

Research Article
Prevalence of Coeliac Disease Among Symptomatic Patients: A Retrospective Study from a Tertiary Care Hospital in North-East Delhi
1Senior Resident, Department of Microbiology, University College of Medical Sciences, Dilshad Garden, Delhi, India.
2Associate Professor, Department of Microbiology, University College of Medical Sciences, Dilshad Garden, Delhi, India.
3Post Graduate [PG-1], Microbiology Department, University College of Medical Sciences, Dilshad Garden, Delhi, India.
4HOD, Director Professor, Microbiology Department, University College of Medical Sciences, Dilshad Garden, Delhi, India.
*Corresponding Author: Nadeem Ahmad, Associate Professor, Department of Microbiology, University College of Medical Sciences, Dilshad Garden, Delhi, India.
Citation: Nirmal S, Ahmad N, Semwal D, Das S. (2025). Prevalence of Coeliac Disease Among Symptomatic Patients: A Retrospective Study from a Tertiary Care Hospital in North-East Delhi, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(4):1-6. DOI: 10.59657/2997-6103.brs.25.096
Copyright: © 2025 Nadeem Ahmad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 22, 2025 | Accepted: October 07, 2025 | Published: October 13, 2025
Abstract
Abstract
Background: Coeliac disease (CD) is an immune-mediated small intestinal disorder precipitated by gluten consumption in genetically predisposed individuals. The condition is increasingly recognized worldwide, including in India, largely due to better availability of serological assays and awareness of non-classical manifestations.
Aim: To determine the prevalence of Coeliac disease among patients presenting with gastrointestinal and related complaints using serological screening.
Materials and Methods: This retrospective study was carried out in the Department of Microbiology, UCMS & GTB Hospital, Delhi, and included 752 consecutive serum samples received between May 2023 and July 2025. IgA anti-tTG antibodies were estimated by Quantitative ELISA (Aeskulisa, Aesku Diagnostics, Germany) employing recombinant human antigen. Results were interpreted as negative (<16 IU/mL), equivocal (16–19 IU/mL), or positive (≥20 IU/mL).
Results: Among 752 patients, 99 (13%) tested positive, 633 (84%) were negative, and 20 (3%) yielded equivocal findings. Males constituted 59% of the study group, with a slight male predominance among positive cases (55.5%). The highest frequency of positivity (87%) was observed in the 1–20 years age group, mainly in children aged 1–10 years. The majority of samples originated from the Paediatrics Department.
Conclusion: CD was detected in 13% of symptomatic patients, with the greatest burden in the paediatric age group. These results highlight the importance of early serological screening in high-risk groups to facilitate timely diagnosis and prevention of long-term sequelae.
Keywords: coeliac disease; gluten-free diet; gastrointestinal symptoms; anti-tTG
Introduction
Coeliac disease (CD) is a chronic autoimmune-mediated condition of the small intestine triggered by gluten ingestion in genetically susceptible hosts [1]. Gluten, a storage protein found in wheat, barley, and rye, provokes an abnormal immune response that damages the intestinal mucosa, producing villous atrophy, crypt hyperplasia, and malabsorptive symptoms. Once regarded as an uncommon entity, CD is now one of the most frequently encountered disorders globally. Besides being limited to the gut, it is increasingly viewed as a multisystem disease with varied clinical expressions. Early institution of a strict gluten-free diet (GFD) remains the cornerstone of management and can reverse intestinal injury, improve growth parameters in children, and prevent complications [2].
Genetic susceptibility is central, with nearly 95% of affected individuals carrying the HLA-DQ2 haplotype and most of the remainder carrying HLA-DQ8 [3]. Nevertheless, only about one-third of siblings develop disease, underscoring the role of additional immunological and environmental triggers [4]. Gluten-driven T-cell activation leads to the generation of autoantibodies, notably anti–tissue transglutaminase. The condition is also more common in association with autoimmune endocrinopathies such as type 1 diabetes mellitus and autoimmune thyroid disease, as well as in patients with a positive family history [5,6].
Epidemiological studies report a global prevalence of 0.7-1.8%, with a female preponderance in several cohorts [7,8]. In India, hospital-based studies have demonstrated a prevalence of approximately 3.75% among patients presenting with gastrointestinal and related symptoms, with the highest burden consistently reported from North India [9]. This apparent rise is attributed not only to improved awareness and availability of diagnostic facilities but also possibly to changing environmental exposures and dietary patterns [10,11].
