

Research Article
Technical Capacities of Community-Based Organizations (CBOs) to Provide Health Services (HIV/AIDS, Tuberculosis, Hepatitis B, Sexually Transmitted Infections and Reproductive Health) to Key Populations in Cameroon in 2022
- Gislain Lionnel Mbita 1,2*
- Henry Olivier Ondoa 2,5,6
- Ernest Desire Mvilongo Anaba 2
- Rose Armelle Ada 3
- Tena Ngounga Arouna 4
- Caroline Medouane 2
- Albert Franck Zeh Meka 1,2
- Joseph Fokam 2
- Serge Clotaire Billong 3
1Field Epidemiology Training Program, Cameroon.
2Central Technical Group of The National Committee for The Fight Against AIDS, Ministry of Public Health, Cameroon.
3Sub-Directorate for The Fight Against HIV/AIDS, Sexually Transmitted Infections and Tuberculosis, Ministry of Public Health, Cameroon.
4World Health Organization, Cameroon.
5Cameroon Project Management Association, Cameroon.
6International Project Management Association, Cameroon.
*Corresponding Author: Ghislain Lionnel Mbita, Central Technical Group of The National Committee for The Fight Against AIDS, Ministry of Public Health, Cameroon
Citation: Mbita GL, Ondoa HO, Anaba EDM, Ada RA, Arouna TN, et al. (2025). Technical Capacities of Community-Based Organizations (CBOs) to Provide Health Services (HIV/AIDS, Tuberculosis, Hepatitis B, Sexually Transmitted Infections and Reproductive Health) to Key Populations in Cameroon in 2022, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(1):1-12. DOI: 10.59657/2997-6103.brs.25.072
Copyright: © 2025 Ghislain Lionnel Mbita, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 03, 2025 | Accepted: June 16, 2025 | Published: June 23, 2025
Abstract
Introduction: Cameroon is committed to increasing equity in access to care by adhering to the provisions of the ALMA-ATA declaration in 1978. The 2021-2023 National Strategic Plan (NSP) for the fight against HIV prioritizes community-led interventions through associations and Community-Based Organizations (CBOs) to reach key populations. The objective of this study was to assess the technical capacities of CBOs to provide quality services as stipulated in the national task delegation guide validated in 2013.
Methodology: This cross-sectional study was conducted in CBOs from June to July 2022 in ten regional capitals of Cameroon including Limbe and Kribi. Data were collected through the KoboCollect platform using a structured assessment grid inspired by the CBO assessment grid of the Global Fund/ Camnafaw /CHAMP projects, the Task Delegation Guide (GDDT) and the community ARV dispensation guide. Variables focused on human and material resource capacities and service availability made it possible to classify CBOs into low, acceptable, good and very good technical capacity to provide HIV, tuberculosis (TB), Hepatitis B, Sexually Transmitted Infections (STIs) and Reproductive Health (RH) health services. Data analysis was carried out using SPSS and Excel to ensure statistical reliability.
Results: The assessment included 58 CBOs, revealing that 11.9% (7/58) had low technical capacity, compared to 33.9% (20/58) acceptable, and 47.7% (28/58) good to provide HIV services. For the provision of TB services, 60.3% (37/58) had low technical capacity, 32.76% (19/58) acceptable and 3.2% (2/58) very good. Furthermore, the majority of CBOs, 87.9% (51/58) had low capacity to provide hepatitis B services. While 75.86% (44/58) and 24.14% (14/58) had low and acceptable technical capacity to provide STI/RH services, respectively.
Conclusion: The assessment highlights the varied technical capacities of CBOs to provide comprehensive HIV, TB, hepatitis B and STI/RH health services to key populations in Cameroon. However, they make a lasting contribution to strengthening care provision. There is a need to revise the GDDT and strengthen the technical capacities of CBOs to improve operational efficiency.
Keywords: community-based organizations; key populations; HIV; Cameroon
Introduction
In Cameroon, the PSN identifies TS, MSM, UD/UDI, TG as a key population for HIV infection. However, the prevalence of HIV among certain groups of this population, notably Sex Workers (24.3%) and Men who have sex with Men (20.7%), remains significantly high compared to the national average of 2.7% [1] (CNLS, 2020). Geographically, 6 out of 10 regions have a prevalence above the national average (2.7%), namely the South 5.8%, the East 5.6%, Adamaoua 4.7%, the North-West 4%, the Center (excluding Yaoundé) 3.5% and the South-West 3.2% [2].
As part of the response, Cameroon adheres, among other things, to the WHO Declaration on Primary Health Care at ALMA-ATA in 1978 [3] which emphasizes the promotion of decentralization of health services to communities in order to increase equity in access to care. The country's commitment to this end is reflected in the development and validation, among other things, of the “National Guide for Delegating Tasks for HIV/AIDS Management at the Operational Level” in 2013.
