

Case Report
Sigmoid Volvulus with Perforation Peritonitis in A Patient with Chronic Traumatic Paraplegia Managed by Emergency Hartmann Procedure: A Case Report
General and Laparoscopic Surgeon, Department of Surgery, Military Hospital Khadki, Pune, Maharashtra, India.
*Corresponding Author: Gurmeet Singh Sarla,General and Laparoscopic Surgeon, Department of Surgery, Military Hospital Khadki, Pune, Maharashtra, India.
Citation: Sarla GS, Gurav O. (2026). Sigmoid Volvulus with Perforation Peritonitis in A Patient with Chronic Traumatic Paraplegia Managed by Emergency Hartmann Procedure: A Case Report, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 7(2):1-4. DOI: 10.59657/2997-6103.brs.26.143
Copyright: © 2026 Gurmeet Singh Sarla, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 02, 2026 | Accepted: July 02, 2026 | Published: July 10, 2026
Abstract
Background: Sigmoid volvulus is a common cause of large bowel obstruction and may progress to bowel ischemia, gangrene, and perforation if diagnosis and treatment are delayed. Patients with chronic neurological disorders, including paraplegia, are predisposed to colonic dysmotility and volvulus. We report a case of sigmoid volvulus with perforation peritonitis in a patient with longstanding traumatic paraplegia managed successfully by emergency sigmoid colectomy and Hartmann procedure.
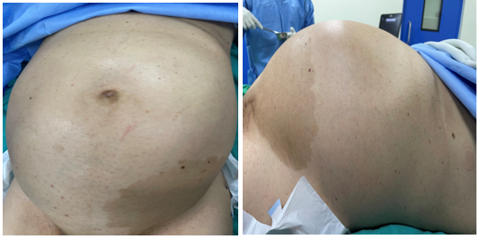
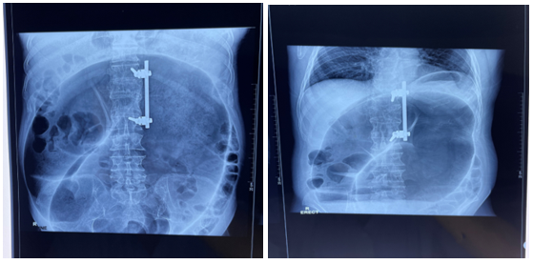
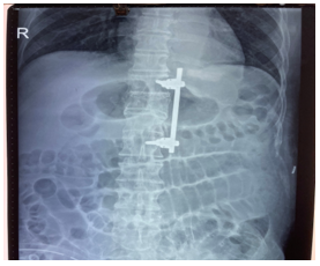
Case Presentation: A 48-year-old male with traumatic paraplegia since 2002 presented with progressive abdominal distension and obstipation for three days. Clinical examination revealed a markedly distended abdomen with absent bowel sounds. Laboratory investigations showed leukocytosis (17,900/mm³). Plain abdominal radiograph demonstrated a classic coffee-bean sign, while ultrasonography with non-contrast computed tomography correlation revealed a markedly dilated sigmoid colon with a whirl sign suggestive of sigmoid volvulus. Following resuscitation, emergency exploratory laparotomy revealed a grossly distended, dusky, rotated sigmoid colon with a 2 × 1 cm perforation on the antimesenteric border and purulent peritoneal contamination. Sigmoid colectomy with Hartmann procedure was performed. The postoperative period was complicated by transient paralytic ileus and superficial surgical site infection, both managed successfully. The patient was discharged in stable condition on postoperative day 20.
Discussion: Chronic paraplegia predisposes patients to altered bowel motility and chronic constipation, recognized risk factors for sigmoid volvulus. Imaging findings such as the coffee-bean sign and whirl sign facilitate prompt diagnosis. In the presence of perforation and non-viable bowel, resection with Hartmann procedure remains a safe and effective surgical option. Early recognition and timely surgical intervention are critical in reducing morbidity and mortality.
Conclusion: Sigmoid volvulus should be considered in paraplegic patients presenting with abdominal distension and obstipation. Prompt diagnosis and emergency surgical management are essential when complications such as ischemia or perforation develop.