The clinical spectrum of CD is highly heterogeneous. Classical disease typically presents with malabsorptive complaints including chronic diarrhoea, steatorrhea, abdominal bloating, anorexia, and weight loss [12]. In children, growth retardation, failure to thrive, and delayed puberty are characteristic. Increasingly, atypical or non-classical forms predominate, manifesting as recurrent abdominal pain, constipation, or vague dyspepsia without diarrhoea. Extra-intestinal manifestations are particularly important, often being the sole presentation. These include iron deficiency anaemia, metabolic bone disease, short stature, delayed menarche, infertility, recurrent miscarriages, unexplained elevation of liver enzymes, dermatitis herpetiformis, and neurological features such as ataxia and peripheral neuropathy [13,14]. Such diverse clinical profiles contribute to under-recognition and diagnostic delay.
Diagnosis relies on a combination of serology and duodenal histology. Current guidelines, including those of the National Institute for Health and Care Excellence (NICE), recommend measuring total IgA and IgA anti-tTG as initial screening. In IgA deficiency, IgG-based assays such as Endomysial Antibody (EMA), Deamidated Gliadin Peptide (DGP), or IgG-tTG are preferred. The availability of highly sensitive and specific serological assays has facilitated case detection and epidemiological studies. Newer diagnostic approaches under evaluation include blood-based T-cell assays measuring gluten-specific cytokine release, advanced HLA risk stratification, and AI-supported histological interpretation, which may further enhance diagnostic accuracy [15].
Given the growing recognition of CD in India, particularly in the northern states, the present study aimed to evaluate its prevalence in patients with gastrointestinal symptoms attending a tertiary care hospital in North-East Delhi.
Materials and Methods
This retrospective study was carried out in the Department of Microbiology, University College of Medical Sciences and Guru Tegh Bahadur Hospital, Delhi. A total of 752 consecutive serum samples submitted for suspected coeliac disease between May 2023 and July 2025 were included in the analysis.
Serological evaluation was performed by estimating IgA anti–tissue transglutaminase antibodies (anti-tTGA) using a commercial ELISA kit (Aeskulisa, Aesku Diagnostics, Germany) that incorporates recombinant human tissue transglutaminase as the antigen. Test results were interpreted in accordance with the manufacturer’s guidelines: values less than 16 IU/mL were classified as negative, 16-19 IU/mL as equivocal, and ≥20 IU/mL as positive. Internal quality controls supplied with the kit were run with each batch to verify assay accuracy and consistency.
Alongside laboratory findings, relevant demographic and clinical information was systematically extracted to assess associations with serological outcomes. Data analysis was conducted using SPSS software.
Results
A total of 752 patients presenting with gastrointestinal or related symptoms were assessed for suspected coeliac disease. Overall, males accounted for 59% of the study population, while females represented 41%. Among those who tested positive, a modest male predominance was observed (55.5% vs. 44.5%) [Figure 1].
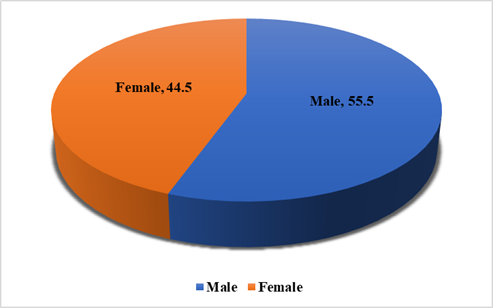
Figure 1: Gender-wise Distribution of cases in the Study Population (%).
Serological screening using IgA anti-tTG ELISA identified 99 positive cases (13%), 633 negative cases (84%), and 20 patients (3%) with equivocal results requiring further clinical correlation [Figure 2]. Taken together, the prevalence of coeliac disease in this symptomatic cohort was 13%, considerably higher than estimates from community-based studies.
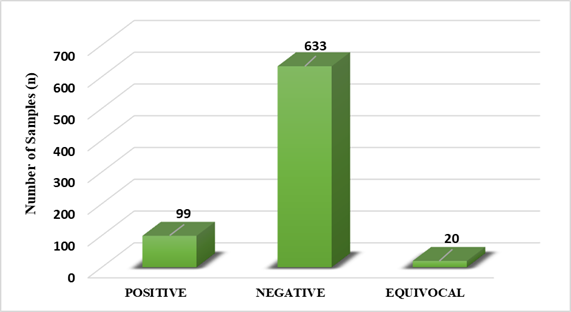
Figure 2: Frequency of Coeliac Disease in Patients Attending a Tertiary Care Centre (n=752).
