

Research Article
Relationship Between Adolescent Sexual Behaviour and Sexually Transmitted Infections Prevalence Among Secondary School Adolescents in Kaiama Community: A Cross-Sectional Study
- Daughter Ewunonam Awala-Owonaro 1
- Peter A. Owonaro 2*
- Akin Moses 3
- Oluwagbenga Ogunfowokan 3
- Omila Aworabhi-Alagoa 3
1Department of Family Medicine, Niger Delta University, Wilberforce Island Bayelsa State, Nigeria.
2Department of Clinical Pharmacy, Niger Delta University, Wilberforce Island Bayelsa State, Nigeria.
3Department of Family Medicine, National Hospital Abuja, Abuja, Nigeria.
*Corresponding Author: Peter A. Owonaro, Department of Clinical Pharmacy, Niger Delta University, Wilberforce Island Bayelsa State, Nigeria.
Citation: Awala-Owonaro DE, Moses A, Ogunfowokan O, Owonaro PA, Aworabhi-Alagoa O. (2026). Relationship Between Adolescent Sexual Behaviour and Sexually Transmitted Infections Prevalence Among Secondary School Adolescents in Kaiama Community: A Cross-Sectional Study, Journal of Women Health Care and Gynecology, BioRes Scientia Publishers. 6(2):1-9. DOI: 10.59657/2993-0871.brs.26.108
Copyright: © 2026 Peter A. Owonaro, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 20, 2026 | Accepted: June 16, 2026 | Published: June 22, 2026
Abstract
The high prevalence of risky sexual behaviour and sexually transmitted infections (STIs) amongst secondary school adolescents constitutes a major public health challenge. In a bid to understand the relationship between adolescent sexual behaviour and STIs among secondary school adolescents in Bayelsa State, an analytic cross-sectional study was carried out from January to March 2020. A multi-staged sampling technique was used to recruit 293 in-school adolescents. Data for socio-demographic characteristics and sexual behaviour were collected using a pre-tested self-administered questionnaire. Blood and urine samples were collected to screen for STIs (Chlamydia, Gonorrhoea, Hepatitis B virus, Syphilis, and HIV infections). Data was analyzed using IBM SPSS version 23.0. Descriptive statistics were summarized, and the Chi-square test was used to examine the statistical relationship between the sexual behaviour and pattern of STIs among the participants. The mean age of the participants was 15.17 ± 1.61 years. Sexual activity (59.4%) and risky sexual behaviour (51.2%; CI = 45.3-57.1%) were high among the participants. A high prevalence of STIs, 36.2% (95% CI = 30.7-42.0), was also found in the study. There was a statistical significance between adolescent sexual behaviour and having an STI (p = 0.0000), having multiple STIs (p = 0.0134), and the pattern of STIs (p = 0.000).
Keywords: sexually transmitted infections; risky sexual behaviour; adolescents
Introduction
Sexually transmitted infections (STIs) are a group of infections which are transmissible from person to person during coitus or other sexual contact [1,2]. Adolescents are disproportionately prone to STIs due to their sexual behaviour, and because most STIs are usually asymptomatic as well as cofactors in HIV transmission, there is the need to reverse this negative trend and safeguard the sexual and reproductive health of adolescents [1,3]. Adolescents and young adults account for almost 50% of all STIs globally, despite the fact that they constitute only one quarter of those who are sexually active, with those within the ages of 16-19 years accounting for the 2nd highest STI prevalence rates globally [2,4-7]. According to the Avert AIDs 2019 report in Nigeria, the south-south geopolitical zone (which Bayelsa State belongs to) has the highest prevalence of HIV, with a prevalence of 4.3% amongst adolescents aged 15-19 years in the region [8]. Studies have shown a rising prevalence of risky sexual behaviours among adolescents,9-11, especially in sub-Saharan Africa and Nigeria, where adolescents constitute 22.5% of the population [9,12-14]. This is even more worrisome given the increasing number of new STI/HIV infections among young people within the region despite the numerous strategies and interventions put in place to curb this menace [15].
