

Case Report
Resection of a Sternal Chondrosarcoma and Chest Wall Reconstruction, And Management Challenges-Case Report
- Abhilash T *
Deenanath Mangeshkar Hospital and Research Center, Pune, India.
*Corresponding Author: Abhilash T. Deenanath Mangeshkar Hospital and Research Center, Pune, India.
Citation: Abhilash T. (2026). Resection of a Sternal Chondrosarcoma and Chest Wall Reconstruction, And Management Challenges-Case Report. Journal of Cancer Management and Research, BioRes Scientia publishers. 4(1):1-7. DOI: 10.59657/2996-4563.brs.26.026
Copyright: © 2026 Abhilash T, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 09, 2026 | Accepted: June 23, 2026 | Published: June 30, 2026
Abstract
Chondrosarcomas are the second most common malignant bone tumors. But it is uncommon for chondrosarcomas to occur within the sternum, especially giant sternal tumors occurring in advanced age. In this case, this study is set out to document the clinical features, pre-surgical planning and surgery methods, and post-operative care of a giant sternal chondrosarcoma in an advanced age patient. An 81-year-old male presented himself with sternum pain and mass. Based on the CT scans done, it was found that there was a destructive lesion in the xiphoid process which involved extra-thoracic and intrathoracic components. Biopsy done was consistent with grade I chondrosarcoma with no metastatic spread. As such, surgery was conducted on the patient due to the non-existence of metastasis. Thereafter, wide excision of the tumor was conducted. Given that the patient was poor, reconstruction of the large defect caused by removal of the tumor was done using a composite surgical mesh and bilateral pectoral myocutaneous flaps. Postoperative outcome was satisfactory and the patient was discharged home free from complications 10days after operation. Using our reconstructive techniques could be a safe, reliable and affordable surgery procedure. It may be an appropriate option for similar cases.
Keywords: primary bone cancer; chondrosarcoma; metastasis; sternum
Introduction
Chondrosarcoma is the second most frequent type of malignant primary bone cancer. The composition of this cancer is the malignant chondrocytes. Occurs in older adults (40 to 75 years old, and mild male preponderance). Most commonly affected sites include the pelvis (25% of all cases), proximal femur, distal femur, proximal humerus, distal tibia, and scapula. Rare involvement of the spine or craniofacial bones. Most often located in the metaphysis or diaphysis, rarely in the epiphysis [1]. The majority of chondrosarcomas are sporadic (primary chondrosarcomas), but secondary chondrosarcomas can arise from osteochondromas or enchondromas. Diagnosis is achieved through a combination of clinical features and imaging techniques (X-rays, CT, MRI) associated with lesional biopsy. Surgical resection is the typical treatment option for most conventional chondrosarcomas, which are not sensitive to chemotherapy or radiotherapy [2,3]. The key principles for chest wall reconstruction include the removal of dead space, maintaining chest wall integrity, preserving pulmonary mechanics, protecting intrathoracic organs, providing sufficient soft tissue coverage, minimizing deformities. There are many artificial meshes, such as polypropylene, polyester, and PTFE, that are used due to their convenience, flexibility, and customization according to the needs of the patient, in line with the ideal characteristics of prosthetic materials (rigidness, non-toxicity, malleability, and radiolucency) [4].
This article will present a very unusual case of chondrosarcoma of the sternum in an elderly man and chest wall reconstruction using a composite surgical mesh with bilateral pectoralis myocutaneous flaps. In this case, there were some special considerations made during the planning and management of perioperative processes. Moreover, the surgical incision is large, and effective drainage is required to avoid infection and necrosis of the flaps. Improvements have been made in these areas. An understanding of the approach to treat sternal chondrosarcoma and reconstructive surgery of the chest wall, especially its perioperative management.
Case Report
An 81-year-old man came to the OPD with an increasing lump on his chest, which had occurred one year ago. He was previously diagnosed with diabetes mellitus. His previous history revealed that he had deep vein thrombosis in 2013, followed by warfarin therapy for five to six months, then single antiplatelet therapy. On examination, he had a hard, fixed lump measuring 10 cm x 9 cm. The upper border was located 4 cm from the sternal angle, while the lower border was 1 cm below the lower costal margin. The left border was 1 cm from the midclavicular line, and the right border was 1 cm medial to the midclavicular line.