Age distribution analysis showed that the vast majority of samples (87%) were obtained from patients aged 1-20 years, with the highest contribution from children between 1 and 10 years. Representation declined progressively across the 21-40, 41-60, and greater than 60-year groups. A similar trend was evident in the positive cohort, with most confirmed cases clustering within the paediatric and adolescent age ranges [Table 1].
Table 1: Age Group Distribution of Patients with Gastrointestinal Symptoms Screened for Coeliac Disease (n=752).
| Age Groups (in years) | Number of Samples (n=752) |
| 0-10 years | 458 |
| 11-20 years | 135 |
| 21-30 years | 77 |
| 31-40 years | 41 |
| 41-50 years | 17 |
| 51-60 years | 12 |
| 61-70 years | 8 |
| 71-80 years | 4 |
| Total | 752 |
Department-wise analysis revealed that the Paediatrics unit submitted the largest proportion of samples (n = 470), followed by Medicine (n = 140), Dermatology (n = 96), the Antenatal Clinic (n = 39), and ENT (n = 7). This departmental pattern corresponded closely with the age profile, as the majority of positive cases were identified in children [Figure 3].
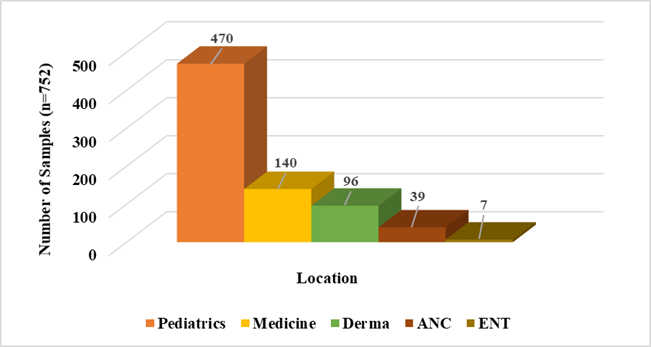
Figure 3: Location-based Distribution of samples Screened for Coeliac Disease (n=752).
Discussion
Coeliac disease (CD) is an immune-mediated disorder of the small intestine, triggered by gluten ingestion in genetically susceptible individuals. Lifelong adherence to a gluten-free diet (GFD) remains the only effective treatment, though this can pose significant challenges in countries like India, where wheat is a staple dietary component [16].
In the present study, celiac disease was detected in 13% of symptomatic patients, a prevalence that aligns with-or slightly exceeds-previous hospital-based reports from India (6-12%) [17] while lower rates (3-4%) have also been documented in earlier studies [9]. This elevated detection likely reflects the high-risk profile of tertiary care populations and highlights the importance of maintaining heightened clinical vigilance, particularly in paediatric and medical outpatient settings, where most cases were identified.
Community-based surveys report considerably lower prevalence rates. For example, Makharia et al. [18] found a prevalence of 1.44% in a large Northern Indian cohort, while Sood et al. [19] reported 0.32% among school-aged children in Punjab. Similarly, in the United States, Rubio-Tapia et al. [20] documented a community prevalence of approximately 1%. By contrast, hospital-based studies consistently demonstrate higher rates among symptomatic populations, highlighting the value of targeted screening in high-risk clinical settings [17].
Age-wise analysis in our cohort revealed that nearly 87% of cases were in the 1-20 years range, with the highest concentration (61%) among children aged 1-10 years. This aligns with previous reports from India and other Asian countries, where CD frequently presents early in life [21,22]. Poddar et al. [23] noted that paediatric patients in North India often present with chronic diarrhoea, abdominal distension, and growth retardation, frequently resulting in severe malnutrition if undiagnosed. Similarly, Bhattacharya et al. [24] emphasized the burden of CD in children in Eastern India, with growth failure and anaemia as common initial signs. The findings of above studies support routine screening for children with chronic gastrointestinal symptoms or unexplained anaemia.
Gender distribution in our cohort showed a slight male predominance (55.5%), although this difference was not statistically significant. While Western populations often demonstrate a female preponderance [25], Indian studies report mixed patterns. For instance, a large North Indian cohort showed higher female prevalence [18], whereas another study from India observed nearly equal male-to-female ratios [23]. Such differences may be influenced by healthcare-seeking behaviour, referral bias, and sociocultural factors affecting access to care.