A report from the Centre for Disease Control and Prevention (CDC) revealed that, in the United States, about 20 million new cases of sexually transmitted infections occur annually, resulting in a cumulative healthcare cost of 16 billion US dollars, with chlamydial and gonococcal infections been the most common and having the highest prevalence amongst female adolescents (15-19 years) and young adults (20-24 years) [16]. Despite all these challenges, most adolescents do not have access to efficient, effective, and affordable sexual and reproductive health/STI preventive services. Hence, the high rate of untreated STIs and their adverse outcomes, such as pelvic inflammatory disease, chronic pelvic pain, testicular infections, ectopic pregnancy, infertility, and several genital and oropharyngeal cancers [16]. This is due to the belief by many that adolescents are a healthy population and, as such, have little or no need for healthcare. This has led to their non-inclusion in preventive health care services in many health institutions, thereby contributing to the increase in STIs, including HIV/AIDS related morbidity and mortality among adolescents, despite the overall decrease in non-adolescents [17,13,4]. The above findings show that there is more to tackling the issue of STIs/HIV than the current interventions, such as the ABC (Abstinence, being faithful, use of condoms) strategy, family life and HIV education (FLHE) program, and the school-based HIV interventions. Understanding the prevalence and patterns of STIs and their association with sexual behaviour among secondary school adolescents in the Kaiama community is therefore important for informing targeted prevention strategies, strengthening adolescent-friendly health services, and achieving global health targets such as Sustainable Development Goal 3 and WHO STI control strategies [18].
Materials and Methods
Study Area
The study was carried out among secondary school adolescents in the Kaiama community of Bayelsa State. Kaiama is the area council headquarters of the Kolokuma-Opokuma local government area with a population of 77,292.46. The community has a peri-urban setting with a population of 8,764 as at the 1991 population census of Nigeria. The community had two Government secondary schools with a population of 550 and 472 students respectively, and three private secondary schools with a population of 450, 387, 508 students respectively as of April 2019.
Study Population
Male and female adolescents in secondary schools residing in the Kaiama community, who were between the ages of 10 and 19 years. The study was conducted between January and March 2020.
Study Design
Analytical cross-sectional study.
Sample Size Determination
The sample size was calculated using the Cochran equation19 and a prevalence of 24.1% for adolescent risky sexual behaviour.20 Accordingly, the calculated sample size was 262. Adjusting for 10% attrition (for non-response and missing data): N = 262 + 26.2 = 289 participants.
Sampling Technique
Multi-stage sampling technique.
The students were initially grouped according to their schools to ensure adequate coverage and generalizability of the results to the entire adolescent student population in the community. The total number of participants to be drawn from each school and each class was then proportionately allocated as calculated below;
The student population from the schools was as follows: School 1, 550 students; School 2, 472 students, school 3; 450 students; School 4, 387 students; and School 5, 508 students, giving a total of 2,367 students. Hence sample size for school 1 was = 550/2367 X 289 = 67 participants.
For school 2, 472/2367 x 289= 58 participants.
For school 3, 450/2367 x 289= 55 participants.
For school 4, 387/2367 x 289= 47 participants.
For school 5, 508/2367 x 289= 62 participants.
Study Instrument
Collection of data for the study was done using a pre-tested self-administered questionnaire adapted from the youth risk behaviour surveillance survey (YRBSS). The questionnaire consisted of two parts; the socio-demographic characteristics, and sexual behaviour of the study participants.
Study Procedure
The participants were given a health talk on sexual behaviour and STIs. A group pretest counselling for STIs was then offered. After which, they were taken to the sickbay and screened for STIs by the research team. In the course of the procedure, any adverse event, for example, needle prick injury, was documented in the adverse event form and managed appropriately by taking samples for hepatitis B, C, and HIV screening from both persons involved, as well as instituting post-exposure prophylaxis therapy for HIV/HBV. Also, for the purpose of maintaining confidentiality, aside from assuring the participants of this, filling out the questionnaires by consenting participants was done in batches with 5-10 persons per day, during their break period, to allow for privacy, and codes rather than names were used in labeling their samples. Screening for STIs among the participants was done individually at the school sickbay after ensuring that the participant had completely filled out the data recording sheet. Five milliliters of blood were drawn from each of the participants into a sample bottle and labelled with codes for easy identification. After a waiting period of 15-20 minutes, they were informed about their test results individually. A post-test counselling was offered on an individual basis by the counsellors. Participants with negative screening results were counselled on the need to avoid sharing of sharp objects, avoidance of risky sexual behaviours, and on safe sex practices such as abstinence, being faithful, and use of condoms. Those with positive test results were counselled on the need for further confirmatory tests, (using PCR for Chlamydia and gonorrhoea, and TPHA for syphilis) and their urine (for chlamydia and gonorrhoea) and blood (syphilis) samples were collected and sent to laboratory for further analysis using nucleic acid amplification tests techniques (GeneXpert). Those who were confirmed positive by the confirmatory test were counselled and offered treatment and then referred to the adolescent HIV/STD clinic of Federal Medical Centre, Yenagoa, for a repeat test in three months. Those who tested positive for incurable STIs were counselled on healthy living despite being positive, their treatment options, and the need for disclosure to important persons who could help them with their care. With their consent, disclosure was made to their parents, and then they were referred to the adolescent HIV/ STD clinic of Federal Medical Centre, Yenagoa. The researcher had already made the necessary arrangements with the referral center so as to ensure their prompt attendance and care without any additional cost to the participants concerned.
