

Case Report
Sebaceoma of the Scalp Mimicking Squamous Cell Carcinoma: Diagnostic Challenge and Immunohistochemical Confirmation
1 Third-year Dermatology Resident, University of Carabobo. Physician attached to the Dermatology service, Dr. Enrique Tejera Hospital City, Valencia City, Venezuela.
2 Internal Medicine Physician-Dermatologist, Head of the Dermatology Department at the Dr. Enrique Tejera University Hospital. Academic Coordinator of the Dermatology Postgraduate Program at the University of Carabobo. Valencia, Venezuela.
*Corresponding Author: González G, Dayangel ,Third-year Dermatology Resident, University of Carabobo.
Citation: González G, Lina A, Sandra V (2026). Sebaceoma Of the Scalp Mimicking Squamous Cell Carcinoma: Diagnostic Challenge and Immunohistochemical Confirmation. International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 6(2):1-4. DOI: 10.59657/2837-8172.brs.26.090
Copyright: © 2026 González G, Dayangel, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 07, 2026 | Accepted: May 21, 2026 | Published: June 04, 2026
Abstract
We present the case of a 46-year-old woman with an erythematous nodular lesion in the occipital region that had been present for four months. After initial suspicion of malignancy, excisional biopsy and immunohistochemistry confirmed the definitive diagnosis of sebaceoma, a rare benign sebaceous tumor. The report highlights the difficulty in differentiating this pathology from more aggressive carcinomas due to its clinical appearance and histological complexity. It concludes that the use of specific markers is vital to ensure accurate diagnosis, avoid excessive treatment, and monitor for potential systemic risks.
Keywords: sebaceoma; benign sebaceous tumor; immunohistochemistry
Introduction
This is a 46- year-old female patient, skin phototype IV/VI according to the Fitzpatrick scale, presenting with a dermatosis located in the occipital region, characterized by a 3x2.5cm diameter neoformation with well-defined, regular borders, an erythematous color with a depressed center, and the presence of a few yellow crusts, of 4 months' duration, without associated symptoms (Figure 1). Dermatoscopy: erythematous base, yellowish areas, yellow crust, arborized and glomerular vessels in the periphery. (Figure 2). The following presumptive diagnoses are considered: 1. Squamous cell carcinoma. 2. Sebaceous carcinoma. 3. Sebaceoma.
The following work plan is carried out
Procedure: excisional biopsy with oncological margins, study by histopathology and immunohistochemistry and complementary studies: CT scan of the skull, neck, thorax and abdomen, which revealed an incidental finding of benign thyroid nodules, without evidence of metastasis.
Histopathology: At 40x magnification, a proliferation of atypical epithelial cells is observed in the dermis. These cells are ovoid, polygonal, and have clear cytoplasm in some areas. In other areas, eosinophilic cytoplasm with keratinization is seen, along with irregular calcifications. The described cell proliferation shows a mitotic index of 0.4 mitoses/field. These characteristics are compatible with sebaceous carcinoma.
In the immunohistochemistry: The antigens investigated are listed below: Cytokeratin 7: positive in numerous neoplastic cells, with a cytoplasmic pattern. Cytokeratin 34BE12: positive in neoplastic cells with a cytoplasmic pattern. p63 protein: positive in numerous neoplastic cells, with a nuclear pattern. Epithelial membrane antigen (EMA): positive in neoplastic cells, with both membranous and cytoplasmic patterns. The dermal lesion is nodular and composed of a mixture of basaloid cells and mature sebaceous cells. The tumor cells are arranged in solid nests of varying sizes, within which occasional ductal structures and areas of squamous metaplasia are identified. No nuclear atypia, mitosis, or necrosis is observed. The findings are consistent with a sebaceoma.

Figure 1: Dermatosis located in the occipital region, characterized by a neoformation of 3x2.5cm in diameter, regular well-defined borders, erythematous color with a depressed center and the presence of few yellow crusts.
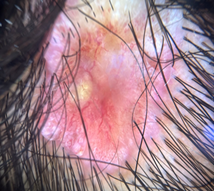
Figure 2: Dermatoscopy: erythematous base, yellowish areas, yellow crust, arborizing and glomerular vessels in the periphery.
Discussion
Sebaceoma is a rare, nodular skin tumor with yellowish areas on its surface, most commonly found on the face and neck [1]. It represents an incidence that ranges between 0.05 % and 0.7 % of all Skin tumors. Most of the patients are found among the sixth and the ninth decade of life. Although these tumors also can be observed in adults younger [2].
This unusual benign sebaceous neoplasm, described by Troy and Ackerman in 1984, was called sebaceous epithelioma, generating confusion regarding its tumor biology, since histopathologically it does not present sufficient differentiation to be called a sebaceous adenoma and is not as undifferentiated as sebaceous carcinoma or basal cell carcinoma with sebaceous differentiation [3].
