

Case Report
Recurrent Squamous Cell Carcinoma Arising in a Post-Burn Marjolin Ulcer of the Popliteal Fossa: A Rare Case Report
- Shivani Malik *
- Palak Aggarwal
- Renu Singh
- Lalit Raj
- Ashok Kumar Arya
Department of Radiation Oncology, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
*Corresponding Author: Shivani Malik,Department of Radiation Oncology, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
Citation: Malik S, Aggarwal P, Singh R, Raj L, Ashok K Arya. (2026). Recurrent Squamous Cell Carcinoma Arising in a Post-Burn Marjolin Ulcer of the Popliteal Fossa: A Rare Case Report. International Journal of Medical Case Reports and Reviews. BioRes Scientia Publishers. 6(2):1-6. DOI: 10.59657/2837-8172.brs.26.091
Copyright: © 2026 Shivani Malik, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 15, 2026 | Accepted: June 29, 2026 | Published: July 06, 2026
Abstract
A Marjolin ulcer is a rare and aggressive malignancy that can arise in chronic scars and non-healing wounds, particularly following burn injuries. We describe the case of a 40-year-old man who presented with a recurrent ulcerative lesion in a long-standing post-burn scar over the left popliteal region. Histopathological evaluation confirmed well-differentiated squamous cell carcinoma. Despite surgical excision and reconstruction, the disease recurred locally within a short interval, following which the patient received radiotherapy with partial symptomatic improvement. This case underscores the aggressive nature of malignant transformation in chronic burn scars, the potential for recurrence even after adequate surgery, and the importance of early biopsy and multidisciplinary management of suspicious non-healing lesions.
Keywords: marjolin ulcer; burn scar carcinoma; squamous cell carcinoma; popliteal fossa; recurrent cutaneous malignancy; radiotherapy
Introduction
Marjolin ulcer refers to a malignant neoplasm arising in chronically injured, inflamed, or scarred skin, classically associated with post-burn scars [2]. The term was originally described by the French surgeon Jean-Nicolas Marjolin in the early nineteenth century to characterize ulcerative changes occurring within burn scars. Subsequent studies established that many of these lesions represented malignant transformation, most commonly squamous cell carcinoma (SCC) [4]. Marjolin ulcers account for approximately 2.5% of all cutaneous SCCs, with malignant degeneration reported in 0.7–2% of chronic burn scars [2-5]. The lower extremities are the most frequently affected anatomical site [5]. Compared with de novo cutaneous SCC, Marjolin ulcers demonstrate more aggressive biological behaviour, including higher recurrence rates, increased metastatic potential, and poorer overall prognosis [5-6].
The latency period between the initial injury and malignant transformation is often prolonged, ranging from several years to decades [3,5]. Chronic inflammation, repeated cycles of tissue injury and repair, impaired vascularity, local immune dysfunction, and genetic alterations are believed to play important roles in the pathogenesis of these lesions [4-6]. Because of their aggressive nature and tendency for delayed presentation, early recognition and prompt biopsy of suspicious chronic ulcers or scar changes are essential for timely diagnosis and management [5,6].
We report a rare case of recurrent post-burn Marjolin ulcer involving the popliteal fossa in a middle-aged man with a latency period of approximately 36 years following the initial thermal injury.
Case Presentation
A 40-year-old man was referred to the Department of Radiation Oncology from the Department of General Surgery for further management of recurrent Marjolin ulcer involving the left popliteal fossa. The patient had sustained a thermal burn injury over the posterior aspect of the left thigh and knee region at the age of four years. The injury had been managed conservatively without skin grafting or reconstructive surgery, and healing subsequently occurred with formation of extensive cicatricial scarring and contracture involving the left popliteal region.
The patient remained asymptomatic for nearly 36 years before developing a progressively enlarging non-healing ulcer over the burn scar approximately 10 months prior to presentation. The lesion was associated with pain and intermittent serous discharge. Histopathological examination of the ulcer revealed well-differentiated squamous cell carcinoma consistent with Marjolin ulcer.
The patient underwent wide local excision of the lesion followed by flap reconstruction. Postoperative recovery was initially satisfactory with adequate wound healing and preserved flap viability. Histopathological examination of the excised specimen demonstrated keratoacanthoma-type well-differentiated squamous cell carcinoma measuring 11.2×8.3×3.8 cm. All surgical margins were free of tumor, and no lymphovascular invasion or perineural invasion was identified.
