

Research Article
Postnatal Contraceptive Behaviour and Influencing Factors in Karonmajiji and Lugbe, Abuja: A Comparative Analysis
1Unicaf University Zambia Federal Medical Centre, Abuja.
2Adjunct Faculty, Department of Social Work, Unicaf University, Zambia.
3Faculty of Science, University of Abuja, Abuja-FCT.
*Corresponding Author: Ochala Ejura Jennifer, Unicaf University Zambia Federal Medical Centre, Abuja.
Citation: : Jennifer O E, Arafath A M Y, Rauf R I. (2025). Postnatal Contraceptive Behaviour and Influencing Factors in Karonmajiji and Lugbe, Abuja: A Comparative Analysis, Journal of Women Health Care and Gynecology, BioRes Scientia publishers. 5(5):1-12. DOI: 10.59657/2993-0871.brs.25.093
Copyright: © 2025 Ochala Ejura Jennifer, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 10, 2025 | Accepted: March 25, 2025 | Published: April 02, 2025
Abstract
Background: Postpartum contraceptive use is critical in preventing closely spaced pregnancies, reducing maternal and infant mortality, and improving reproductive health outcomes. This study examines the contraceptive behaviours of postnatal mothers in Karonmajiji and Lugbe, Abuja, focusing on demographic influences, family planning counselling, and contraceptive accessibility. The research aims to identify the key determinants of contraceptive uptake and the association between the contraceptive behaviour of women attending Primary Healthcare Centres in Abuja. Results will provide evidence-based recommendations for tailored interventions.
Methods: A cross-sectional study was conducted using structured questionnaires administered to postpartum women in Karonmajiji and Lugbe Primary Healthcare Centres. Data on contraceptive history, future contraceptive intentions, timing of contraceptive initiation, counselling experiences, and socio-demographic factors were collected and analyzed from consenting mothers. Descriptive statistical tests were used to compare findings between the centres, while insights were contextualized within existing global literature on postpartum contraceptive use.
Results: Findings reveal significant variations in contraceptive behaviours between the two communities. Injectable contraception was the most commonly used method in both locations (23.3% in Karonmajiji, 16.3% in Lugbe), but a large proportion of women had never used contraception (46.6% in Karonmajiji, 53.1% in Lugbe). Future contraceptive intentions were higher in Karonmajiji (57.9%) compared to Lugbe (42.3%), where resistance to contraception was more pronounced. Family planning counselling played a crucial role, with 57.1% of Karonmajiji respondents engaging in discussions with healthcare providers, compared to only 30.4% in Lugbe. Factors such as marital structure (higher polygamy in Karonmajiji), education, employment, ethnicity, and religious beliefs influenced contraceptive adoption. Key barriers included fear of side effects, lack of partner support, misinformation, and economic constraints.
Conclusion: The study highlights gaps in postpartum contraceptive uptake and the need for enhanced family planning interventions in both communities, particularly in Lugbe, where contraceptive use remains lower. Community-based counselling, improved contraceptive accessibility, and culturally sensitive engagement strategies are essential to increasing uptake. Strengthening healthcare services and leveraging digital health solutions can further bridge knowledge gaps and improve maternal health outcomes in Nigeria.