The Determine HIV 1/2 rapid test kit by Abbott (Alere Medical Co; LOT; 01046K00A, EXP. 2021-02-05) was used in screening the participants for HIV 1 & 2. For syphilis, the Aria syphilis antibody rapid test (REF; ROO30S, LOT F1113Q9HO2D; EXP DATE; 2021-05-13) was used for the qualitative detection of anti-treponemal pallidum antibodies syphilis, while the Aria hepatitis surface antigen rapid test (CTK Biotech Poway USA, REF; ROO40S, LOT; FO615Q14OO1D; EXP; 2021-05-17) was used for screening for hepatitis B virus infection among the participants. The Nova immunoglobulin M rapid test kit was used in screening the participants for the chlamydia and gonorrhoea test. A clinical data recording sheet was used to record the results of the screening, and a coding system was used to identify the participants.
Data Analysis
Participants responses from the questionnaires were coded into quantitative data to enable parametric analysis. Data were entered into a Microsoft Excel spreadsheet and then transported into the Statistical Package for the Social Sciences (SPSS) version 23.
Descriptive statistics in the form of charts, frequency tables, and percentages were used in describing the characteristics of the participants (categorical variables) and their sexual behaviour, as well as in determining the prevalence of risky sexual behavior and undiagnosed STI/HIV infection among the participants. While the relationship between adolescent risky sexual behaviour and STIs/HIV positivity was explored using chi square test and Fisher's exact test. Finally, a bivariate logistic regression was used to assess the statistical significance of the relationships found among the variables listed above. A p-value of less than 0.05 was considered significant.
Ethical Issues
Ethical approval was gotten from the Health Research Ethics Committee of the National Hospital, Abuja, and the Bayelsa State Ministry of Health.
A letter of permission to conduct the study was also gotten from the Bayelsa State Post-Primary Schools Board. Informed consent was obtained from each participant’s parent/guardian. The welfare, rights, and confidentiality of the participants were guaranteed throughout the research. The study was carried out in line with the Principles of Good Clinical Practice and in conformity with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of Study Participants
Of the 293 participants, 150 (51.2%) were females, while 143 (48.8%) were males. The mean age of the participants was 15.17 ± 1.61, with a median and modal age of 16 years. The age range of the participants was 11-18 years, with most of them 178 (60.8%) being in their mid-adolescent years (14-16 years). The majority of the respondents, 216 (73.7%), were Ijaws, while the remaining 77 (26.3%) were from other tribes such as Igbo, Yoruba, Hausa, Isoko, Urhobo, and Itsekiri. Christianity was the dominant religion reported by the participants. Over half of the participants, 172 (58.7%), reported that they resided with their parents. Also, S.S.1 had the highest number of respondents (N=71, 24.2%), while J.S.S.1 had the least (N = 25, 8.5%). this is as shown in Table 1.
Table 1: Socio-demographic characteristics of study participants.
| Variables | Frequency (n =293) | Percent (%) |
| Age in Years | ||
| 11 - 13 | 44 | 15.0 |
| 14 - 16 | 178 | 60.8 |
| 17 - 19 | 71 | 24.2 |
| Religion | ||
| Christianity | 265 | 90.4 |
| Islam | 21 | 7.2 |
| None | 5 | 1.7 |
| Others | 2 | 0.7 |
| Living Standard | ||
| Living with both parents | 172 | 58.7 |
| Living with a single parent | 39 | 13.3 |
| Living with step parent | 44 | 15.0 |
| Living with grandparents | 17 | 5.8 |
| Living with relatives | 21 | 7.2 |
| Participants’ Educational Level | ||
| JSS 1 | 25 | 8.5 |
| JSS 2 | 49 | 16.7 |
| JSS 3 | 56 | 19.1 |
| SS 1 | 71 | 24.2 |
| SS 2 | 53 | 18.2 |
| SS 3 | 39 | 13.3 |
(n = number of participants in the study population; N = number of observation)
More than half (N = 176, 60.1%) of the participants' parents were married. On the educational qualification of the participants’ parents, the most frequent educational qualification reported by the respondents was secondary level of education for both parents (fathers’ N = 123, 42.0%, and mothers’ N = 139, 67.6%). On the occupation of their parents, most of the participants had mothers who were civil servants (N = 127, 43.3%) while the majority of their fathers (N = 131, 44.8%) were traders, as shown in Table 2.