Approximately six months after surgery, the patient developed another non-healing ulcerative lesion at the operative site, raising suspicion of local recurrence. On physical examination, extensive cicatricial scarring was noted over the left popliteal fossa, posterior thigh, and upper leg with surrounding atrophic hyperpigmented and hypopigmented scar tissue changes [Figure 1A]. The reconstructed flap measured approximately 12 × 8 cm and appeared viable. A recurrent nodular-ulceroproliferative lesion measuring approximately 5 × 4 cm with irregular indurated margins, yellowish slough, and focal granulation tissue was identified at the superior aspect of the reconstructed flap [Figure 1B].
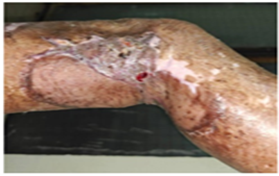
Figure 1A: Clinical photograph showing extensive cicatricial scarring involving the left popliteal fossa, adjacent posterior thigh, and upper leg. The surrounding skin demonstrates atrophic changes with mixed hyperpigmented and hypopigmented mature scar tissue. The postoperative reconstructed flap measuring approximately 12×8 cm appears viable with preserved contour.

Figure 1B: Clinical image demonstrating recurrent nodular-ulcer proliferative lesion arising at the superior aspect of the reconstructed flap in the left popliteal region. The lesion measures approximately 5.0 × 4.0 cm with irregular indurated margins and ulcer base covered with yellowish slough and focal granulation tissue. Electron beam radiotherapy treatment portal for recurrent Marjolin ulcer involving the left popliteal fossa using 12 MeV electrons.

Figure 1C: Clinical photograph obtained during radiotherapy showing development of a smaller satellite ulcerative lesion measuring approximately 2 × 2 cm on the lateral aspect of the left leg below the knee, associated with watery discharge. Treatment field encompassed the primary recurrent lesion along with adjacent satellite ulcerative focus after field modification during treatment course.
Because of persistent clinical suspicion of residual or recurrent disease, contrast-enhanced magnetic resonance imaging (MRI) of the left knee region was performed. Imaging demonstrated an altered signal intensity lesion within the posterolateral subcutaneous tissue of the popliteal region showing minimal post-contrast enhancement and focal diffusion restriction, measuring approximately 5.7 × 19 × 10 mm, suggestive of residual or recurrent disease [Figure 2A]. Diffusion-weighted imaging and corresponding apparent diffusion coefficient mapping showed focal restricted diffusion with an ADC value of approximately 0.92 × 10⁻³ mm²/s, supporting the possibility of residual malignant tissue [Figure 2B]. Associated surrounding muscular edema and mild knee joint effusion were also present [Figure 2C].
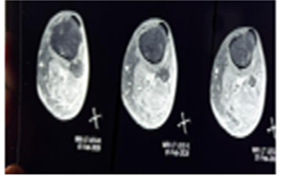
Figure 2A: Contrast-enhanced magnetic resonance imaging (MRI) of the left knee demonstrating an area of altered signal intensity in the posterolateral subcutaneous tissue of the popliteal region with minimal post-contrast enhancement and focal diffusion restriction, suggestive of residual/recurrent lesion.
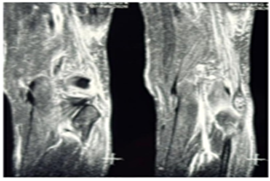
Figure 2B: MRI diffusion-weighted imaging (DWI) and corresponding apparent diffusion coefficient (ADC) map showing focal restricted diffusion within the lesion (ADC value approximately 0.92×10⁻³ mm²/s), consistent with residual malignant tissue.
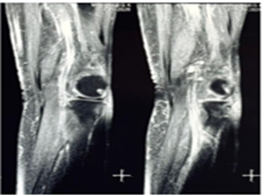
Figure 2C: MRI of the left knee revealing associated surrounding muscular edema and mild knee joint effusion adjacent to the recurrent lesion in the popliteal fossa region.
In view of recurrent disease, the patient was planned for adjuvant external beam radiotherapy using a linear accelerator (Elekta Versa HD) with 12 MeV electron beam therapy and 0.5 cm wet cotton bolus using a treatment field size of 14 × 8 cm. The treatment portal is shown in Figure 1B. A total dose of 50 Gy in 25 fractions was prescribed with the expectation of achieving improved local disease control, reduction in tumor burden, symptomatic relief, and prevention of further locoregional progression.