Keywords: postpartum contraceptive use; family planning; reproductive health; birth spacing; maternal health
Introduction
Contraceptive behaviour among postnatal mothers is a critical aspect of maternal and child health, influencing birth spacing, family planning, and overall reproductive well-being (Robinet, Jeffredo, & Clesse, 2023). Understanding the demographic, reproductive history, and family planning counselling patterns among postnatal mothers gives a pointer to improving contraceptive uptake and addressing existing barriers (Makins, 2022; Thapa et al., 2019). This study explores the contraceptive behaviour of postnatal mothers in Karonmajiji and Lugbe, Abuja, comparing the demographic influences, reproductive histories, and family planning counselling experiences that shape contraceptive decisions Given the high unmet need for postpartum family planning, targeted interventions must be developed to ensure effective contraception access and utilisation (Cherie, Wordofa, & Debelew, 2024; Zhuang, Li, & Li, 2019). The postpartum period represents a crucial window for family planning interventions, allowing women to prevent unintended pregnancies and achieve optimal birth spacing (Cooper 2020; Liljeblad, 2023). In Nigeria, postpartum contraceptive prevalence remains low, despite the availability of multiple contraceptive options and family planning programs (Anyatonwu et al., 2023). Studies have shown that maternal age, marital status, education level, and knowledge of contraception significantly impact postpartum contraceptive use (Adeoye et al., 2024). The Transtheoretical Model (TTM) has been widely used to assess health behaviours, including contraceptive uptake among postnatal mothers (Ansari-Majd, et al., 2021; Jalambadani, 2022). The model suggests that contraceptive behaviour is shaped by individual choice and follows through a stage of change from pre-contemplation, contemplation and action with its maintenance fuelled by health-promoting and educational activities. Self-efficacy and decisional balance factors support positive or negative behaviours. Perceptions of susceptibility to unintended pregnancy powers PROS of contraception, and downplays CONS or barriers to use (Bell et al., 2020). Additionally, the influence of sociocultural factors such as religious beliefs, partner involvement, and familial pressures plays a crucial role in shaping contraceptive decisions (Silva et al., 2022).
Empirical Review
Demographic Factors Influencing Contraceptive Behaviour
Demographic factors such as age, marital status, education level, and employment status significantly influence contraceptive decisions among postnatal mothers. Evidence of investigations shows postnatal mothers exhibited low decision-making autonomy regarding contraception, with husbands and mothers-in-law playing dominant roles in determining contraceptive use (Bhan et al., 2022; Yusuf 2021). Similarly, maternal age is a critical determinant, as older women are more likely to adopt long-acting reversible contraceptives (LARC) compared to younger mothers (Mutea et al., 2022; Jalang’o et al., 2017). Education level is another determinant of contraceptive use, as women with higher education are more likely to understand and adopt contraceptive methods (Mutea et al., 2022; Rusibamayila et al., 2017). Research in Nigeria found that women with tertiary education were significantly more likely to use modern contraceptives than those with lower educational attainment (Olayiwola et al., 2021; Dev et al., 2019). Furthermore, employment status influences contraceptive choices, with employed women exhibiting higher contraceptive prevalence due to financial independence and exposure to health information (Law, Tan, & Tong, 2019; Mutea et al., 2022).
Reproductive History and Contraceptive Uptake
A woman’s reproductive history, including the number of pregnancies, birth spacing, and history of miscarriage, significantly impacts her contraceptive behaviour (Coombe et al., 2020). Women with previous unintended pregnancies and miscarriages should be more likely to use contraceptives postpartum (Jaafar, S. K. (2022). James, Toombs, & Brodribb, 2018). Additionally, the resumption of menstruation is a key factor influencing contraceptive uptake, as women often perceive themselves at a lower risk of pregnancy before their menstrual cycle resumes (Nakiwunga, et al., 2022). Postpartum women with prior antenatal care visits demonstrated higher contraceptive uptake, indicating that healthcare exposure plays a pivotal role in reproductive decision-making (Mutea et al., 2022). Furthermore, the duration since the last childbirth affects contraceptive decisions, with women in the early postpartum period exhibiting lower contraceptive use due to breastfeeding and perceived infertility (Cherie et al., 2024).
Family Planning Counseling and Contraceptive Decision-Making
Access to quality family planning counselling significantly enhances postpartum contraceptive use (Robinet, Jeffredo, & Clesse, 2023). Studies have demonstrated that healthcare provider engagement and structured contraceptive counselling during antenatal and postnatal visits improve contraceptive adoption (Thapa et al., 2019). However, gaps in counselling services, particularly in rural settings, limit contraceptive utilization (Cherie, Wordofa, & Debelew, 2024; Ene, & Ajibo, 2023). The role of healthcare providers in promoting contraceptive use cannot be overstated. Postpartum women who received counselling from trained health personnel exhibited higher contraceptive adherence than those who did not (Atukunda, et al., 2022; Puri et al., 2020). Similarly, research in Nigeria found that women who discussed contraception with healthcare providers were significantly more likely to use postpartum contraceptives. Cultural and religious beliefs also influence the effectiveness of family planning counselling. Misconceptions about contraceptive side effects and myths surrounding modern contraceptive methods hindered effective counselling interventions. Furthermore, spousal support and partner involvement in family planning discussions are crucial for successful contraceptive adoption (Adeoye et al., 2024; Anyatonwu et al., 2023; Silva et al., 2022). Empirically, education, employment status, reproductive history, and access to quality counselling significantly impact contraceptive uptake. Further suggesting that addressing sociocultural barriers and enhancing healthcare engagement through structured counselling programs can improve postpartum contraceptive use and reduce unintended pregnancies. This study aims to contribute to the existing body of knowledge by comparing contraceptive behaviour among postnatal mothers in Karonmajiji and Lugbe, Abuja. By analysing demographic influences, reproductive histories, and family planning counselling experiences, this research seeks to provide insights into tailored interventions that promote effective contraception and reproductive health management in Nigeria.