Keywords: sigmoid volvulus; perforation peritonitis; hartmann procedure; traumatic paraplegia; large bowel obstruction; emergency surgery
Introduction
Sigmoid volvulus results from twisting of the sigmoid colon around its mesenteric axis, leading to luminal obstruction and vascular compromise [1]. It accounts for a significant proportion of large bowel obstruction worldwide, particularly in the so-called “volvulus belt”, an endemic area that includes Africa, South America, Russia, Eastern Europe, the Middle East, India and Brazil, colonic volvulus represents 13 to 42% of all intestinal obstructions [2]. Delayed diagnosis can result in bowel ischemia, gangrene, perforation, and generalized peritonitis. Neurological disorders, including spinal cord injuries, contribute to chronic bowel dysmotility and constipation, increasing the risk of volvulus formation [3]. We present a rare case of perforated sigmoid volvulus in a patient with chronic traumatic paraplegia managed by emergency sigmoid colectomy with Hartmann procedure.
Case Presentation
A 48-year-old male with a history of traumatic paraplegia following spinal injury in 2002 presented with abdominal distension and obstipation of three days duration. The abdominal distension was insidious in onset and progressively increased over time. There was no history of vomiting, fever, or urinary complaints. The patient had previously undergone surgery for left inguinal hernia in 1996.
On examination, the patient was conscious and oriented. The abdomen was markedly distended with a girth of 102 cm. Bowel sounds were absent. There was no guarding or rigidity. Digital rectal examination revealed an empty, roomy rectum.
Laboratory investigations revealed hemoglobin of 14.6 g/dL, total leukocyte count of 17,900/mm³ with neutrophilic predominance, and normal renal function parameters. Plain abdominal radiography demonstrated a massively dilated loop of colon with a characteristic coffee-bean appearance suggestive of sigmoid volvulus. Ultrasonography with NCCT correlation revealed disproportionate dilatation of the sigmoid loop forming an inverted U-shaped configuration extending into the upper abdomen. Twisting of the sigmoid mesentery and mesenteric vessels produced a distinct whirl sign [4], confirming the diagnosis.
The patient was admitted to the intensive care unit and resuscitated with intravenous fluids. Nasogastric decompression and urinary catheterization were performed. Broad-spectrum intravenous antibiotics were administered, and emergency exploratory laparotomy was planned.
Surgical Findings and Management
Emergency laparotomy was performed under general anesthesia through a vertical midline incision. Upon entering the peritoneal cavity, a gush of air with feculent odor was encountered. The sigmoid colon was found to be grossly distended, dusky, and rotated around its mesenteric axis. A perforation measuring approximately 2×1 cm was identified on the antimesenteric border. The sigmoid mesentery was long and redundant.
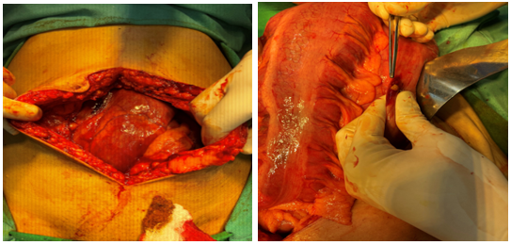
Purulent peritoneal fluid with minimal fecal contamination was present. Thorough peritoneal lavage was performed using approximately 4-5 liters of warm normal saline. The sigmoid colon was divided at the rectosigmoid junction, and approximately 40 cm of non-viable sigmoid and descending colon was resected. The rectal stump was closed in two layers.
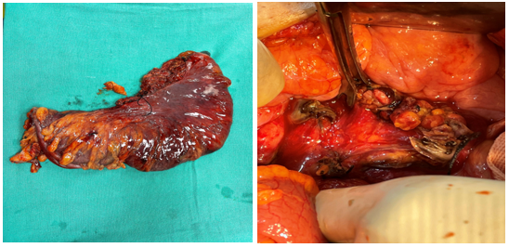
An end colostomy was fashioned from the mobilized descending colon. Two intra-abdominal drains were placed, and the abdomen was closed in layers.

Postoperative Course
The patient was managed in the intensive care unit with intravenous antibiotics, supportive therapy, and wound care. On postoperative day 2, laboratory investigations demonstrated hemoglobin of 10 g/dL, serum albumin of 2.1 g/dL, and hypokalemia (3.0mEq/L). Reduced urine output necessitated consultation with the medical team, following which albumin infusion, potassium replacement, and diuretic therapy were administered. Chest physiotherapy, incentive spirometry, and wheelchair mobilization were initiated early. The colostomy became functional, and gradual clinical improvement was observed. On postoperative day 7, the patient developed paralytic ileus. Abdominal radiography demonstrated dilated jejunal loops with a concertina appearance. Conservative management resulted in complete resolution.