Figure 1: Photography of the patient's clinical presentation.
The above further in-depth study was performed using a CT thorax scan and was found that there was a destruction of the xiphoid process with large lobulated lesion having a size of 9.6x8.1x8.3cm. The subcutaneous portion of the lesion was identified causing a bulge under the overlying skin. The deep bulge associated with the lesion was seen in the anterior mediastinum which in turn caused a depression on the pericardium. There is an involvement of the sterno-costal and Morgagni foramina with some extension noted in the proximal part of the rectus abdominis on both sides. There was also noted some involvement of the anterior chest wall muscles in this region.
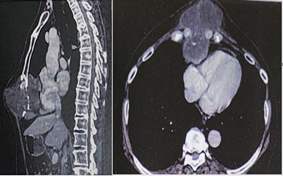
Figure 2: CT scan slice showing the mass at the level of the xiphisternum.
PET Scan revealed weakly metabolic lytic lesion in xiphisternum, anterior extra thoracic component measures 56 X 82 mm (SUV-2.96), intrathoracic component 50 X 46 mm (SUV-1.42) abutting pericardium. Calcific nodule in superior segment of left lung lower lobe 4mm.
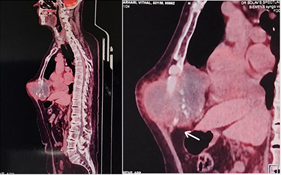
Figure 3: PET CT scan slice showing the metabolically active mass at the level of the xiphisternum.
A core biopsy of the mass confirmed a diagnosis of low-grade chondrosarcoma. In the laboratory workup, biological analyses were conducted, including a complete blood count, biochemical profile and coagulation panel. Interestingly, all these results were within normal limits, showing no significant deviations from the expected values. A doppler lower limb was conducted in view of the past history of deep vein thrombosis. Revealed thrombosis in left superficial femoral vein and preoperative injection clexane started.
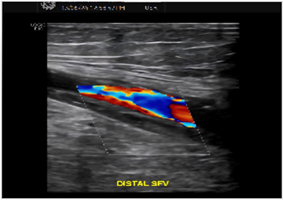
Figure 4: Doppler lower limb showing superficial femoral vein thrombosis
Subsequently, multidisciplinary treatment (MDT) was administered by the Departments of Oncosurgery, Anesthesia, General medicine and Cardiology. Due to the patient’s advanced age, previous deep vein thrombosis history, giant tumor, severe surgical trauma, and other comprehensive factors, the MDT team was of the view that the patient had a high surgical risk and poor prognosis. The patient and her family were thoroughly briefed about the surgical morbidities and associated risks.
During the operation, the patient was placed in Supine position under general anesthesia and received perioperative antibiotic prophylaxis. A circular skin incision, centered on the tumor and including the biopsy scar, was made. The dissection advanced to above the lower part of the pectoralis major and below the upper part of Rectus abdominis muscle.
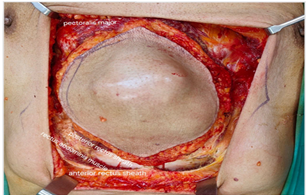
Figure 5: Dissecting above the lower part of the pectoralis major and below the upper part of Rectus abdominis muscle.
Posterior Rectus sheath opened and entered into the peritoneal cavity, and mass separated from the anterior part of the diaphragm. Mass densely adhered to the lower part of the pericardium. Pericardium opened and primarily closed with 2-0 vicryl. The tumor was then resected en bloc and sent for pathologic study.
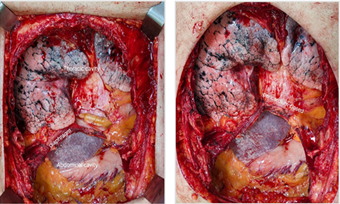
Figure 6A: Tumor resected and pericardium opened. 6B. Pericardium closed primarily 12 cm circular composite mesh placed to repair diaphragmatic defect.

Figure 7: 12 cm circular composite mesh placed to repair diaphragmatic defect.