Methodology
The methodology for this study employs descriptive statistical methods to analyse data collected on the contraceptive behaviour of postnatal mothers attending Primary Healthcare Centres (PHCs) in Karonmajiji and Lugbe, Abuja. Descriptive statistics were used to summarise demographic characteristics and contraceptive behaviours, including frequency distributions, percentages, and mean scores. Bar charts, pie charts, and histograms are utilized to visually present trends and patterns. All statistical analyses are conducted using SPSS (Version 27.0) to ensure accurate computation and interpretation of results. The study received ethical approval from UNICAF University Research and Ethics Committee. Approval for data collection was obtained from the Federal Capital Territory (FCT) Health Research Ethics Committee and the Abuja Municipal Area Council Health Department.
Results and Discussion
Respondents Demographic Analysis
The demographic findings align with existing literature on contraceptive behaviour, particularly regarding age, marital structure, education, employment, ethnicity, and religion. The majority of respondents in both locations fall within the reproductive age group of 20-39 years, accounting for 89.5% in Karonmajiji and 89.3% in Lugbe. This demographic pattern is crucial, as women within this age range are at the highest risk of unintended pregnancies and are the primary target for postpartum contraception. Studies such as Cherie et al. (2024) and Dev et al. (2019) highlight those younger women, often experience a higher unmet need for contraception, emphasising the importance of targeted interventions. The lower percentage of respondents under 20 years old in both communities suggests that adolescent postpartum contraceptive needs may be underrepresented, despite the critical role that early contraceptive education plays in preventing rapid repeat pregnancies. Marital structure further influences contraceptive use, with Karonmajiji exhibiting a higher prevalence of polygamous marriages (22.6%) compared to Lugbe (8.6%). The literature suggests that polygamous relationships often create complexities in family planning decisions, particularly where male partners or extended family members, such as mothers-in-law, exert significant influence over reproductive choices and decision-making thus limiting women’s autonomy. Jalang’o et al. 2017; and Obare et al., 2021; Mukanga et al., 2023). Similarly, Thapa et al. (2019) highlighted how subjective norms, including spousal and familial influence, impact contraceptive behaviours. This suggests that in Karonmajiji, where polygamous unions are more common, family planning interventions should incorporate strategies that engage male partners and extended family members to ensure broader acceptance and uptake of contraceptive methods. Education levels in both communities also shape contraceptive decisions, with tertiary education similarly prevalent in Karonmajiji (43.6%) and Lugbe (44.8%). However, Lugbe has a significantly higher percentage of respondents with vocational training (40.2%) unlike Karonmajiji (24.8%). The literature underscores that higher educational attainment is associated with increased contraceptive knowledge and usage. Adeoye et al. (2024) and Anyatonwu et al. (2023) found that education enhances awareness and reproductive health, facilitating better contraceptive decision-making. However, education alone may not be sufficient. This suggests that in both Karonmajiji and Lugbe, educational programs must be accompanied by effective family planning counselling to ensure women understand the proper use of contraceptive methods.