Table 2: Marital status, occupation, and educational level of participants' parents.
| Variable | Frequency (N) | Percent | ||
| Marital Status of Participants’ Parents | ||||
| Divorced | 20 | 6.8 | ||
| Separated | 53 | 18.1 | ||
| Married | 176 | 60.1 | ||
| Cohabiting | 44 | 15.0 | ||
| Educational Qualification | Frequency N (%) n=293 | Frequency N (%) n=293 | ||
| Mother | Father | |||
| None | 16 | (5.5) | 27 | (9.2) |
| Primary | 48 | (16.4) | 77 | (26.3) |
| Secondary | 134 | (45.7) | 123 | (42.0) |
| Tertiary | 95 | (32.4) | 66 | (22.5) |
| Occupation | ||||
| Farmer | 58 | (19.8) | 70 | (23.9) |
| Trader | 63 | (21.5) | 131 | (44.7) |
| Fishing | 23 | (7.9) | 18 | (6.2) |
| Civil Servant | 127 | (43.3) | 61 | (20.8) |
| Artisan | 22 | (7.5) | 13 | (4.4) |
Participants Reported Sexual Behaviour
Tables 3 and 4 are the items used in assessing the sexual behaviour of the participants. The items in Table 3 were used in computing the domain rating for the sexual behaviour of the participants. More than half of the participants (59.4%) were sexually experienced. The majority of whom (80.2%) experienced early sexual debut. The mean age at sexual debut among the participants was 14.14 ± 1.99, as shown in Table 3.
Table 3: Participants reported sexual behaviour.
| Sexual Behavior | Frequency | Percentage (%) |
| Ever had sex (n=293) | ||
| Yes | 174 | 59.4 |
| No | 119 | 40.6 |
| Age at sexual debut (n=174) | ||
| ≤ 15 years | 116 | 80.2 |
| ˃ 15 years | 58 | 19.8 |
| Sexual partners in last 12 months (n=174) | ||
| ≤ 1 | 92 | 52.9 |
| ≥ 2 | 82 | 47.1 |
| Use of condom during last sexual encounter (n=174) | ||
| Yes | 83 | 47.7 |
| No | 91 | 52.3 |
| Exchange of gift for sex (n=174) | ||
| Yes | 53 | 30.5 |
| No | 121 | 69.5 |
| Had sex under the influence of drugs or alcohol (n=174) | ||
| Yes | 92 | 52.9 |
| No | 82 | 47.1 |
More than one-third of the sexually experienced participants (35.6%) believed that it was good for adolescents to engage in sexual activity. One-third of them (33.3%) also reportedly engaged in anal sex, while 26.4% of them were bisexual, as shown in Table 4.
Table 4: Participants reported sexual behaviour continued.
| Variable | Frequency (N=174) | Percent (%) |
| Perception About Adolescents Having Sex | ||
| Good | 62 | 35.6 |
| Wrong | 67 | 38.5 |
| Not sure | 45 | 25.9 |
| Preferred Mode of Sexual Intercourse | ||
| Vaginal | 87 | 50.0 |
| Anal | 58 | 33.3 |
| Oral | 2 | 1.2 |
| Vaginal & anal | 21 | 12.1 |
| All three modes (vaginal, anal & oral) | 6 | 3.5 |
| Sexual Orientation | ||
| Heterosexual | 115 | 66.1 |
| Gay | 2 | 1.2 |
| Lesbianism | 11 | 6.3 |
| Bisexual | 46 | 26.4 |
Prevalence/Pattern of STIs in the Study
Among the participants, the prevalence of STIs was 36.2% (95% CI 30.7% - 42.0%). With regards to the pattern of sexually transmitted infections among the respondents, the most common STI among them was gonorrhea, while HIV was the least common. Almost one-third of those with STIs had multiple infections (N = 34; 32.1%) in the figures below.