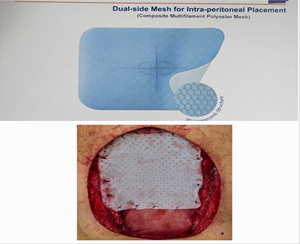
Figure 8: 15x15 cm rectangular composite mesh placed to repair anterior chest wall defect.
Finally, Bilateral pectoralis myocutaneous flaps raised. Rotational advancement flap raised from right side. Advancement flap raised from left side. Skin closed and bilateral ICD inserted. The total operating time was 180 min, and the blood loss was 900 ml.

Figure 9: Bilateral pectoralis myocutaneous flaps raised. Rotational advancement flap raised from right side. Advancement flap raised from left side.
The patient was transferred to the intensive care unit the day after surgery, and back to the general ward on post operative day 2. Antibiotics, aerosol inhalation, and nutritional support treatment were administered. Right and Left chest tubes were removed on postoperative day 5 and 7 respectively. The chest X Ray was normal. The patient had no discomfort and was discharged without any complications on postoperative day 10. The final diagnosis given by the pathologic examination was Chondrosarcoma-Grade-I, No e/o de-differentiation and Excision margins Clear.
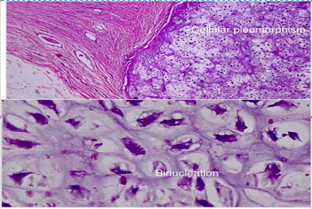
Figure 10: Final diagnosis given by the pathologic examination was Chondrosarcoma-Grade-I
Discussion
It is uncommon for sternum to develop a chondrosarcoma. Chondrosarcomas typically affect people between 40 to 75 years of age with a slight predilection for males [1]. The natural history of chest wall chondrosarcoma involves a slow growing nature and local recurrence. Metastasis occurs late in untreated chondrosarcomas; however, death from primary tumor may occur before the development of metastases [5]. Extensive radiologic study is needed to ascertain the extent of the tumor. Mass seen on examination usually forms only a small portion of the larger tumor invading the sternum. Planar tomography and skeletal survey, former parts of evaluation protocol, have now been replaced by CT scans to assess the extent of the tumor. MRI studies may prove useful in assessing large tumors where there might be mediastinal involvement in form of pericardium, heart or great vessel infiltration [6]. CT scan findings of chondrosarcomas include hypodense, round shaped mass located inside the sternum, the bone is expansive and the cortex is thin and destroyed. PET-CT scan may sometimes help to distinguish benign from malignant bone neoplasm but in well-differentiated tumors, it is difficult to do so since they show marginal FDG-avidity in PET-CT images. Though histopathology report of the excised mass remains the sole determinant for nature of cancer, PET-CT still remains a reliable and valuable modality for detecting the extent of tumor. Histopathologically, chondrosarcomas have characteristic architecture, having abundant hyaline cartilage cell population and a chondromyxoid cartilage matrix. The abnormal cell population consists of round or oval shaped cells with a deeply eosinophilic cytoplasm [6,7].
As of now, surgical excision is the only cure for chondrosarcoma since chemotherapy and radiotherapy remain unhelpful in curing the condition [1,3]. Wide margins determine local recurrence in all grades of chondrosarcoma. Local recurrence impacts disease-specific survival in grade-2 and grade-3 tumors. In grade-1 chondrosarcomas, narrow margins are tolerable. As biopsy does not accurately predict the final tumor grade, in all grades, minimum 4 mm margin remains essential [8]. The tumor grade determines the prognosis. Grade-1 chondrosarcoma carries a favorable prognosis compared to grade-2 or 3 with poor prognosis [5].