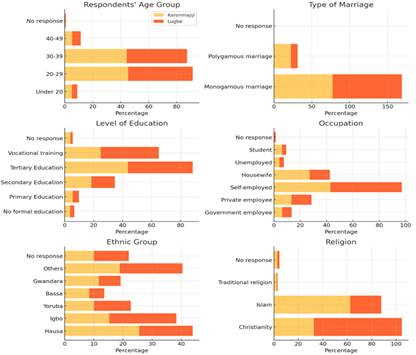
Figure 1: Bar Charts showing the demographic characteristics of the Karonmajiji and Lugbe participants
Employment status further influences postpartum contraceptive behaviour, with self-employment being the dominant occupation in both communities 42.9% in Karonmajiji and 54.3% in Lugbe. However, a larger proportion of respondents in Karonmajiji are housewives (27.1%) compared to Lugbe (15.3%). Economic independence plays a crucial role in contraceptive decision-making, as seen in Cherie et al. (2024) and Anyatonwu et al. (2023), who found that employed women are more likely to use contraception due to greater autonomy and financial capacity to access family planning services. Conversely, financially dependent women, such as housewives, often face greater barriers to accessing contraception (Coombe et al., 2020; James et al. 2018). The higher percentage of housewives in Karonmajiji suggests that financial constraints may be a more significant barrier to contraceptive uptake in this community, highlighting the need for subsidized or free contraceptive services. Cultural and ethnic factors also play a role in contraceptive practices. Karonmajiji has a higher Hausa representation (25.6%), while Lugbe has a higher Igbo population (23.0%). Ethnic variations in contraceptive acceptance have been widely documented. cultural norms significantly shape contraceptive decisions, these beliefs influence both pregnancy intentions and contraceptive behaviours. Thus, requiring tailored interventions (Coombe et al. 2020; Rusibamayila et al. 2017). Given the ethnic diversity in both Karonmajiji and Lugbe, family planning programs must be culturally sensitive and address specific concerns related to reproductive health within different ethnic groups. Religious beliefs further influence contraceptive choices, with Islam being the predominant religion in Karonmajiji (62.4%) and Christianity being dominant in Lugbe (72.1%). Religious perspectives on contraception vary widely, affecting attitudes toward family planning. reported that fear of contraceptive side effects and religious objections were significant barriers to uptake. Given these differences, contraceptive counselling efforts in Karonmajiji and Lugbe must consider religious perspectives, potentially collaborating with religious leaders to promote family planning within acceptable faith-based frameworks (Geda et al., 2021; Hakizimana & Odjidja, 2021; Okafor et al., 2022).
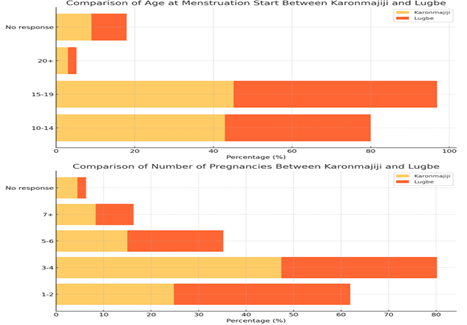
Figure 2: Respondents' Reproductive History
The onset of menstruation among respondents in both Karonmajiji and Lugbe aligns with broader findings on reproductive health, where menarche typically occurs between the ages of 10 and 19. In Karonmajiji, 42.9% of respondents reported each. Additionally, 9.0% of respondents in Karonmajiji and 8.9% in Lugbe did not experience menarche between ages 10 and 14, while 45.1% started menstruating between ages 15-19. Similarly, in Lugbe, 37.1% experienced menarche between ages 10-14, and 51.8 percentage between the ages 15-19. The literature suggests that early menarche can influence reproductive behaviour, including the timing of first pregnancies and contraceptive use (MaeregayehuTibo et al., 2021). Studies on postpartum contraceptive use indicate that age at menarche may have long-term implications for reproductive health and decision-making about family planning, as younger menarche is often associated with earlier childbearing and an increased need for contraception, reinforcing the need for targeted reproductive health education (Abera et al., 2015). The number of pregnancies reported in Karonmajiji and Lugbe reveals variations in reproductive behaviour between the two locations, with most women experiencing 1-4 pregnancies. In Karonmajiji, 24.8% of respondents reported having 1-2 pregnancies, while 47.4% had 3-4 pregnancies. Comparatively, in Lugbe, 37.1% had 1-2 pregnancies, and 32.8% had 3-4 pregnancies. Additionally, 15.0% of respondents in Karonmajiji and 20.2% in Lugbe reported having had 5-6 pregnancies, while 8.3% in Karonmajiji and 8.0% in Lugbe had experienced 7 or more pregnancies. A small percentage did not report their pregnancy history (4.5% in Karonmajiji and 1.8% in Lugbe). These findings align with studies highlighting the influence of fertility preferences, contraceptive access, and social norms on reproductive outcomes (Jalang’o et al., 2017). The higher percentage of respondents in Lugbe with fewer pregnancies compared to Karonmajiji suggests possible differences in contraceptive uptake and spacing behaviour. The presence of women with five or more pregnancies in both locations reflects patterns observed in studies on contraceptive non-use or discontinuation, where family planning needs and sociocultural influences contribute to high fertility rates (Dev et al., 2019; Mukanga et al., 2023).