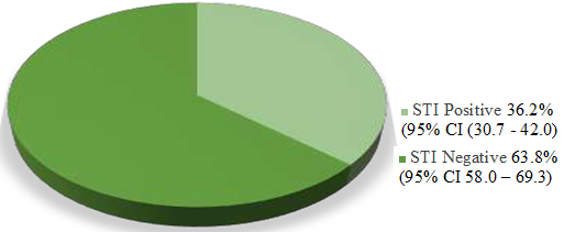
Figure 1: Pie chart showing prevalence of STIs in the study.
Pattern of Infection Amongst STI-Positive Participants
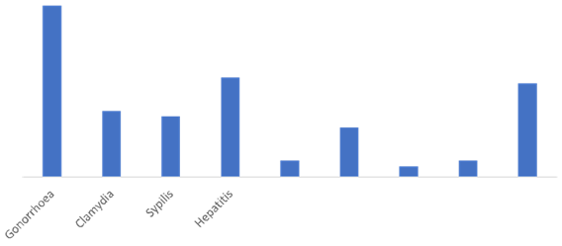
Figure 2: Bar chart showing the pattern of infection amongst STI-positive participants.
A significant association was noted between the participants' sexual behaviour and the frequency (p = 0.000) and pattern (p = 0.000) of STIs amongst them. Also, the association between their sexual behaviour and presence of multiple STIs was significant (p = 0.000) as shown in Table 5. After a logistic regression analysis, the association between having an STI and sexual behaviour remained significant (p=0.000; OR = 0.13; 95% CI = 0.053 – 0.316). Data not shown.
Table 5: Association between sexual behaviour and STI amongst participants.
| Sexual Behaviour | Risky n=150 Frequency (%) | Non-risky n=143 Frequency (%) | Total n=293 | Chi-square X2 | p-value |
| STIs | |||||
| Yes | 85 (56.7) | 21 (14.7) | 106 (36.2) | 55.881 | 0.0000* |
| No | 65 (43.33) | 122 (85.3) | 187 (63.8) | ||
| Multiple STIs | |||||
| Yes | 29 (19.3) | 5 (3.5) | 34 (11.6) | 17.900 | 0.0000* |
| No | 121 (80.7) | 138 (96.5) | 259 (88.4) | ||
| Pattern of STIs | |||||
| No STI | 63 (42.0) | 124 (86.7) | 187 (63.8) | 63.690 | 0.0000* |
| Gonorrhoea & syphilis | 1 (0.7) | 2 (1.4) | 3 (1.0) | ||
| Gonorrhoea & hepatitis B | 8 (88.9) | 1 (5.3) | 9 (3.1) | ||
| Gonorrhoea & HIV | 2 (1.3) | 0 (0.0) | 2 (0.7) | ||
| Gonorrhoea & Chlamydia | 15 (10.0) | 2 (1.4) | 17 (5.8) | ||
| Syphilis & hepatitis B | 3 (2.0) | 0 (0.0) | 3 (1.0) | ||
| Gonorrhoea | 26 (17.3) | 5 (3.5) | 31 (10.6) | ||
| Chlamydia | 11 (7.3) | 1 (0.7) | 12 (4.1) | ||
| Syphilis | 8 (5.3) | 3 (2.1) | 11 (3.75) | ||
| Hepatitis | 13 (8.7) | 5 (3.5) | 18 (6.0) | ||
Discussion
The prevalence of undiagnosed STIs was found to be quite high in the study (36.2%; 95% CI 30.7%-42.0%). This finding was similar to that of Azuike and co-workers in Nnewi, who reported an STI prevalence of 35.8% amongst in-school adolescents, and also that reported in South-Africa [21]. It is, however, slightly higher than the 29.6% reported by Asuke and colleagues [22]. and lower than the self-reported prevalence of 47.1% among in-school adolescents in south-western Nigeria [23]. These findings reveal the huge burden of STIs amongst secondary school adolescents. Also, some other studies reported lower prevalence rates, Anaene et al. (21.6%), [24] Adeomi and co-workers (16.3%), [25] Aliyu and associates (11.6%), [26] and Rutaremwa et al. (STI prevalence= 17.4%; HIV prevalence = 5.3%) [27]. These lower rates may be due to the differences in the study population, study design, and the fact that most of the STI rates were self-reported rather than an actual laboratory diagnosis. The high prevalence of STIs in this study may be due to the high level of risky sexual behaviours reported by the participants.
