft that needs to fill the lesion as it enables easy visual inspection of the dimensions (Figure 2E). Subsequently, a segment is cut from the allograft head of femur to match the defect and radius of curvature of the patient’s humeral head (Figure 2F). The graft is then placed into the prepared bed, gently pushed by hand, such that the entire graft is flush to adjacent native cartilage (Figure 2G). Following, the graft is assessed for stability by gentle internal and external rotation. It is then secured in place with the use of two or three headless compression screws (Figure 2H-I). With the humeral head surface restored, the subscapularis tendon is then repaired.
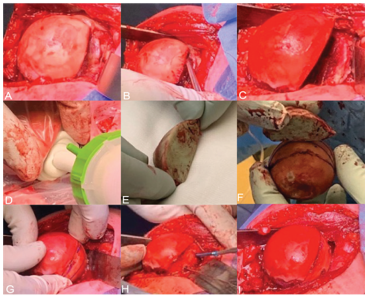
Figure 2: The reverse Hill-Sachs lesion is exposed and debrided (A-B). The defect is reshaped and sharp edges are created (C) and subsequently filled with cement to create a 3-dimensional model (D-E). A wedge of the allograft is produced on the back table after measuring the length, width and depth of the cement model (F) after which the graft is placed in the defect (G). Final fixation is secured with 2 or 3 headless compression screws in the humeral head (H-I).
Postoperative management
All four patients had their upper limb kept in a patient tailored orthosis in 15-20 degrees of internal rotation (to reduce the risk of re-rupture of the shortened subscapularis) for 4 weeks, after which passive mobilization was allowed. Twelve weeks postoperatively, active mobilization followed by full range of motion were permitted.
Follow-up examinations were done 6 weeks, 3 and 6 months post-operatively or until union and proper incorporation of the graft was seen. Patients’ clinical examination was combined with X-rays and a CT-scan at 3 and 6 months for incorporation of the graft and the congruency of the joint.
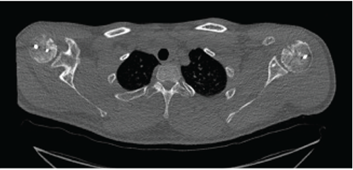
Figure 3: Postoperative Computed tomography (CT) illustrating proper incorporation of the humeral head using osteochondral allograft transplantation.
Results
Postoperative computed tomography at 3 months indicated the subchondral portion of the graft in near-anatomic alignment with signs of bone bridging and healing, concluding proper incorporation of the graft to the surrounding bone. All shoulders were free from re-dislocation at time of final follow-up with no signs of degenerative changes or avascular necrosis on computed tomography (mean follow-up 6 months).
Discussion
Management of moderate to large reverse Hill-Sachs defects is a challenging clinical situation in young patients. Options include disimpaction [9-11], soft tissue procedures such as remplissage [12], the McLaughlin procedure [6, 13], osteochondral allograft [14-16] and joint arthroplasty [17]. Two of the presented patients were initially treated at outside hospitals and were referred to our institution. Though an arthroplasty was recommended previously, given their age and the size, location, and engaging nature of the lesion in combination with the intact anatomy of the glenoid, we advised an osteochondral allograft.
Segmental allograft reconstruction has its own shortcomings such that it is difficult to precisely create and adjust the segment according to the dimensions of the defect. The current paper describes a relatively simple and novel addition to the surgical procedure which increases the accuracy and ensures an anatomic situation of the humeral head and subsequent reconstruction of the joint line. To our best knowledge, such has not been described in the literature and we feel that it adds to the current knowledge of the procedure.
Declarations
Acknowledgements
The authors hereby declare we did not receive any financial or moral support for the publication of this article.
Sources of support
The authors hereby declare we did not receive any financial or moral support for the publication of this article.
Conflict of interest declaration
The authors certify that neither they nor their immediate family members maintain any funding sources or commercial affiliations, including consultancies, equity interests, stock ownership, or patent/licensing arrangements, that could present a conflict of interest with respect to the submitted article.