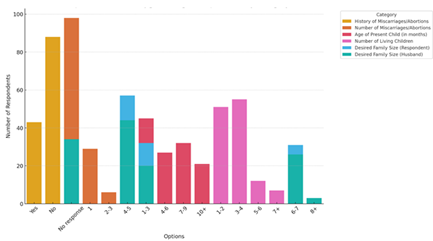
Figure 3: Karonmajiji and Lugbe respondents by reproductive categories
The prevalence of miscarriages and abortions among postpartum women has been a subject of interest in reproductive health research, particularly in understanding its implications for family planning decisions and contraceptive use. The present study indicates that the proportion of women who have experienced a miscarriage or abortion is comparable between Karonmajiji (32.3%) and Lugbe (31.3%). These findings highlight the importance of access to contraception and reproductive healthcare in preventing unintended pregnancies and reducing pregnancy-related complications. Despite the similar prevalence rates, a significant majority of respondents in both locations reported no history of miscarriage or abortion, reflecting an overall trend where access to healthcare services and maternal care may play a role in reducing pregnancy-related risks Dev et al., 2019). The number of reported miscarriages or abortions further highlights variations in reproductive experiences, with 21.8% of respondents in Karonmajiji and 17.8% in Lugbe having experienced a single event. However, multiple miscarriages (2-3) were more frequently reported in Lugbe (11.1%) than in Karonmajiji (4.5%), with a small percentage in Lugbe (3.3%) reporting four or more miscarriages. Notably, a substantial proportion of respondents did not provide an answer (73.7% in Karonmajiji and 67.8% in Lugbe), which may suggest the presence of stigma, cultural sensitivities, or a lack of awareness regarding miscarriages as a reproductive health issue. Similar findings in research by Coombe et al. (2020) and Sharma et al. (2015) suggest that sociocultural factors, including religious beliefs and community attitudes, often shape women's willingness to disclose reproductive health issues, including miscarriage experiences.
The distribution of the present child's age across the two locations suggests that most postpartum women have infants under six months old, with 33.8% in Karonmajiji and 46.7% in Lugbe reporting a child aged 1-3 months. This corresponds with global trends indicating that contraceptive adoption often begins during this window as women recover from childbirth and assess their future fertility intentions. The data also show a declining proportion of women with children aged 10 months or older, which may reflect recent childbirth patterns and access to antenatal care services that facilitate birth spacing education (Cherie et al., 2024). In terms of the number of living children, most women in both locations reported having between one and four children, a finding consistent with studies highlighting a shift towards smaller family sizes as access to contraceptive methods improves (Adeoye et al., 2024). Specifically, 38.3% of respondents in Karonmajiji and 53.0% in Lugbe reported having 1-2 children, while 41.4% in Karonmajiji and 32.5% in Lugbe had 3-4 children. The preference for smaller family sizes aligns with literature suggesting that education, economic factors, and healthcare access contribute to shifts in reproductive goals (Anyatonwu et al., 2023; Rusibamayila et al., 2017). The preference for a desired family size among respondents and their husbands further supports this trend. In both locations, the majority of women preferred having 4-5 children (42.9% in Karonmajiji and 46.3% in Lugbe), while a smaller proportion desired 1-3 children (24.0% in Karonmajiji and 37.4% in Lugbe). Husbands’ preferences for larger families appear more pronounced, with 33.1% in Karonmajiji and 39.4% in Lugbe favouring 4-5 children and some expressing interest in six or more children. These findings are in line with studies indicating that spousal influence remains a strong determinant of contraceptive uptake, as women’s reproductive choices are often mediated by their partners’ preferences and cultural expectations (Bell et al., 2020; Shahabuddin et al., 2016).