The most prevalent STIs reported in this study were gonorrhoea and chlamydia, as reported in most studies [7,21,28]. This may be due to their behavioural, biological, and cultural characteristics, which predispose them to STIs. Another issue is the sexual barriers that limit their access to quality STI management and prevention strategies [7]. Most of these infections were asymptomatic, and the majority had no history of STI before the study, as was also reported in similar studies [29,24,21]. This shows the need to strengthen community STI prevention strategies by providing comprehensive health information, education, and promotion for adolescents. Enhancing their access to condoms and vaccines will also aid in reducing their burden [16]. Also, enhancing early diagnosis and treatment of infected persons and their partners through the provision of primary point-of-care screening outlets and use of recommended management guidelines (like the opt-out screening approach) will go a long way in reducing the burden of STIs and their adverse outcomes [16].
This study found the prevalence of HIV among the participants to be 0.3%. This is lower than the findings of John in Jos, Nigeria, who found a HIV prevalence of 2.4% among sexually active adolescents/young persons, and that of Rutaremwa et al in their study in Uganda, who reported a HIV prevalence rate of 5.3% among the participants [30,27]. The higher HIV prevalence rate in these studies may be due to the differences in the age range of the study population, as well as the fact that they were carried out in urban settings in comparison to this study that was done in a peri-urban community.
A significant association (p = 0.000) was noticed between the sexual behaviour of the participants and their being positive for sexually transmitted infections (OR = 0.13; 95% CI = 0.07-0.24). This study also found a significant association (p = 0.027) between the sexual behaviour of the participants and there been positive for multiple STIs (OR = 4.41; 95% CI 1.31-19.70).
Also, the association between the sexual behaviour of the participants and the pattern of STIs was found to be significant (p = 0.000). These findings are in congruence to those of Kao et al, who reported a significant association between the total number of STIs at Wave 3 in the participants and their gender (p less than 0.001, β = .084), being of African American race/ethnicity (p less than 0.001, β= 0.122), family connectedness (p less than 0.001, β = 0.048), and permissive parental attitudes about sex (p less than 0.001, β = 0.065).29 Scott and associates also found in their study that the more risky sexual behaviours reported by the participants, the more the likelihood of them having an STI (odds ratio 1.1) [31]. A significant association between early sexual debut and a lifetime prevalence of STIs, substance use disorder, and depression was also reported in a study carried out in Seattle, Washington DC [32]. In Uganda, Rutaremwa et al reported a significant association between risky sexual behaviour and the risk of having an STI, HIV, or coinfection of STI/HIV (p less than 0.05), with female participants being at a higher risk compared to their male counterparts (p less than 0.001; OR = 2.1; 95% CI = 1.2-2.6) [27]. Their study also revealed a significant association (p = 0.000) between the number of lifetime sexual partners and the likelihood of having an STI (OR = 2.6; 95% CI = 1.8-3.7), testing positive for HIV (OR = 4.5; 95% CI = 2.3-8.6) and having HIV/STI co-infection (OR = 2.8; 95% CI = 2.0-3.9) amongst the participants [27]. Thus, showing the huge toll of risky sexual behaviours on adolescent health. Adolescents face a lot of challenges in safeguarding their sexual and reproductive health, mainly as a result of their cognitive immaturity, which decreases their ability to take cognizance of the long-term consequences of their actions beyond the immediate gratification and their lack of adequate knowledge and information, which they need to enable them make informed decisions [33]. Fatusi et al in their study also reported a significant association between self-reported symptoms of STI and risky sexual behaviour such as early sexual debut (p= 0.021), multiple sexual partners (p less than 0.001), concurrent partners (p = 0.002), and transactional sex (p = 0.013) [34]. This high prevalence of STIs and risky sexual behaviour among the participants in this study may be attributed to a lack of adequate knowledge about STIs, risky sexual behaviour, and its associated outcomes, as was reported by Abbey et al in their study [35].
Recommendations
Adolescent-friendly health clinics should be provided in schools and communities to enhance their access to information and other targeted services like screening for STIs, treatment, and counselling on issues related to their sexual and reproductive health.
Implications for Practice and Policy
Family physicians should be affiliated with school health clinics as consultants to help in the design and implementation of school-based STIs prevention programs, as well as in the training of school teachers, nurses, and health educators on preventive strategies against adolescent risky sexual behaviour and STIs.
References
- Aji J, Aji MO, Ifeadike CO, Emelumadu OF, Ubajaka C, et al. (2013). Adolescent Sexual Behaviour and Practices in Nigeria: A Twelve-Year Review. Afrimedic. 4(1):10-16.
Publisher | Google Scholor - Aladeniyi OB, Bodunwa OK, Sonde M. (2017). Statistical Analysis of Reported Cases of Sexually Transmitted Diseases. Int J Stat Appl. 7(3):186-191.