In terms of departmental distribution, the majority of samples originated from the Paediatrics Department, followed by Medicine, reflecting the age distribution of patients. Positive cases were also identified from Dermatology, Antenatal Clinic, and ENT clinics, indicating the spectrum of extra-intestinal manifestations. Globally, studies by Marsh [26] and Green & Cellier [27] have described atypical presentations such as infertility, recurrent pregnancy loss, osteoporosis, cryptogenic hypertransaminasia, and neurological complications, which often present to non-gastroenterology specialties. These observations highlight the importance of interdisciplinary awareness and inclusion of CD in differential diagnoses across various clinical departments.
The clinical implications of these findings are significant. Untreated CD can lead to long-term complications including iron deficiency anaemia, osteoporosis, infertility, and in rare cases, enteropathy-associated T-cell lymphoma (EATL) [28]. Early diagnosis, particularly in children, is crucial to prevent irreversible consequences such as growth retardation and delayed puberty. Hospital-based screening initiatives are suggested based on the findings of current study. The study also demonstrates that proactive case finding in high-risk groups facilitates earlier diagnosis and better outcomes [29,30].
This study had some limitations. Being a retrospective analysis, detailed clinical data and histopathological confirmation were not uniformly available, which may have affected prevalence estimates. Furthermore, the hospital-based design reflects a high-risk population and does not represent the true community prevalence.
Nonetheless, the study’s strengths include a large sample size and systematic evaluation across multiple departments, providing valuable insights into the epidemiology of CD in North-East Delhi.
Conclusion
This study demonstrates a substantially higher prevalence of CD among symptomatic patients compared to community-based estimates, with the majority of cases occurring in the paediatric age group. The findings emphasize the importance of routine serological screening in high-risk populations (Chronic diarrhoea, malabsorption, unexplained anemia, Type 1 diabetes mellitus) complemented by histopathological confirmation to ensure accurate diagnosis. Enhancing clinician awareness, particularly in paediatrics and general medicine, is essential for timely detection and for minimizing long-term morbidity associated with undiagnosed CD.
Acknowledgment
We would like to sincerely thank the staff of the Serology Section, Department of Microbiology, for their invaluable support and assistance in conducting this study. Their expertise and dedication greatly contributed to the successful completion of this work.
References
- Ludvigsson JF, Leffler DA, Bai JC, Biagi F, Fasano A, et al. (2013). The Oslo Definitions for Coeliac Disease and Related Terms. Gut. 62(1):43-52.
Publisher | Google Scholor - Fasano A, Catassi C. (2012). Clinical Practice. Celiac Disease. N Engl J Med. 367(25):2419-2426.
Publisher | Google Scholor - Sollid LM, Lie BA. (2005). Celiac Disease Genetics: Current Concepts and Practical Applications. Clin Gastroenterol Hepatol. 3(9):843-851.
Publisher | Google Scholor - Van Heel DA, West J. (2006). Recent Advances in Coeliac Disease. Gut. 55(7):1037-1046.
Publisher | Google Scholor - Smyth DJ, Plagnol V, Walker NM, Cooper JD, Downes K, et al. (2008). Shared and distinct genetic variants in type 1 diabetes and celiac disease. N Engl J Med. 359(26):2767-2777.
Publisher | Google Scholor - Fasano A. (2005). Clinical Presentation of Celiac Disease in The Pediatric Population. Gastroenterology. 128(4 Suppl 1):S68-S73.
Publisher | Google Scholor - Singh P, Arora A, Strand TA, Leffler DA, Catassi C, et al. (2018). Global Prevalence of Celiac Disease: Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol. 16(6):823-836.
Publisher | Google Scholor - Catassi C, Gatti S, Fasano A. (2014). The New Epidemiology of Celiac Disease. J Pediatr Gastroenterol Nutr. 59 Suppl 1:S7-S9.
Publisher | Google Scholor - Meena M, Sood A, Choudhary S, et al. (2024). Prevalence and Predictors of Celiac Disease in Children with Constipation: A Hospital-Based Study. J Pediatr Gastroenterol Nutr. 69(4):e89-e94.
Publisher | Google Scholor - Gibson PR. (2020). Commentary: Recognising the Boom in Coeliac Disease. Aliment Pharmacol Ther. 51(6):552-553.
Publisher | Google Scholor - Lohi S, Mustalahti K, Kaukinen K, Laurila K, Collin P, et al. (2007). Increasing Prevalence of Coeliac Disease Over Time. Aliment Pharmacol Ther. 26(9):1217-1225.