References
- Zacchilli, M. A., & Owens, B. D. (2010). Epidemiology of shoulder dislocations presenting to emergency departments in the United States. The Journal of Bone and Joint Surgery. American Volume, 92(3):542–549.
Publisher | Google Scholor - Cicak, N. (2004). Posterior dislocation of the shoulder. The Journal of Bone and Joint Surgery. British Volume, 86(3):324–332.
Publisher | Google Scholor - Perron, A. D., & Jones, R. L. (2000). Posterior shoulder dislocation: Avoiding a missed diagnosis. The American Journal of Emergency Medicine, 18(2):189–191.
Publisher | Google Scholor - Robinson, C. M., & Aderinto, J. (2005). Posterior shoulder dislocations and fracture-dislocations. The Journal of Bone and Joint Surgery. American Volume, 87(3):639–650.
Publisher | Google Scholor - Robinson, C. M., Seah, M., Akhtar, M. A., & Jenkins, P. J. (2011). The epidemiology, risk of recurrence, and functional outcome after an acute traumatic posterior dislocation of the shoulder. The Journal of Bone and Joint Surgery. American Volume, 93(17):1605–1613.
Publisher | Google Scholor - McLaughlin, H. L. (1952). Posterior dislocation of the shoulder. The Journal of Bone and Joint Surgery. American Volume, 34(3):584–590.
Publisher | Google Scholor - Saupe, N., White, L. M., Bleakney, R., et al. (2008). Acute traumatic posterior shoulder dislocation: MR findings. Radiology, 248(1):185–193.
Publisher | Google Scholor - Baudi, P., Campochiaro, G., Rebuzzi, M., et al. (2013). Assessment of bone defects in anterior shoulder instability. Joints, 1(1):40–48.
Publisher | Google Scholor - Assom, M., Castoldi, F., Rossi, R., et al. (2006). Humeral head impression fracture in acute posterior shoulder dislocation: New surgical technique. Knee Surgery, Sports Traumatology, Arthroscopy, 14(7):668–672.
Publisher | Google Scholor - Bock, P., Kluger, R., & Hintermann, B. (2007). Anatomical reconstruction for reverse Hill-Sachs lesions after posterior locked shoulder dislocation fracture: A case series of six patients. Archives of Orthopaedic and Trauma Surgery, 127(7):543–548.
Publisher | Google Scholor - Engel, T., Hepp, P., Osterhoff, G., et al. (2009). Arthroscopic reduction and subchondral support of reverse Hill-Sachs lesions with a bioabsorbable interference screw. Archives of Orthopaedic and Trauma Surgery, 129(8):1103–1107.
Publisher | Google Scholor - Purchase, R. J., Wolf, E. M., Hobgood, E. R., et al. (2008). Hill-Sachs “remplissage”: An arthroscopic solution for the engaging Hill-Sachs lesion. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 24(6):723–726.
Publisher | Google Scholor - Krackhardt, T., Schewe, B., Albrecht, D., et al. (2006). Arthroscopic fixation of the subscapularis tendon in the reverse Hill-Sachs lesion for traumatic unidirectional posterior dislocation of the shoulder. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 22(2):227.e1–227.e6.
Publisher | Google Scholor - Gerber, C., & Lambert, S. M. (1996). Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. The Journal of Bone and Joint Surgery. American Volume, 78(3):376–382.
Publisher | Google Scholor - Martinez, A. A., Calvo, A., Domingo, J., et al. (2008). Allograft reconstruction of segmental defects of the humeral head associated with posterior dislocations of the shoulder. Injury, 39(3):319–322.
Publisher | Google Scholor - Martinez, A. A., Navarro, E., Iglesias, D., et al. (2013). Long-term follow-up of allograft reconstruction of segmental defects of the humeral head associated with posterior dislocation of the shoulder. Injury, 44(4):488–491.
Publisher | Google Scholor - Checchia, S. L., Santos, P. D., & Miyazaki, A. N. (1998). Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. Journal of Shoulder and Elbow Surgery, 7(1):53–65.
Publisher | Google Scholor