Publisher | Google Scholor - Gabster A, Pascale JM, Cislaghi B, Francis SC, Weiss HA, et al. (2019). High Prevalence of Sexually Transmitted Infections and High-Risk Sexual Behaviors Among Indigenous Adolescents of the Comarca Ngäbe-Buglé, Panama. Sex Transm Dis. 46(12):780-787.
Publisher | Google Scholor - Morris JL, Rushwan H. (2015). Adolescent Sexual and Reproductive Health: The Global Challenges. Int J Gynecol Obstet. 131:S40-S42.
Publisher | Google Scholor - World Health Organization. (2016). Global Health Sector Strategy on Sexually Transmitted Infections 2016-2021: Towards Ending STIs. 12-17.
Publisher | Google Scholor - Kachur R, Mesnick J, Liddon N, Kapsimalis C, Habel M, et al. (2013). Adolescents, Technology and Reducing Risk for HIV, STDs and Pregnancy. Atlanta, GA Centers Dis Control Prev. 1-72.
Publisher | Google Scholor - CDC. (2018). STDs in Adolescents and Young Adults - 2017 Sexually Transmitted Diseases Surveillance.
Publisher | Google Scholor - United Nations Joint Programme on HIV/AIDS (UNAIDS). (2019). HIV and AIDs in Nigeria. Glob Inf HIV AIDS. 1-16.
Publisher | Google Scholor - Okigbo CC, Kabiru CW, Mumah JN, Sanyu AM, Donatien B. (2015). Influence of Parental Factors on Adolescents’ Transition to First Sexual Intercourse in Nairobi, Kenya: A Longitudinal Study. J Reprod Heal. 12(73):1-12.
Publisher | Google Scholor - Ogunsanmi P, Olusanya M, Olusanya O. (2014). Influence of Quality of Parent-Child Relationship and Parental Communication Styles Among in- School Adolescents in Ondo State. Eur Sci J. 10(16):373-379.
Publisher | Google Scholor - Agius P, Taft A, Hemphill S. (2015). Excessive Alcohol Use and its Association with Risky Sexual Behaviour: A Cross-sectional Analysis of data from Victorian Secondary School Students. Aust N Z J Public Heal. 37(1):76-82.
Publisher | Google Scholor - Salam RA, Faqqah A, Sajjad N, Lassi ZS, Das JK, et al. (2016). Improving Adolescent Sexual and Reproductive Health: A Systematic Review of Potential Interventions. J Adolesc Heal. 59:S11-S28.
Publisher | Google Scholor - UNICEF. (2015). Joint United Nations Programme on HIV and AIDS: Strengthening the Adolescent Component of National HIV Programmes Through Country Assessments. 1-21.
Publisher | Google Scholor - Cortez R, Saadat S, Edmore M, Oluwole O. (2016). Adolescent Fertility and Sexual Health in Nigeria: Determinants and Implications. 1-5.
Publisher | Google Scholor - Adejimi AA, Olagunoye A, Akinkumi G, Agbeleye O, Alawale O, et al. (2017). Evaluation of HIV Prevention Programme Among Out-of-School Youths: Achievements and Implications of HIV/AIDS funded project in Osun. Int J Adolesc Youth. 23(2):171-181.
Publisher | Google Scholor - Hull S, Kelley S, Clarke. JL. (2017). Sexually Transmitted Infections: Compelling Case for an Improved Screening Strategy. Popul Health Manag. 20(1):S1-S10.
Publisher | Google Scholor - Dittus PJ, Michael SL, Becasen JS, Gloppen KM, McCarthy K, et al. (2018). Parental Monitoring and Its Associations with Adolescent Sexual Risk Behaviour: A Meta-analysis. J Paediatr. 136(6):1587-1599.
Publisher | Google Scholor - World Health Organization. (2015). Global Health Sector Strategies 2016-2021 (GHSS) Briefing Note. 1-9.
Publisher | Google Scholor - Adegun PT, Amu EO. (2017). Prevalence and Healthcare-seeking Behaviour for Sexually Transmitted Infections among In-school Adolescents in Ado-Ekiti, South-Western Nigeria. Int J Adolesc Med Health. 29(6):1-7.
Publisher | Google Scholor - Azuike EC, Chisom II, Achunam NS, Emelumadu OF, Seyifumi BJ, et al. (2015). Sexual Behaviour Among Senior Secondary School Students in Nnewi North and Nnewi South Local Government Areas of Anambra State, South-Eastern Nigeria. Eur J Prev Med. 3(2):26-33.