Furthermore, the PSN 2021-2023 guidelines [4] focus on prioritizing interventions in terms of population targets and geographic coverage. Community-based interventions are given pride of place for all impact outcomes, particularly within community-based associations and organizations. The main issue concerns HIV infection and associated coinfections (TB, Hepatitis B, and other STIs).
To date, thanks to the combined efforts of all stakeholders in the response to the epidemic, remarkable progress has been made and encouraging results recorded in terms of a continued decline in new infections (-48 percentage between 2010 and 2019) and deaths (-37 percentage between 2010 and 2019), as well as the increase in antiretroviral (ARV) treatment coverage for people living with HIV (PLHIV) estimated at 81.1% in June 2021 [5] (CNLS 2021).
Despite these advances, many challenges persist at the programmatic and financial levels to achieve the “95-95-95” goals and eliminate the epidemic by 2030, especially for key populations [6]. There is therefore a need to strengthen the decentralization of services and the delegation of tasks to the community level. In a context where new strategies are being developed to match the dynamics of the epidemic; among underserved or poorly served populations and reduce the problems associated with stigma and discrimination. It would be appropriate to implement the Final Declaration of the last regional summit on HIV in West and Central Africa [7]. This called for the development of innovative community response strategies to the Pandemic. This will include Strengthening the infrastructure of community organizations [...] through the adoption of appropriate health policies and the mobilization of sustainable financing [7].
To this end, given the increasingly important place given to differentiated services (demedicalized screening, community dispensation of ARVs, human rights, etc.), improving the package of interventions of community-based organizations and their scaling up requires capacity building that complies with standards and qualities adapted to the needs of key populations and recommended in the fight against HIV.
In order to ensure capacity building for community actors and with a view to improving the quality of HIV care for key populations, the national AIDS control program, with the technical support of WHO, intends to assess the capacities of community-based organizations working for the benefit of key populations. This will make it possible to propose an improvement to the national task delegation guide in order to align it with current requirements for the provision of people-centered services, and to enable community-based organizations to improve their capacities in the provision of HIV, TB, Hepatitis B, SR and STI services.
Objectives
General Objective
Assess the capacities of Community Based Organizations (CBOs) in providing HIV, TB, Hepatitis B, STI and reproductive health (RH) services to key populations in Cameroon
Specific Objectives
- Map CBOs providing HIV, TB, Hepatitis B, STI and reproductive health services to key populations according to the 10 priority clinical care standards.
- Human resources of CBOs providing HIV, TB, Hepatitis, STI and reproductive health services to key populations.
- Evaluate the material resources (equipment and materials, tools, documentation and reporting system, attendance) of OBC KPs.
- HIV, TB, Hepatitis B, STI and reproductive health services in OBC KP.
Determine the overall technical capabilities of OBCs.
Methodology
Type of Study
This was a cross-sectional study.
Study Sites
The study was conducted in the identity and non-identity OBCs of key populations (Sex workers, Men who have Sex with Men, Transgender, Drug users and Injectable Drug users) in ten (10) regional capitals including Limbe and Kribi.
Table 1: Distribution of the various reference OBCs and FOSAs by region, June 2022.
| Region | SITES | ||
| Identity OBCs | Non-identity OBCs | FOSA | |
| Adamaoua | 3 | 2 | 1 |
| Center | 6 | 3 | 1 |
| East | 3 | 3 | 1 |
| Far North | 3 | 2 | 1 |
| Coastline | 6 | 3 | 1 |
| North | 3 | 2 | 1 |
| Northwest | 3 | 3 | 1 |
| West | 3 | 3 | 1 |
| South | 3 | 2 | 2 |
| Southwest | 3 | 2 | 2 |
| National | 36 | 25 | 12 |
Study Period
The study took place over the period from June to July 2022 and the data collection lasted 05 days.
Study Population
The study population consisted of managers of:
- Community-Based Identity Organizations of TS, MSM, TG, UD and IDU.
- Non-identity Community-Based Organizations of TS, MSM, TG, UD and IDU.
Inclusion Criteria
- OBC identity of TS, MSH, TG, UD and UDI.
- STI/HIV/AIDS/TB and SR services to KPs.
- Responsible for identity or non-identity OBC of TS, MSH, TG, UD and UDI.
Exclusion Criteria
- Refusal of the person responsible for the participation of the OBC.
Sampling
Sampling and Selection Procedures of OBCs
The identity or non-identity OBCs of the TS, MSH, TG, UD and UDI of the 10 regions of Cameroon were identified.
Sample Size Calculation of OBC (TS, MSH, TG, UD and IDU)
The number of study sites was calculated according to the criteria recommended by WHO and taking into account the estimation of the size of key populations [2] and the seropositivity of key populations (TS, MSM, TG, UD and IDU) [6]. The distribution by region was made taking into account the weight of the estimation of the size of the population by region.