During the course of radiotherapy, the patient developed a smaller adjacent satellite ulcerative lesion measuring approximately 2 × 2 cm with watery discharge along the lateral aspect of the left leg below the knee after six fractions of treatment [Figure 1C]. The treatment fields were subsequently reassessed and modified to include the newly developed lesion. However, despite repeated counselling and telephonic follow-up, the patient discontinued treatment because of personal and family-related circumstances and received only 28 Gy in 14 fractions.
At the last follow-up visit, partial clinical response was observed with approximately 40% reduction in lesion size along with reduction in discharge and bleeding. Although complete treatment could not be delivered, the patient demonstrated symptomatic improvement and partial local disease regression following radiotherapy.
Discussion
Marjolin ulcer is a rare but highly aggressive cutaneous malignancy arising in chronically damaged or previously traumatized skin, most commonly within post-burn scars [2-3]. Although the term was initially used to describe malignant degeneration occurring in burn scars, it now broadly encompasses malignancies arising in chronic wounds, pressure sores, venous ulcers, osteomyelitic sinuses, radiation dermatitis, and other longstanding inflammatory dermatoses [2-8]. Squamous cell carcinoma (SCC) remains the predominant histological subtype, accounting for the majority of reported cases [5]. Compared with conventional cutaneous SCC, Marjolin ulcers exhibit more aggressive biological behavior, including higher rates of local recurrence, regional nodal metastasis, and disease-specific mortality [5-6].
The incidence of malignant transformation in chronic burn scars has been reported to range between 0.7% and 2%, while burn scar-associated malignancies constitute approximately 2.5% of all cutaneous SCCs [2-5]. Lower extremities are the most commonly affected anatomical sites, likely due to increased frequency of trauma, delayed wound healing, and chronic irritation in these regions [5]. Involvement of the popliteal fossa, as observed in the present case, is uncommon and clinically significant because of the proximity to major neurovascular structures and repeated movement-related mechanical stress, which may impair wound healing and facilitate malignant progression [1].
The pathogenesis of Marjolin ulcer is multifactorial and incompletely understood [2-8]. Chronic inflammation is believed to play a central role in carcinogenesis through persistent cycles of tissue destruction and regeneration, leading to continuous cellular proliferation and accumulation of genetic mutations [2-8]. Poor vascularity, lymphatic obliteration, impaired immune surveillance, repeated secondary infection, and chronic irritation collectively create a pro-oncogenic microenvironment [2-8]. Molecular alterations involving tumor suppressor genes such as TP53, defective apoptotic pathways including Fas gene mutations, and increased oxidative stress have also been implicated in malignant transformation [6]. Furthermore, chronic scar tissue often lacks adequate lymphatic drainage, resulting in delayed immune recognition and facilitating unchecked tumor progression [8].
A characteristic feature of Marjolin ulcer is the prolonged latency period between the initial injury and malignant transformation, typically ranging from 20 to 40 years [2-5]. In the present case, SCC developed approximately 36 years after the initial thermal injury, which is consistent with previously reported literature [1]. Such prolonged latency frequently contributes to delayed diagnosis because chronic scar changes may mask early malignant transformation [5]. Clinically, the development of pain, foul-smelling discharge, bleeding, induration, rapid increase in size, nodularity, or ulceration within a longstanding scar should raise suspicion for malignant degeneration and warrant immediate biopsy [2-8].
Histopathologically, our patient demonstrated well-differentiated SCC of keratoacanthoma type with negative resection margins and absence of lymphovascular or perineural invasion. Despite these relatively favourable pathological features, the patient developed local recurrence within six months of surgery, highlighting the aggressive nature of Marjolin ulcer and its propensity for recurrence even after apparently adequate surgical excision [5-7]. Reported recurrence rates for Marjolin ulcer are considerably higher than those for de novo cutaneous SCC, emphasizing the importance of meticulous long-term surveillance [5-6].
Wide local excision remains the cornerstone of treatment for localized disease [6-7]. Most authors recommend surgical margins of 2–3 cm with histopathological margin assessment whenever feasible [6-7]. Reconstruction using skin grafts or flaps is frequently required because these lesions are often extensive and associated with underlying scar contractures [7]. In advanced cases with osseous involvement, neurovascular infiltration, or unresectable disease, amputation may be considered, although its survival benefit remains controversial [7]. Sentinel lymph node evaluation and regional nodal assessment are important because nodal metastasis significantly worsens prognosis [5-6].