Publisher | Google Scholor - Francis SC, Mthiyane TN, Baisley K, Mchunu SL, Ferguson JB, et al., (2018). Prevalence of Sexually Transmitted Infections Among Young People in South Africa: A Nested Survey in a Health and Demographic Surveillance Site. PLoS Med. 2(15):790-814.
Publisher | Google Scholor - Asuke S, Kurya JM, Olusanmi BT, Hikon YA, Eseigbe P. (2019). Knowledge of Sexually Transmitted Infections and Practice of Risky Sexual Behaviours Among Senior Secondary School Students in Jos North Local Government Area, Plateau State, Nigeria. Port Harcourt Med J. 13(3):87-92.
Publisher | Google Scholor - Korenromp E, Broutet N. (2017). World Health Organization Global Health Sector Strategy on Sexually Transmitted Infections: An Evidence-To-Action Summary for Columbia. 68(3):193-201.
Publisher | Google Scholor - Anaene M, Soyemi K, Caskey R. (2016). Factors Associated with the Over-treatment and Under-treatment of Gonorrhea and Chlamydia in Adolescents Presenting to a Public Hospital Emergency Department. Int J Infect Dis. 53:34-38.
Publisher | Google Scholor - Adeomi AA, Adeoye OA, Adewole A, Israel O, Temitayo-oboh A. (2014). Sexual Risk Behaviours Among Adolescents Attending Secondary Schools in a Southwestern State in Nigeria. J Behav Heal. 3(3):176-180.
Publisher | Google Scholor - Aliyu AA, Dahiru T, Ladan AM, Shehu AU, Abubakar AA, et al., (2013). Knowledge, Sources of information, and Risk Factors for Sexually Transmitted Infections among Secondary School Youths in Zaria, Northern Nigeria. J Med Trop. 5(2):102-106.
Publisher | Google Scholor - Rutaremwa G, Agaba P, Nansubuga EA, Nankinga O. (2015). Association Between Risky Sexual Behaviour and Having STIs or HIV Among Young Persons Aged 15-24 years in Uganda. Paa Confex Com. 1-18.
Publisher | Google Scholor - Ugboma HA, Nwagwu VO, Jeremiah I. (2014). Genital Chlamydia Trachomatis Infection among Female Undergraduate Students of University of Port Harcourt, Nigeria. Niger Med J. 55(1):9-13.
Publisher | Google Scholor - Kao TA, Manczak M. (2013). Family Influences on Adolescents’ Birth Control and Condom Use, Likelihood of Sexually Transmitted Infections. J Sch Nurs. 29(1):61-70.
Publisher | Google Scholor - John C, Okolo SN, Isichei C. (2014). Sexual Risk Behaviour and HIV Infection Among Adolescents in Secondary Schools in Jos, Nigeria. Niger J Paed. 41(2):86-89.
Publisher | Google Scholor - Scott ME, Wildsmith E, Welti K, Ryan S, Schelar E, et al. (2011). Risky Adolescent Sexual Behaviors and Reproductive Health in Young Adulthood. Perspect Sex Reprod Health. 43(2):110-118.
Publisher | Google Scholor - Epstein M, Furlong M, Kosterman R, Bailey JA, King KM, et al. (2018). Adolescent Age of Sexual Initiation and Subsequent Adult Health Outcomes. AJPH. 108(6):822-828.
Publisher | Google Scholor - Kazdouh HE, El-Ammari A, Bouftini S, El-Fakir S, El-Achhab Y. (2019). Perceptions and Intervention Preferences of Moroccan Adolescents, Parents, and Teachers Regarding Risks and Protective Factors for Risky Sexual Behaviours Leading to Sexually Transmitted Infections in Adolescents: Qualitative Findings. Reprod Health. 16(138):1-17.
Publisher | Google Scholor - Fatusi A, Wang W. (2009). Multiple Sexual Partnerships Mediate the Association Between Early Sexual Debut and Sexually Transmitted Infection among Adolescent and Young Adult Males in Nigeria. Eur J Contracept Reprod Heal Care. 14(2):134-143.
Publisher | Google Scholor - Abbey AL, Dozie IN, Iwuala CC, Ede AO, Ebirim CI, et al. (2020). Risky Sexual Behaviours and Practices Associated with HIV/AIDS Infections amongst Youths in Yenagoa LGA, Bayelsa State, Nigeria. J Nurs Heal Sci. 9(1):36-44.
Publisher | Google Scholor