Thus, the number of CBOs required to assess the capacity of community-based organizations to provide HIV/AIDS services to a population with a precision i = 0.025 and for a fixed risk α = 0.05 (Z α /2 = 1.96) is given by the following formula: Or

P=proportion of the active queue of OBCs
i=accuracy of the estimate
Zα/2=reduced deviation for risk α =0.05
Table 2: Indicators used to estimate the sample size in Cameroon, 2022.
| Population Types | Population Size | Number of Tests in 2020 | Number of Positive Tests in 2020 | HIV Positivity in 2020 | Source | Calculated Sample Size |
| Key Populations | 89,781 | 110,867 | 13,406 | 0.12 | 2020 Annual Report Mapping_Programmatic_Estimation_TS-HSH-UD-Teenagers-young people_CM_VF | 77 OBC |
Data Collection Tool
For data collection, an OBC evaluation grid, a questionnaire for reference FOSAs and a beneficiary satisfaction questionnaire were developed and then digitized using the KoboCollect online platform. These tools were developed from the following documents:
- National guide to task delegation.
- The ten standards of priority clinical care.
- National guide to community dispensing of ARVs.
- Evaluation grid for CBOs of Global Fund/ Camnafaw and CHAMP projects.
Pre-Test
The pre-test took place in 02 OBC and 1 FOSA for (03) three days. This activity made it possible to improve the quality of the tools developed, to reformulate certain questions, to identify and correct inconsistencies.
Data Collection Procedures
In each OBC selected for the survey, the investigators, equipped with the service notes, met with the heads of the structures (FOSA, OBC) and explained to them the purpose and objectives of the evaluation. After the consent of the head of the OBC/FOSA, the questionnaire was administered.
The beneficiaries were enrolled consecutively after their consent in the OBCs.
Ethical Considerations
As part of this study, personal data was not collected, but compliance with the requirements of ethics in human health research was observed, in particular:
- Voluntary participation of those responsible for the enrolled structures.
- Respect for the people interviewed.
- The autonomy of the leaders of the various OBCs surveyed.
- The confidentiality of the information obtained.
However, administering the questionnaire took the participant a few minutes.
The OBCs and their clients received a briefing on the service package and regulatory documents.
The FOSAs were made aware of the need to coach the OBCs under their supervision.
Data Management and Analysis
Data Monitoring
Data monitoring was carried out by two data managers. This enabled the reliability, accuracy, and consistency of data entered into the forms submitted to the platform by investigators to be monitored and verified in real time.
Data Analysis
An analysis and tabulation plan were developed to generate tables and graphs based on themes, items and indicators.
After data cleaning, analysis was done using SPSS and Excel software. The data from the analysis were described using numbers, proportions and presented in the form of tables and graphs.
Study Variables
The main variable of interest “Overall technical capacity of the OBC” is a composite variable and was defined as an ordinal variable (low, acceptable, good and very good). The judgment criterion for this variable is the proportion of OBCs classified in each of its categories (low, acceptable, good and very good). It was constructed from the indicators:
- Technical capacity in human resources (22 items).
- Technical capacity in material resources (11 items).
- Technical capacity in HIV service provision (16 items).
- Technical capacity in TB service offering (5 items).
- Technical capacity in hepatitis B service provision (5 items).
- Technical capacity in IST/SR service provision (14 items).
To assess the variable “Overall technical capacity of the OBC”, the calculation of the scores was carried out by weighting the items of each indicator. The items of each of the indicators had the same weight, i.e., 1 point if the item was "yes" and 0 if the item was "no". The score ranged from 0 to 108 points. Moreover, it was decided that the indicators relating to HIV, TB, HVB and SR service offers contributed 60% and the other indicators 40% to the construction of the variable Overall technical capacity of the CBO. The total scores after weighting ranged between 0 and 1 and served as a basis for assessing this variable. Thus, the overall technical capacity of the CBO was low if the score was less than 0.5, acceptable if the score was between 0.5 and 0.7, good if the score was between 0.8 and 0.9 and very good if the score was greater than 0.9. The main variable of interest was the overall technical capacity of the CBOs. The secondary variables of interest of the study were the technical capacity of OBCs to offer health services to key populations. These are composite variables constructed from the indicators:
- Human Resources.
- Material resources.
- Availability of HIV, TB, HVB, STI/SR services.
Judgment Criteria
This is the proportion by Weighting of OBCs with weak, acceptable, good and very good technical capacities:
- Low (below the indicator average).
- Acceptable (around the indicator average).
- Good (above average below the maximum of the indicator).
- Very good (close to the maximum value of the indicator).
Survey Implementation Procedures
The implementation of the study took into account the development and validation of the protocol and collection tools; compliance with administrative procedures; briefing of investigators, pre-testing and the actual data collection.
Results
Mapping CBOs Providing HIV, TB, HVB, STI and SR Services to Key Populations
The field visit made it possible to assess 58 OBCs, including 27 identity groups and 31 non-identity groups, and to draw up a map of OBCs according to their profiles and areas of intervention.