Comparative analysis between Karonmajiji and Lugbe respondents
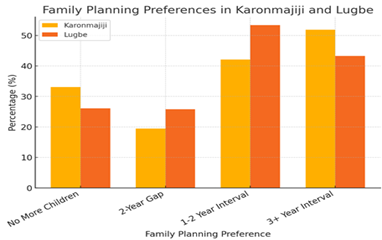
Figure 4: Showing comparative analysis of child spacing Preferences in Karonmajiji and Lugbe participants
As presented in the charts above, the timing of the next child and the spacing between pregnancies are crucial aspects of family planning, reflecting broader patterns of postpartum contraceptive use and reproductive decision-making. In Karonmajiji, 33.1% of respondents preferred not to have additional children, compared to 26.1% in Lugbe, indicating a significant interest in family size limitation. Among those planning for another child, the most common preference was a two-year gap, with 25.8% in Lugbe and 19.5% in Karonmajiji opting for this interval. However, in Lugbe, the majority (53.4%) reported pregnancy intervals of 1-2 years, while in Karonmajiji, 42.1% preferred a longer spacing of three years or more, suggesting a potential trend toward extended birth intervals. These findings align with studies such as Abera et al. (2015) and Dev et al. (2019), which highlight the strong influence of postpartum contraceptive use on birth spacing and reproductive choices. Additionally, menstrual cycle resumption post-delivery serves as an important indicator of postpartum reproductive readiness, with 51.9% of women in Karonmajiji and 43.3% in Lugbe reporting the return of menstruation. Correspondingly, 45.1% and 54.3%, respectively, had not resumed their cycles, reinforcing the link between physiological recovery and contraceptive decisions to (Naigino et al., 2021).
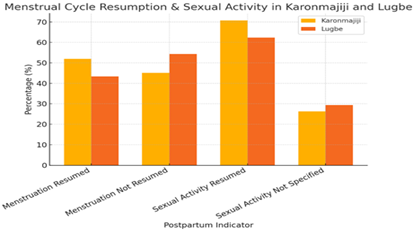
Figure 5: Comparison of Reproductive activity among participants
Resumption of sexual activity post-delivery further influences postpartum family planning needs, with 70.7% of respondents in Karonmajiji and 62.3% in Lugbe engaging in sexual intercourse after childbirth. The period of resumption varied, with 21.8% in Karonmajiji and 31.6% in Lugbe resuming within two months, while others delayed up to six months or more. Notably, a significant portion (26.3% in Karonmajiji and 29.4% in Lugbe) did not specify their timing. These statistics are consistent with findings from Sok et al. (2016) and Zhuang et al. (2019), which indicate that early postpartum sexual activity, often without consistent contraceptive use, increases the risk of closely spaced pregnancies. Furthermore, Silva et al. (2022) and Booth et al. (2018) emphasise that effective postpartum contraceptive counselling should be initiated early and reinforced postnatally to prevent unintended pregnancies and promote optimal birth spacing. The relatively early resumption of sexual activity observed in both Karonmajiji and Lugbe reinforces the necessity for immediate postpartum contraceptive interventions. There is a need for more advocacy for targeted family planning programs that address regional variations in contraceptive use, accessibility, and cultural perceptions to ensure healthier birth intervals.
Section C: Comparative Analysis of Contraceptive Behaviour Among Postnatal Mothers in Karonmajiji and Lugbe, Abuja
Contraceptive History and Usage Patterns
The study reveals differences in the contraceptive history of respondents in Karonmajiji and Lugbe, which aligns with the study’s objective of analysing demographic influences on contraceptive behaviour. A slightly higher proportion of women in Lugbe (53.1%) reported no history of contraceptive use compared to Karonmajiji (46.6%). However, 48.9% of respondents in Karonmajiji and 42.9% in Lugbe had previously used contraceptives, indicating some level of acceptance in both locations. Injectable contraception was the most commonly used method in both communities, with 23.3% of respondents in Karonmajiji and 16.3% in Lugbe reporting usage. Condom use was also notable, with 9.8% in Karonmajiji and 13.2% in Lugbe indicating prior use, alongside lower but relevant figures for implants and oral contraceptives. Indicating similar trends in the literature (Abate & Obsie, 2021; Assefa & Koboto, 2021; Seifu et al., 2020). However, a significant proportion of women in both locations (16.5% in Karonmajiji and 22.4% in Lugbe) expressed no intention to use contraception, which suggests potential cultural or informational barriers requiring targeted interventions.