Publisher | Google Scholor - Adams DW, Arnone JA, Fasano A. (2024). Clinical Presentation and Spectrum of Gluten-Related Disorders. Gastroenterology. 166(5):1071-1088.
Publisher | Google Scholor - Tovoli F, Negrini G, Farì R, Guidetti E, Faggiano C, et al. (2014). Increased Prevalence of Celiac Disease among Patients with Unexplained Iron-Deficiency Anemia in Northern Sardinia. J Gastrointestin Liver Dis. 23(1):15-19.
Publisher | Google Scholor - Hadjivassiliou M, Grünewald RA, Davies-Jones GAB. (2002). Gluten Sensitivity as a Neurological Illness. J Neurol Neurosurg Psychiatry. 72(5):560-563.
Publisher | Google Scholor - Ludvigsson JF, Bai JC, Biagi F, Card TR, Ciacci C, et al. (2014). Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology. Gut. 63(8):1210-1228.
Publisher | Google Scholor - Fasano A, Catassi C. (2012). Clinical Practice. Celiac Disease. N Engl J Med. 367(25):2419-2426.
Publisher | Google Scholor - Gupta R, Reddy DN, Makharia GK, et al. (2013). Prevalence and Clinical Profile of Celiac Disease in Indian Patients: A Multicenter Hospital-Based Study. Indian J Gastroenterol. 32(6):380-386.
Publisher | Google Scholor - Makharia GK, Verma AK, Amarchand R, Bhatnagar S, Das P, et al. (2011). Prevalence of Celiac Disease in The Northern Part of India: A Community-Based Study. J Gastroenterol Hepatol. 26(5):894-900.
Publisher | Google Scholor - Sood A, Midha V, Sood N, Kaushal V, Puri H. (2001). Increasing Incidence of Celiac Disease in India. Am J Gastroenterol. 96(9):2804-2805.
Publisher | Google Scholor - Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA, Everhart JE. (2012). The Prevalence of Celiac Disease in The United States. Am J Gastroenterol. 107(10):1538-1544.
Publisher | Google Scholor - Kang JY, Kang AH, Green A, Gwee KA, Ho KY. (2013). Systematic Review: Worldwide Variation in the Frequency of Coeliac Disease and Changes Over Time. Aliment Pharmacol Ther. 38(3):226-245.
Publisher | Google Scholor - Gujral N, Freeman HJ, Thomson AB. (2012). Celiac Disease: Prevalence, Diagnosis, Pathogenesis and Treatment. World J Gastroenterol. 18(42):6036-6059.
Publisher | Google Scholor - Poddar U, Thapa BR, Singh K. (2006). Clinical Features of Celiac Disease in Indian Children: Are they Different from The West? J Pediatr Gastroenterol Nutr. 43(3):313-317.
Publisher | Google Scholor - Bhattacharya M, Kapoor S, Dubey AP. (2013). Celiac disease presentation in a tertiary referral centre in India: current scenario. Indian J Gastroenterol. 32(2):98-102.
Publisher | Google Scholor - Catassi C, Fabiani E, Corrao G, Barbato M, De Renzo A, et al. (2002). Risk of Non-Hodgkin Lymphoma in Celiac Disease. JAMA. 287(11):1413-1419.
Publisher | Google Scholor - Marsh MN. (1992). Gluten, Major Histocompatibility Complex, and The Small Intestine. A Molecular and Immunobiologic Approach to The Spectrum of Gluten Sensitivity (‘Celiac Sprue’). Gastroenterology. 102(1):330-354.
Publisher | Google Scholor - Green PHR, (2007). Cellier C. Celiac Disease. N Engl J Med. 357(17):1731-1743.
Publisher | Google Scholor - West J, Logan RF, Hill PG, Lloyd A, Lewis S, et al. (2003). Seroprevalence, correlates, and characteristics of undetected coeliac disease in England. Gut. 52(7):960-965.
Publisher | Google Scholor - Catassi C, Kryszak D, Bhatti B, Sturgeon C, Helzlsouer K, et al. (2010). Natural History of Celiac Disease Autoimmunity in A USA Cohort Followed Since 1974. Ann Med. 42(7):530-538.
Publisher | Google Scholor - Singh P, Shergill S, Makharia S, Mishra A, Makharia GK. Celiac Disease in Women with Infertility: A Systematic Review and Meta-Analysis. J Clin Gastroenterol. 50(1):33-39.
Publisher | Google Scholor