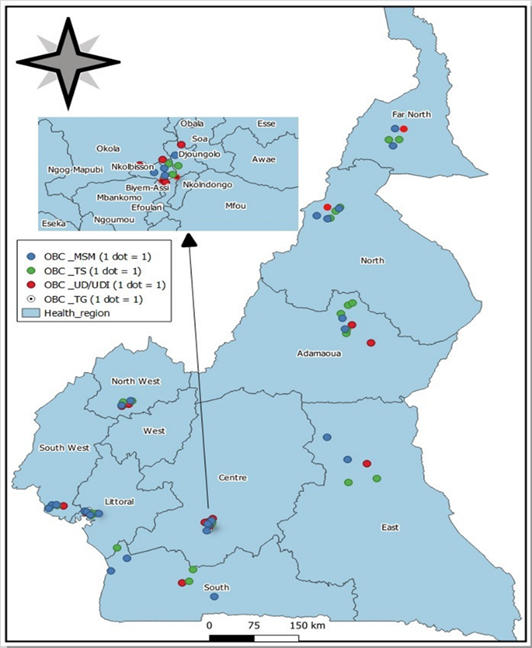
Figure 1: Location of OBCs assessed by type of target in the health regions of Cameroon, June 2022.
Distribution of OBCs by Areas of Intervention
The table below shows the distribution of OBCs by areas of intervention in the sites concerned in the 10 Regions of Cameroon.
Table 3: Distribution of OBCs by area of intervention, June 2022.
| OBC | Areas of intervention | Numbers (N=58) | Percentage (%) |
| HIV | 44 | 100.00 | |
| HIV+TB | 21 | 47.73 | |
| HIV+ STI/SR | 4 | 9.09 | |
| HIV+TB+ STI/SR | 12 | 27.27 | |
| HIV+TB+HBV + STI/SR | 1 | 2.27 |
Human Resource Capacities of CBOs Providing HIV, TB, HVB, STI/RH Services to Key Populations in Cameroon
In general, there is availability of staff dedicated to providing services. However, this availability depends on the services offered within the CBOs. Upon observation, in the DICs, a more comprehensive staff covering the 3 (95) for HIV was noted, which was not the case in the CBOs without DICs. The most frequent proportion of staff in the CBOs was that of peer educators (11.72%), followed by mobilizers (7.23%). Staff dedicated to monitoring and evaluation and GAS were available in 92.98% of the CBOs. It should be noted that the staff available in the CBOs reported having been trained through capacity building sessions within the framework of ongoing projects (CARE/Champ, CAMNAFAW/Global Fund). The CBOs were frequently capable of community mobilization (84.21%) and HIV screening (82.46%). As for the specialized staff (doctors, nurses and laboratory technicians), they are mostly service providers and therefore their interventions are not continuous.
Table 4: Availability of human resources in OBCs, Cameroon, June 2022.
| Labels | Response Methods | Staff | % |
| Average number of staff available to the OBC/DIC | Peer educator | 11.72 | |
| CPS | 2.19 | ||
| APS | 2.68 | ||
| Nurse | 0.81 | ||
| Doctor | 0.42 | ||
| The mobilizers | 7.23 | ||
| Laboratory technician | 0.81 | ||
| An accountant | 1.28 | ||
| Psychologist | 0.28 | ||
| Dispenser | 0.75 | ||
| Availability of staff dedicated to monitoring, evaluation and GAS | 1- Yes | 53 | 92.98 |
| 2-No | 4 | 7.02 | |
| Proportion of OBC capacity for certain services | Management of HIV, STI, TB, Hepatitis, SR? | 44 | 77.19 |
| Community mobilization | 48 | 84.21 | |
| Counseling | 43 | 75.44 | |
| Screening | 47 | 82.46 | |
| Therapeutic education | 36 | 63.16 | |
| Link to treatment | 38 | 66.67 | |
| Psychosocial support | 38 | 66.67 | |
| Demedicalized screening | 38 | 66.67 | |
| Self-test | 39 | 68.42 | |
| NTIC | 28 | 49.12 |
Resource Capacities of CBOs Providing HIV, TB, HVB, STI/SR Services to Key Populations in Cameroon
The availability of material resources depends on the service package offered by the respective OBCs. Regarding the availability of an adequate service provision system, 55.77% of OBCs had a general medicine consultation office, 36.54% had a pharmacy, 44.23% had a laboratory, 11.54% were able to perform minor surgery and 40.38% had an ARV dispensing office. Regarding the availability of functional IT equipment, we note that most (92.73%) of OBCs had the equipment with 77.19% having an internet connection. Regarding the regular inventory of equipment, 91.23% of OBCs reported conducting at least one annual inventory. In general, we noted that OBCs with DICs are better equipped than those without DICs.