Reconstruction of large portions of chest wall had always been a challenge owing to intra-operative difficulty, complications of surgery and respiratory insufficiency resulting from instability of chest wall and paradoxic breathing [6]. A number of materials have been used in reconstructing the chest wall: fascia Lata, rib grafts, large cutaneous flap. The real breakthrough occurred when the use of latissimus dorsi muscle became the norm. The technique for reconstruction depends upon the extent of the skeletal and soft tissue defect [10]. There are several techniques employed for reconstruction of chest wall: Teflon patch + titanium alloy plate, bone cement, 3D printing technology, autologous grafting and titanium internal fixation system. Most of these techniques involve heavy costs, technical skills and long procedure time [3]. A variety of options of prosthesis materials could be used. Materials like Marlex mesh, polytetrafluoroethylene patch and prolene mesh can be used easily. They must be sutured with tension improving chest wall stability. The biggest advantage of using polytetrafluoroethylene is its impermeability against flow of air and fluid [7]. First, skeletal stability must be achieved through the use of prosthesis or bioprosthetics alone or in combination. Then, soft tissue cover must be attained by any of several types of rotational, advancement or free flaps [11,12].
Complications following chest wall resection and reconstruction can be categorized into surgical site complications, respiratory complication and others. Surgical site and respiratory problems are the most common type of complication with an incidence rate of around 40% in some series [13].
This paper describes a case study of an 81-year-old male with a past history of deep venous thrombosis. When the patient started seeing doctors, many hospitals refused him surgery due to his old age, tumor size or other considerations leading to delayed diagnosis. Eventually he came to our hospital for further management. Radiographic imaging including thoracic CT helped in demonstrating distinct features of the tumor. We used composite mesh and bilateral pectoralis myocutaneous flap, which were the least expensive and easiest methods to perform chest wall reconstruction successfully. For the postoperative care of the elderly patients with massive trauma, sufficient amounts of antibiotics and nutritional supplementation are essential. We gave the patient 7 days of antibiotics and enteral nutrients in addition to regular diet and chest physiotherapy to enhance respiratory function. It helped reduce surgical risk and speed up postoperative recovery process. The patient was happy about the postoperative experience. He was discharged after 10 days without developing any complication following successful surgery. In cases where the tumor is not resectable, palliation would still help. This applies particularly to the elderly patients with tumors of enormous size who deserve to live a good life for 3-5 years after surgery.
Conclusion
Sternal giant low-grade chondrosarcoma is an exceptionally rare cancer in elderly patients. The management of such large tumors is difficult because of the location, extent of disease and its invasive nature. Complete removal of the tumor surgically remains an ideal method for dealing with sternal giant chondrosarcomas, and it is imperative to make sure that the surgery is clear of tumor. This case report describes the difficulties encountered while performing the surgery for reasons of patient age, large size of the tumor, mediastinal invasion and pericardial involvement of the mass. Post-surgery antibiotics and nutritional support will also remain crucial. Using our reconstructive methods, chest wall reconstruction can be safely achieved using composite mesh and local flap surgeries in old age with multiple problems.
References
- (2014) A rare case of primary sternal Chondrosarcoma: a case report. Oncol Lett.,
Publisher | Google Scholor - NCCN Clinical Practice Guidelines.
Publisher | Google Scholor - (2024) Surgical case report. Int J Surg Case Rep.,
Publisher | Google Scholor - (2024) Reconstruction of massive chest wall defect after malignant chest wall mass excision in resource limited setting: a case report. Int J Surg Case Rep.,
Publisher | Google Scholor - Orthobullets – Chondrosarcoma.
Publisher | Google Scholor - (1996) Predictors of survival in malignant tumors of the sternum. J Thorac Cardiovasc Surg.,
Publisher | Google Scholor - Chondrosarcoma of the chest wall: factors affecting survival. Ann Thorac Surg.,
Publisher | Google Scholor - Resection of a giant sternal chondrosarcoma and chest wall reconstruction: a cse report. Ann Transl Med.,
Publisher | Google Scholor - The role of surgical margins in chondrosarcoma. Eur J Surg Oncol.,
Publisher | Google Scholor - Analysis of the chest wall reconstruction methods after malignant tumor resection.
Publisher | Google Scholor - Chest wall resection and reconstruction: a 25-year experience. Ann Thorac Surg.,
Publisher | Google Scholor - Chest wall reconstruction after extended resection. J Thorac Dis.,
Publisher | Google Scholor - Management of complications after chest wall resection and reconstruction: a narrative review. J Thorac Dis.,
Publisher | Google Scholor