A superficial surgical site infection subsequently developed and was treated successfully with daily wound care and secondary suturing on postoperative day 10. The patient was discharged on postoperative day 20 in stable condition. He was tolerating a full oral diet, the colostomy was healthy and functional, and the surgical wound had healed satisfactorily. Comprehensive stoma-care education was provided to the patient and family members before discharge.
Discussion
Sigmoid volvulus occurs due to twisting of a redundant sigmoid colon around a narrow mesenteric base. Chronic constipation, neurological disorders, prolonged immobility, and megacolon are recognized predisposing factors. Patients with spinal cord injury frequently develop neurogenic bowel dysfunction, leading to chronic constipation and colonic elongation, which increase susceptibility to volvulus.
The classic radiological feature on plain radiography is the coffee-bean sign, while computed tomography often demonstrates the whirl sign, indicating torsion of the mesentery. These findings were clearly demonstrated in the present case and facilitated timely diagnosis.
Management depends on bowel viability and the presence of complications. Endoscopic decompression may be considered in uncomplicated cases; however, gangrene, perforation, and generalized peritonitis mandate emergency surgery. Hartmann procedure remains a preferred option in unstable patients or when significant contamination is present, as it avoids the risks associated with primary anastomosis in a hostile abdomen.
Our patient had multiple risk factors including chronic paraplegia and a redundant sigmoid colon. The presence of perforation and non-viable bowel necessitated definitive surgical resection. Despite postoperative complications including paralytic ileus [5] and surgical site infection, the patient recovered satisfactorily with multidisciplinary management.
Conclusion
Sigmoid volvulus should be considered in elderly patients with chronic paraplegia presenting with abdominal distension and obstipation [6]. Early imaging facilitates prompt diagnosis, while emergency surgery remains the cornerstone of management in cases complicated by ischemia or perforation.
A staged approach with proximal diversion during initial surgery minimizes anastomotic complications and ensures safe restoration of bowel continuity after recovery [7]. Hartmann procedure provides a safe and effective treatment option in the setting of perforation peritonitis [8].
Statement of Informed Consent
Informed consent was obtained from the patient that was presented in the case report.
References
- Lal, S. K., Morgenstern, R., Vinjirayer, E. P., Matin, A. (2006). Sigmoid Volvulus an Update. Gastrointestinal Endoscopy Clinics, 16(1):175-187.
Publisher | Google Scholor - Perrot, L., Fohlen, A., Alves, A., Lubrano, J. (2016). Management of The Colonic Volvulus in 2016. Journal of Visceral Surgery, 153(3):183-192.
Publisher | Google Scholor - Atamanalp, S. S. (2013). Sigmoid Volvulus: Diagnosis in 938 Patients Over 45.5 Years. Techniques in Coloproctology, 17(4):419-424.
Publisher | Google Scholor - Duda, J. B., Bhatt, S., Dogra, V. S. (2008). Utility of CT Whirl Sign in Guiding Management of Small-Bowel Obstruction. American Journal of Roentgenology, 191(3):743-747.
Publisher | Google Scholor - Schuster, T. G., Montie, J. E. (2002). Postoperative Ileus After Abdominal Surgery. Urology, 59(4):465-471.
Publisher | Google Scholor - Perrone, G., Giuffrida, M., Papagni, V., Pattonieri, V., Tarasconi, A., et al. (2021). Management of Acute Large Bowel Obstruction in Elderly Patients. In Emergency General Surgery in Geriatrics (pp. 349-360). Cham: Springer International Publishing.
Publisher | Google Scholor - Wyke, M. N. Z., Kyaw Ye Naung Htun, Aung Ko Ko Linn, Thant Lwyn San, Khin Aung Htun. (2026). Sigmoid Volvulus Presenting as Large Bowel Obstruction in an Elderly Patient with Diabetes and Hypertension: A Case Report Emphasizing Timely Surgical Management. International Journal of Medical Science and Clinical Research Studies, 6(01):203-208.
Publisher | Google Scholor - Barbieux, J., Plumereau, F., Hamy, A. (2016). Current Indications for The Hartmann Procedure. Journal of Visceral Surgery, 153(1):31-38.
Publisher | Google Scholor