Table 5: Availability of material resources in OBCs, Cameroon, June 2022.
| Variables | Terms and Conditions | Effective | % |
| Does OBC have an adequate service provision system? (Technical equipment and inputs) | Boxing or Consulting Room | ||
| Yes | 29 | 55.77 | |
| No | 23 | 44.23 | |
| Pharmacy | |||
| Yes | 19 | 36,538 | |
| No | 33 | 63,462 | |
| Laboratory | |||
| Yes | 23 | 44,231 | |
| No | 29 | 55,769 | |
| Archive | |||
| Yes | 49 | 94.23 | |
| No | 3 | 5.77 | |
| Surgery | |||
| Yes | 6 | 11.54 | |
| No | 46 | 88.46 | |
| Dispensing Office | |||
| Yes | 21 | 40.38 | |
| No | 31 | 59.62 | |
| Does the OBC/DIC have functional IT equipment (server, desktop, laptop, hard drive, printer)? | Yes | 51 | 92.73 |
| No | 4 | 7.27 | |
| Does the OBC/DIC have internet access? | Yes | 44 | 77.19 |
| No | 13 | 22.81 | |
| Does the OBC/DIC regularly carry out inventories of equipment and materials? | Yes | 52 | 91.23 |
| No | 5 | 8.77 | |
| Does the OBC/DIC have a policy for securing and controlling assets? | Guardian, | 23 | 57.5 |
| Secure door, | 39 | 97.5 | |
| Access filtering, | 19 | 47.5 | |
| A safe, | 11 | 27.5 | |
| Metal cabinets | 19 | 47.5 | |
Availability of HIV, TB, HVB, STI/SR services in OBC KPs.
Technical Capacity in HIV Service Offering
Risky behaviors and vulnerability of key populations lead to a disproportionate HIV infection rate among these groups in Cameroon. Some identity organizations conduct HIV-related activities thanks to grants from established projects. The field assessment of these CBOs revealed that they are equipped with reference documents such as: guidelines (61.4%), SOPs (57.89%), and national guides (54.39%) on HIV. It was noted that these documents are the most relevant to CBOs.
Regarding the service offer, we noted that pre-exposure prophylaxis and post-exposure prevention were available at 28.08% and 17.54%. Other prevention service offers were frequent at more than 50%. Therapeutic education was infrequent (5.26%); community distribution of ARVs was in 28.07%. Psychosocial support was present in 70.18% of OBCs. Prevention, care and management of co-infections and comorbidities (HIV/TB/hepatitis B) was present in 47.37% of OBCs. The minimum education service package for harm reduction (drugs) was present in 49.12% of OBCs.
Table 6: Situation of HIV supply to KP in OBCs, Cameroon, June 2022.
| HIV supply indicators | Staff | % |
| Availability of validated reference documents | ||
| SOP | 33 | 57.89 |
| Directive | 35 | 61.40 |
| National guides | 31 | 54.39 |
| The 10 WHO Clinical Standards | 10 | 17.54 |
| Biosafety document | 14 | 24.56 |
| OBC prevention service offering | ||
| Distribution of condoms and lubricants | 56 | 98.25 |
| Community awareness | 57 | 100.00 |
| Educational talk | 57 | 100.00 |
| HIV screening | 52 | 91.23 |
| PrEp | 16 | 28.07 |
| Post Exposure Prevention | 10 | 17.54 |
| Demedicalized screening | 36 | 63.16 |
| Self-test | 38 | 66.67 |
| Community dispensation of ARVs by OBC | ||
| Distribution of ARVs | 16 | 28.07 |
| ETP | 3 | 5.26 |
| Support group | 14 | 24.56 |
| Other | 26 | 45.61 |
| Offers a psychosocial support service | ||
| Yes | 40 | 70.18 |
| No | 15 | 26.32 |
| N / A | 2 | 3.51 |
| Prevention, care and management of co-infection and comorbidity (HIV/TB/hepatitis) | ||
| Yes | 27 | 47.37 |
| No | 25 | 43.86 |
| N / A | 5 | 8.77 |
| Availability of the minimum service package for harm reduction (drugs) in the OBC | ||
| Yes | 28 | 49.12 |
| No | 21 | 36.84 |
| N / A | 7 | 12.28 |
TB Service Offer
The assessment of OBCs offering TB services showed that regarding the availability of normative documents: SOPs 35.09%, guidelines 40.35% and national guides 35.09%. Regarding the service offer, the organization of awareness campaigns by the OBC was implemented by 63.79% of OBCs. The referral of index cases to guardian FOSA was implemented by 64.29% of OBCs, saliva sampling (53.57%), active case finding around contact cases by the OBC (48.21%) and the minimum service package for risk reduction in the OBC (37.50%).