The sebaceoma it’s an adnexal epithelioma with differentiation of sebaceous glands. Clinically, the Sebaceoma appears as rounded, raised papulonodules and yellowish. The size of the tumor usually approximately 1 cm, although have described injuries larger [3].
Due to its rarity and to broad spectrum of injuries cutaneous, the sebaceoma consider a difficult injury to diagnose [2].
When the diagnosis is uncertain, it must perform a biopsy followed by an analysis histopathological for differentiate carefully the sebaceoma of other tumors. Histopathologically, the sebaceoma sample a wide range of patterns, from the observed in its sebaceous adenoma up to features that can be difficult to distinguish of carcinoma of sebaceous glands [2].
Histologically, the sebaceoma is a tumor dermal with or without connection with the epidermis. Its appearance histological of tumor is benign and includes multiple nests of basaloid cells with less of 50 % of Mature sebocytes. The absence of palisade peripheral and clefts between the nests and the stroma lo distinguishes from basal cell carcinoma with sebaceous differentiation.
Immunohistochemistry (IHC) positive diffuse of CK in the cells epithelial, and a positivity from EMA with an irregular pattern [4].
The use of immunohistochemistry has become established as an indispensable tool for differentiating these entities, avoiding unnecessary aggressive treatments and providing diagnostic accuracy in oncological dermatology.
A sebaceoma is a rare tumor of the scalp. benign neoplasm distinctive of adnexal epithelium with differentiation towards sebaceous structures; it presents like a nodular lesion circumscribed or small (5-30 mm), solitary nodules flesh-colored or yellowish, but sometimes they are multiple, particularly in it MuirTorre syndrome, how rare once it diagnoses earlier of a Histological examination [2,5].
Sebaceoma presents a diagnostic challenge, as it is diagnosed mistakenly as sebaceous adenoma, which is more organized and usually has a component less prominent basaloid [5]. The differentiation of sebaceomas of carcinoma sebaceous in a case typical based on growth infiltrative and atypia Cytological analysis of the latter. The sebaceoma must be differentiated of trichoblastoma with sebaceous differentiation, which invariably shows focal differentiation of hair follicle and bodies papillary mesenchymals [6].
The sebaceoma must be distinguished of the adenoma sebaceous, which typically presents an architecture lobular and has less of 50
Conclusion
This case underscores the need to consider sebaceous tumors in the differential diagnosis of nodular scalp lesions, especially when they mimic more common malignancies. Immunohistochemistry is confirmed as an essential tool for establishing a definitive diagnosis and avoiding excessive or inappropriate treatments. Furthermore, excisional biopsy with oncological margins is a safe and effective initial approach for suspicious lesions. Accurate identification of these neoplasms not only ensures appropriate clinical management and avoids unnecessary interventions, but also provides valuable knowledge about the atypical presentation of sebaceous tumors, enriching dermatological practice and strengthening decision-making in complex scenarios.
Name of the institution where the work was carried out: Dermatology service of the Dr. “Enrique Tejera” hospital city, Valencia - Carabobo State, Venezuela.
Summary: We present the case of a 46-year-old woman with an erythematous nodular lesion in the occipital region that had been present for four months. After initial suspicion of malignancy, excisional biopsy and immunohistochemistry confirmed the definitive diagnosis of sebaceoma, a rare benign sebaceous tumor. The report highlights the difficulty in differentiating this pathology from more aggressive carcinomas due to its clinical appearance and histological complexity. It concludes that the use of specific markers is vital to ensure an accurate diagnosis, avoid excessive treatment, and monitor for potential systemic risks.
References
- Leal Vásquez RA, Maza de Franco A, Leal Calderón CM (2020). Sebaceoma: presentation of a case and review of the medical literature. Rev Med Derm Lat Am.,58(2): 123-8.
Publisher | Google Scholor - Zlatarova Z, Chivchibashi Pavlova D, Dzhenkov D (2023). Sebaceoma of the eyelid originating from a meibomian gland: a rare case and review of the literature. Int Ophthalmol.,43(2):145 - 9.
Publisher | Google Scholor - Vargas P, Orlandi D, Giacaman P, Figueroa A (2020). Sebaceoma: dermatoscopic findings in two cases. Rev Chil Dermatol.,36(1):22-4.
Publisher | Google Scholor - Yaghoobi R, Pazyar N (2022). Sebaceoma in a patient with a history of kidney transplantation. Indian J Dermatol.,67(2):209.
Publisher | Google Scholor - Lee DW, Kwak SH, Kim JH, Byeon JY, Lee HJ, et al., (2021). Sebaceous carcinoma arising from a sebaceoma . Arch Plast Surg.,48(3):250 - 254.
Publisher | Google Scholor - Han S, Cho SJ, Kang SJ, Kim JH, Kim CW (2023). Borderline malignant sebaceoma of the auricle: a case report. Indian J Otolaryngol Head Neck Surg.,75(1 ): eXXX - eXXX .
Publisher | Google Scholor