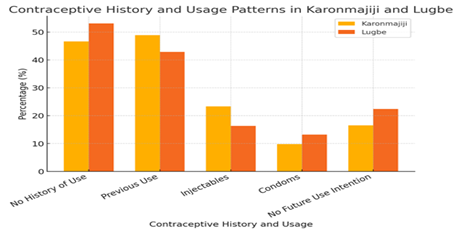
Figure 6: Comparison of contraceptive practice and usage
Future Contraceptive Use Intentions
The study highlights key variations in future contraceptive use intentions, which can guide interventions promoting effective contraception. In Karonmajiji, 57.9% of respondents expressed an intention to use contraceptives, compared to only 42.3% in Lugbe. Conversely, 49.4% of respondents in Lugbe reported no intention to use contraceptives in the future, compared to 34.6% in Karonmajiji. This difference suggests that family planning counselling may have a stronger influence on contraceptive decision-making in Karonmajiji than in Lugbe. This nuanced finding is an eye-opener to a ready population needing focused counselling right at the city (Chace Dwyer et al., 2022). Additionally, uncertainty regarding the timing of contraceptive initiation post-delivery was higher in Lugbe (41.4%) than in Karonmajiji (30.8%), further reinforcing the need for postpartum family planning education in Lugbe.
Current Contraceptive Use and Maintenance
When assessing current contraceptive use, a majority of women in both locations reported not using any form of contraception (72.9% in Karonmajiji and 72.7% in Lugbe), emphasising gaps in sustained family planning. Among those currently using contraceptives, 17.3% of Karonmajiji respondents had been using their method for 6-12 weeks, compared to 12.3% in Lugbe. However, high non-response rates regarding the duration of contraceptive use (65.4% in Karonmajiji and 76.7% in Lugbe) suggest possible inconsistencies in contraceptive maintenance or incomplete reporting. Additionally, while 57.1% of respondents in Karonmajiji practised family planning between pregnancies, only 39.6% in Lugbe did the same, indicating a need for stronger family planning interventions in Lugbe.
Influence of Family Planning Counselling
Family planning counselling plays a significant role in shaping contraceptive behaviours, with notable differences between Karonmajiji and Lugbe. In Karonmajiji, 57.1% of respondents reported discussing contraception with a healthcare provider, compared to only 30.4% in Lugbe. Similarly, 55.6% of Karonmajiji respondents received family planning counselling from a nurse or midwife, while 49.7% of Lugbe respondents had not received any counselling at all. The disparities in access to contraceptive information are further reflected in the sources of contraceptive knowledge, with 51.9% of respondents in Karonmajiji receiving information from healthcare providers, compared to only 31.6% in Lugbe. Instead, a larger proportion of women in Lugbe (36.2%) relied on friends and family. Just like participants in Okoeguale et al., (2022), this population are at increased risk of misinformation and hesitancy toward contraceptive use. Meanwhile, literature is awash with evidence of counselling benefits (Borovac-Pinheiro et al., 2019; Nurjanah et al., 2022; Palinggi et al., 2021; Reyes-Lacalle et al., 2020; Solomon et al., 2020). What is left is to take full advantage of it.
Perceptions of Contraceptive Benefits
The study findings indicate that perceptions of contraception's benefits, such as preventing unwanted pregnancies and supporting family size limitation, are generally positive in both locations. In Karonmajiji, 56.4% of respondents strongly agreed that contraception helps prevent unwanted pregnancies, while 45.1% of Lugbe respondents held the same view. However, scepticism about contraceptives was slightly higher in Lugbe, where 12.6% of respondents strongly disagreed with this notion, compared to 7.5% in Karonmajiji. Similarly, the perception that contraception allows for worry-free pregnancy was higher in Karonmajiji (54.9% strongly agreeing) compared to Lugbe (41.1% strongly agreeing), suggesting that respondents in Karonmajiji may feel more secure in the reliability of contraceptives for family planning.