Table 7: Availability of TB services in CBOs, Cameroon, 2022.
| Indicators | Staff | % |
| Availability of reference document validated in the OBC | ||
| SOP | 20 | 35.09 |
| Directive | 23 | 40.35 |
| National guides | 20 | 35.09 |
| Organization of awareness campaigns by the OBC | ||
| Yes | 37 | 63.79 |
| No | 8 | 13.79 |
| N/A | 13 | 22.41 |
| Reference of index cases to the guardian FOSAs | ||
| Yes | 36 | 64.29 |
| No | 8 | 14.29 |
| N/A | 12 | 21.43 |
| Saliva samples in the OBC | ||
| Yes | 30 | 53.57 |
| No | 14 | 25.00 |
| N/A | 12 | 21.43 |
| Active search for cases around contact cases by the OBC | ||
| Yes | 27 | 48.21 |
| No | 17 | 30.36 |
| N/A | 12 | 21.43 |
| Availability of the minimum service package for risk reduction in the OBC | ||
| Yes | 21 | 37.50 |
| No | 23 | 41.07 |
| N/A | 12 | 21.43 |
Technical Capacity in HVB Service Offer
The package of viral hepatitis B services offered remains facing many challenges. The assessment conducted among the OBC KPs noted that regarding the availability of a minimum service for the prevention of viral hepatitis in the OBC, 20% are involved in awareness activities on hepatitis B and vaccination. 26% are involved in the distribution of condoms. Regarding the provision of screening/vaccination services in the OBC, 44.44% do not offer these services. Similarly, 44.98% of OBCs do not have a minimum service package for risk reduction.
Table 8: Results of the evaluation of hepatitis B services offered to KP in OBC Cameroon, 2022.
| Indicators | Staff | % |
| Availability of reference document validated in the OBC | ||
| SOP | 11 | 20.37 |
| Guidelines | 9 | 16.67 |
| National guides | 8 | 14.81 |
| Availability of a minimum viral hepatitis prevention service in the OBC | ||
| Awareness raising on viral hepatitis and vaccination | 10 | 20 |
| Distribution of condoms | 13 | 26 |
| Screening | 2 | 4 |
| Offer of screening or vaccination services for hepatitis B/C in the OBC | ||
| Yes | 10 | 18.52 |
| No | 24 | 44.44 |
| N/A | 14 | 25.93 |
| Availability of a minimum service package for risk reduction | ||
| Yes | 12 | 24.49 |
| No | 24 | 48.98 |
| N/A | 13 | 26.53 |
Technical Capacity in IST/SR Service Offer
In the OBCs visited, sexual and reproductive health services are offered. Regarding the availability of reference documents, it was noted that: 37.04% (20/58) have SOPs, 33.33% (18/58) have guidelines and 35.19% (19/58) have national guides.
In terms of offering a minimum STI prevention service package, 87.04% of CBOs raise awareness about STIs and prevention methods, 88.89% distribute condoms, and 70.37% conduct STI screening. Regarding the offer of a minimum STI service package, 75.93% of CBOs provide syndromic and etiological management of STIs. Furthermore, regarding the offer of family planning services, 57.41% of CBOs distribute prevention materials. 46.30% provide pre- and post-counseling, and 24.07% provide contraceptive methods. Similarly, the offer of a minimum service package for reduction was available in 57.41% of CBOs.
Table 9: Results of the evaluation of STI and SR services offered to KP in OBCs, Cameroon, 2022.
| Indicators | Staff | % |
| Availability of reference document validated in the OBC | ||
| SOP | 20 | 37.04 |
| Directive | 18 | 33.33 |
| National guides | 19 | 35.19 |
| Offer of a minimum package of STI prevention services | ||
| Awareness of STIs and means of prevention | 47 | 87.04 |
| Distribution of condoms | 48 | 88.89 |
| Screening | 38 | 70.37 |
| Raising awareness of cervical cancer and anal cancer screening | 13 | 24.07 |
| Offer of a minimum service package for STI treatment | ||
| Treatment for OBCs with medical staff | 15 | 27.78 |
| Syndromic and etiological PEC | 41 | 75.93 |
| Offers family planning services through OBC | ||
| Distribution of prevention materials | 31 | 57.41 |
| Pre and post counseling | 25 | 46.30 |
| Provision of contraceptive methods | 13 | 24.07 |
| Pregnancy test | 7 | 12.96 |
| Availability of a minimum service package for risk reduction by the OBC | ||
| Yes | 31 | 57.41 |
| No | 15 | 27.78 |
| N/A | 8 | 14.81 |
Overall Technical Capacities of OBCS to provide HIV, TB, HVB, STI/SR services to Key Populations
Generally speaking, the “Overall technical capacity of each OBC KPs” was determined based on the weighting of technical capacities in human and material resources and in the provision of HIV, TB, HVB, STI/SR services then classified as weak, acceptable, good and very good. Of the 58 OBCs KPs assessed 27 (46.55%) had low overall technical capacity to provide HIV, TB, HVB, STI/SR health services to Key Populations 22 (37.93%) had acceptable overall technical capacity and (15.51%) good overall technical capacity. Note that no OBC KP had very good capacity.