Radiotherapy has an important adjunctive role in recurrent disease, positive or close surgical margins, nodal metastasis, inoperable lesions, large tumours, poorly differentiated tumours, and in patients unsuitable for surgery [5-6]. Electron beam radiotherapy was selected in our patient because of the superficial location of the lesion and the ability of electron therapy to deliver adequate surface dose while sparing deeper structures. Although the planned dose was 50 Gy in 25 fractions, the patient discontinued treatment after receiving 28 Gy in 14 fractions because of personal reasons. Nevertheless, partial clinical response with reduction in lesion size and discharge was observed, suggesting radiosensitivity of the recurrent lesion. The development of a satellite ulcerative lesion during treatment further reflected the aggressive local behaviour of the disease.
Recent advances in systemic therapy, particularly immune checkpoint inhibitors such as Pembrolizumab and Cemiplimab, have demonstrated promising outcomes in advanced and metastatic cutaneous SCC, including selected cases of Marjolin ulcer [6]. However, evidence remains limited because of the rarity of the condition, and standardized treatment guidelines are still lacking [6].
The present case is noteworthy because of several uncommon and clinically relevant features, including occurrence in the popliteal fossa, an exceptionally long latency period following childhood burn injury, early postoperative recurrence despite histologically negative margins, and partial response to incomplete adjuvant radiotherapy [1]. This case highlights the importance of early burn wound reconstruction, lifelong surveillance of chronic scars, prompt biopsy of suspicious lesions, and multidisciplinary management in achieving optimal outcomes in patients with Marjolin ulcer [5-8].
Conclusion
Marjolin ulcer is a rare but highly aggressive malignancy associated with chronic scar tissue and longstanding non-healing wounds. Early biopsy of suspicious ulcerative lesions arising within burn scars is essential for prompt diagnosis and treatment. Although surgery remains the primary treatment modality, recurrence remains common, necessitating close long-term surveillance. This case further highlights the role of radiotherapy in recurrent disease and underscores the need for standardized management protocols for Marjolin ulcer.
Ethics Statement
Written informed consent for publication was obtained from the patient. Ethical approval was not required according to institutional policy because no experimental intervention was performed. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Declarations
Author Contributions
Shivani Malik: Conceptualization, Manuscript writing and critical revision
Palak Aggarwal: data collection, manuscript drafting
Renu Singh: Literature review
Lalit Raj: Histopathological interpretation
Ashok Kumar Arya: Supervision and final approval
All authors reviewed and approved the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
No external funding was received for this study.
Acknowledgements
I would be like to acknowledge Mr. Ankur Ghangas for significant help in drafting the manuscript.
References
- Kaushik R, Nayyar A (2025). A rare presentation of Marjolin ulcer in burn scar in popliteal fossa. Indian J Pathol Oncol.,12:174-177.
Publisher | Google Scholor - Marietta M, Crane JS (2025). Marjolin Ulcer. StatPearls [Internet]. StatPearls Publishing, Treasure Island (FL).
Publisher | Google Scholor - Alia M, Ben Ammar C, Dhambri S, Kedous S (2025). Retroauricular squamous cell carcinoma developing on a burn scar: Marjolin’s ulcer—a case report and review of the literature. Int J Surg Case Rep., 130:111183.
Publisher | Google Scholor - Fleming MD, Hunt JL, Purdue GF, Sandstad J (1990). Marjolin’s ulcer: a review and reevaluation of a difficult problem. J Burn Care Rehabil.,11:460-469.
Publisher | Google Scholor - Abdi MA, Yan M, Hanna TP (2020). Systematic review of modern case series of squamous cell cancer arising in a chronic ulcer (Marjolin’s ulcer) of the skin. JCO Glob Oncol.,6:809-818.
Publisher | Google Scholor - Kanth AM, Heiman AJ, Nair L, et al., (2021). Current trends in management of Marjolin’s ulcer: a systematic review. J Burn Care Res., 42:144-151.
Publisher | Google Scholor - Aydoğdu E, Yildirim S, AközT (2005). Is surgery an effective and adequate treatment in advanced Marjolin’s ulcer? Burns.31:421-431.
Publisher | Google Scholor - Pekarek B, Buck S, Osher L (2011). A comprehensive review on Marjolin’s ulcers: diagnosis and treatment. J Am Col Certif Wound Spec.,3:60-64.
Publisher | Google Scholor