Overall technical capacities of OBCs KPs to provide HIV health services
Regarding the overall technical capacity of CBOs to provide HIV services, statistical analyses showed that 11.9% (7/58) of CBOs had low capacity, 33.9% (20/58) acceptable and 47.7% good. Furthermore, 6.8% (4/58) of CBOs KPs had very good overall technical capacity to provide HIV service. In addition, serious gaps in human and material resources were observed, with 47.5% (28/58) of OBC KPs OBCs having low technical capacity and facing difficulties in addressing all components of service provision according to national health policies (See Table 10).
Table 10: Technical capacity of CBOs to provide HIV services in Cameroon in June 2022.
| Variables | Technical Capacity in HIV Service Provision | Material Resources | Human Resources | |||
| Technical Capacity | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) |
| Weak | 7 | 11.9 | 28 | 47.5 | 28 | 47.5 |
| Acceptable | 20 | 33.9 | 11 | 18.6 | 11 | 18.6 |
| Good | 28 | 47.5 | 19 | 32.2 | 19 | 32.2 |
| Very good | 4 | 6.8 | 1 | 1.73 | 1 | 1.73 |
| Significance (p) | 0.00 | 0.00 | ||||
Overall technical capacities of OBCs KPs to provide TB health services
The statistical data revealed that in terms of TB service provision, 63.79% (37/58) of OBC KPs had low technical capacity, 32.76% (19/58) had acceptable technical capacity. Furthermore, no OBC had good technical capacity and 3.45% (2/58) had very good capacity. Similarly, it appears that (18/58) OBC or 69.23% do not have adequate human resources and 87.50% (21/58) do not have material resources (See table 11).
Table 11: Technical capacity of OBCs to offer TB services in Cameroon in June 2022.
| Variables | Technical capacity in TB service Offering | Material Resources | Human Resources | |||
| Technical Capacity | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) |
| Weak | 37 | 63.79 | 21 | 87.50 | 18 | 69.23 |
| Acceptable | 19 | 32.76 | 3 | 12.50 | 6 | 23.04 |
| Good | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| Very good | 2 | 3.45 | 0 | 0.00 | 2 | 7.69 |
| Significance (p) | 0.97 | 0.00 | ||||
Technical capacities of OBCs KPs to provide HVB health services
The service provision in viral hepatitis B (HVB) showed that (51/58) of the OBC KPs or 87.93% of the OBCs had low technical capacity, (5/58) or 8.62 percentage acceptable technical capacity and (2/58) or 03.44% good capacity. However, no OBC KPs had very good technical capacity. Furthermore, it was noted that (25/58) of the OBC KPs or 92.59% do not have material resource capacity and (19/58) OBC in human resources. The minimum service package in the OBC KPs is almost non-existent (see table 12).
Table 12: Technical capabilities of OBCs to offer HVB services at KPs, Cameroon June 2022.
| Variables | Technical Capacity in HVB Service Offering | Material Resources | Human Resources | |||
| Technical Capacity | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) |
| Weak | 51 | 87.93 | 25 | 92.59 | 19 | 100.00 |
| Acceptable | 5 | 8.62 | 0 | 0.00 | 0 | 0.00 |
| Good | 2 | 3.44 | 2 | 7.41 | 0 | 0.00 |
| Very good | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| Significance (p) | 0.013 | 0.00 | ||||
Technical capacities of OBCs KPs to provide STI/SR health services
The overall technical capacity of OBC KPs related to providing reproductive health and sexually transmitted infections services showed that (44/58) or 75.86% of OBC KPs had low technical capacity, (14/58) or 24.14% had acceptable technical capacity. However, no OBC had good or very good technical capacity. Furthermore, there was a lack of material and human resources in these OBC KPs with low capacities of 92.59% (25/58) and (19/58) OBCs in human resources respectively. (See table 13).
Table 13: Technical capacities of OBCs to offer IST/SR services in Cameroon in June 2022.
| Variables | Technical capacity in IST/SR service provision | Material resources | Human Resources | |||
| Technical Capacity | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) | Staff (n) | Frequency (%) |
| Weak | 44 | 75.86 | 25 | 92.59 | 19 | 90.48 |
| Acceptable | 14 | 24.14 | 2 | 7.41 | 2 | 9.52 |
| Good | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| Very good | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| Significance (p) | 0.004 | 0.011 | ||||
Table 14: Profiles of OBCs assessed in June 2022.
| Assessment of capacities according to OBC types | Ability | ||||
| Weak (%) | Acceptable (%) | Good (%) | Very good (%) | total (%) | |
| Identity | 10(37.0) | 12(44.4) | 5(18.5) | 0(00) | 27(46.55) |
| Non-Identity | 17(54.8) | 10(32.3) | 4(12.9) | 0(00) | 31(53.44) |
| Total | 27(4655) | 22(3793) | 9(1551) | 0(00) | 58(100) |
Discussion
KPs service package offer made it possible to identify gaps in order to see which priority areas require action to make this offer more effective and to effectively delegate tasks to the OBCs.
In terms of HIV service provision, most of the OBC KPs had acceptable to very good technical capacities. It should be noted that the provision of the minimum service package in these OBC KPs is effective. However, as for the optimal service package including new strategies such as Prep, demedicalized screening (DD), self- testing (AT) and community dispensing of ARVs to achieve the three 95 targets, are not implemented in the OBC KPs. Data collected in the field showed that very few OBCs, 5.26 % (3/58), implemented ETP, 28.07% (16/58) ARV dispensing and Prep and 17.54% (10/58) Prep. This can be explained by the observed lack of material and human resources. This state of affairs is not in line with the ten priority clinical care standards for key populations, the task delegation guide for HIV/AIDS care and the sexual health provision framework for key populations.
The overall performance of the technical capacities of the TB service provision was weak and they did not have adequate human or material resources. The minimum service package existed in a majority of CBOs with acceptable capacities. Community activities such as awareness campaigns, case referral and saliva sampling constituted the minimum service package in the ten priority clinical care standards and the sexual health service offering framework for key populations was effective [8]. Some CBOs offered less than the minimum optimal service package. The GAPs observed in the implementation of community activities related to TB require optimization of the TB service offering in CBOs.
The provision of services for viral hepatitis B (HVB) in accordance with the ten priority clinical care standards and the benchmark for sexual health provision for key copulations [8]. The results of the assessment show that the majority of CBOs have weak technical capacities in terms of viral hepatitis B (HVB) service provision. Furthermore, they do not have the capacity in material and human resources. The minimum service package in CBOs is almost non-existent. Other activities such as screening, vaccination and referral constituting the optimal service package are not implemented. It is clear that viral hepatitis B, which is one of the major HIV co-infections among key populations, is not implemented in CBOs, hence the need to strengthen the technical capacities of CBOs on the complete packages of viral hepatitis services.
The technical capacity in the provision of reproductive health and sexually transmitted infections services was acceptable in the CBOs with insufficient material and human resources. Awareness of STIs, means of prevention and syndromic and ethological management of STIs were effective in the CBOs. Other priority services constituting the optimal service package such as proctological care, gynecologists, family planning, referral for post-abortion care, pregnancy monitoring and obstetric care and complex cases of gynecological monitoring as well as the comprehensive management of GBV and psychosocial support remain poorly implemented in the CBOs in accordance with the framework for the provision of sexual health to key populations. Although the service provision exists, strengthening the technical capacities of the CBOs is necessary.
Summary of Identified Needs
At the end of the analysis of the results obtained and taking into account the task delegation guide, we note that the OBCs have technical capacities for the implementation of certain tasks “Not Applicable” at their level in the 2013 guide. However, it is necessary to proceed with a delegation of the identified tasks and to strengthen the capacities in this area. Scaling up requires a formal delegation of tasks as well as capacity building for structures with weak or acceptable capacities.
In addition to the services contained in the DDT guide, the evaluation found that other services are implemented in the OBCs and can therefore be taken into account in updating the guide and formally delegated to the OBCs thereafter.
Conclusion
The assessment of the technical capacities of the 58 OBC KPs to provide HIV, HVB, TB, STI and SR health services made it possible to classify them into three categories:
- OBC with low technical capacity.
- OBC with acceptable and good technical capacity.
- OBC with very good technical capacity.
Regarding the last two categories and in comparison, with the task delegation guide, the results obtained showed that these offered more than the minimum package of services dedicated to them. However, the surplus of services offered is not taken into account in the (normative) task delegation guide; hence the need to update said guide. This update will make it possible to supervise the implementation of task delegation.
Also, provide a capacity building plan for CBOs with low technical capacity. This update could contribute to strengthening policies, guidelines and guides for the management of HIV, TB, hepatitis B and SR in Cameroon on the eve of achieving the 95-95-95 objectives.
References
- Ministry of Public Health Cameroon. (2020). CNLS Annual Report 2020.
Publisher | Google Scholor - The DHS Program. (2018). Cameroon 2018 Demographic and Health Survey.
Publisher | Google Scholor - World Health Organization, Unicef. (1979). Report of the International Conference on Primary Health Care Alma-Ata.
Publisher | Google Scholor - Ministry of Public Health Cameroon. (2022). National Strategic Plan to Combat HIV/AIDS and STIs in Cameroon 2021-2023.
Publisher | Google Scholor - Ministry of Public Health, Technical Group of the National Committee for the Fight Against AIDS. (2021). Annual Activity Report of the National Committee for the Fight Against AIDS in Cameroon.
Publisher | Google Scholor - UNAIDS Report: Progress Against HIV Threatened. (2022). vih.org.
Publisher | Google Scholor - Dakar Call to Reinvent the Response to the HIV Pandemic: A Renewed Commitment to End AIDS in West and Central Africa. UNAIDS. (2021).
Publisher | Google Scholor - USAID, PEPFAR. 10 Priority Clinical Care Standards for Key Populations.
Publisher | Google Scholor