Concerns About Contraceptive Use
Despite generally favourable perceptions of contraception, concerns about contraceptive side effects are prominent in both locations. In Karonmajiji, 45.1% of respondents expressed concerns about side effects, while 49.7% in Lugbe shared the same worry. These findings highlight side effects as a critical barrier to contraceptive uptake, reinforcing the need for counselling interventions that address misconceptions and provide reassurance about the safety of contraceptives. Additionally, social influences play a significant role in shaping contraceptive decisions, with 37.6% of respondents in Karonmajiji and 34.7% in Lugbe strongly agreeing that the experiences of friends and neighbours with side effects influence their own contraceptive choices. This underscores the need for community-based education initiatives to counteract misinformation and promote positive contraceptive experiences.
Impact of Cultural and Economic Factors
Cultural and economic perceptions influence contraceptive behaviour in both locations. While 52.6% of Karonmajiji respondents strongly disagreed with beliefs against contraception, a slightly lower proportion (48.8%) in Lugbe held the same view. However, 18.1% of respondents in Lugbe strongly agreed with anti-contraceptive beliefs, compared to 10.5% in Karonmajiji, indicating a greater cultural hesitancy toward contraceptive use in Lugbe. Additionally, economic considerations play a role in contraceptive decision-making. While 49.6% of respondents in Karonmajiji strongly disagreed that contraception is more expensive than pregnancy, 12% in Lugbe strongly agreed with this notion, indicating a potential financial barrier to contraceptive adoption. This suggests the need for targeted interventions that highlight the long-term economic benefits of contraception in Lugbe.
Conclusion
This study explores key demographic, socio-cultural, and economic factors influencing postpartum contraceptive behaviour in Karonmajiji and Lugbe, Abuja. While contraceptive awareness exists, uptake remains inconsistent, with higher reluctance in Lugbe (49.4% do not intend to use contraception) compared to Karonmajiji (34.6%). Injectable contraceptives are the most preferred method, but concerns over side effects, religious beliefs, and misinformation hinder broader adoption. Family planning counselling is more accessible in Karonmajiji (57.1%) than Lugbe (30.4%), where reliance on friends and family for contraceptive information increases the risk of misconceptions.
Summary of Findings
Findings reveal low contraceptive use in Lugbe (53.1% have never used contraception) compared to Karonmajiji (46.6%). The majority of women (72.9% in Karonmajiji, 72.7% in Lugbe) are not using contraception postpartum, increasing the risk of closely spaced pregnancies. Economic barriers affect contraceptive uptake, with 12% in Lugbe perceiving contraception as costly. Cultural and religious beliefs strongly influence decisions, with Lugbe exhibiting greater scepticism toward contraception (18.1% strongly agree with anti-contraceptive beliefs). Women in Karonmajiji (57.9%) are more likely to seek future contraception than those in Lugbe (42.3%), emphasizing the need for targeted interventions.
Recommendations
Expand counselling services in Lugbe, where 49.7% of women received no counselling, and integrate family planning discussions into antenatal, postnatal, and immunization visits. Engage husbands, elder family members, and religious leaders to promote contraception within culturally acceptable frameworks, reducing resistance to contraceptive use. Ensure continuous contraceptive supply, subsidize costs for economically disadvantaged women, and increase distribution through Primary Healthcare centres and pharmacies. Promote Long-Acting Reversible Contraceptives (LARCs) such as implants and IUDs to reduce discontinuation rates and encourage consistent contraceptive use. Extend contraceptive education of pharmacist as they are a veritable source for Lugbe residents. Launch peer education programs to address misinformation and encourage contraceptive uptake. Utilize mobile health (mHealth) platforms for contraceptive reminders and follow-ups, ensuring that postpartum women receive ongoing support for reproductive health decisions.
References
- Timmermans A, Opmeer BC, Khan KS, Bachmann LM, Epstein E, Clark TJ, et al. (2010). Endometrial thickness measurement for detecting endometrial cancer in women with postmenopausal bleeding: A systematic review and meta- analysis. Obstet Gynecol, 116(1):160-167.
Publisher | Google Scholor - Loiacono RMR, Trojano G, Del Gaudio N, Kardhashi A, Deliso MA, Falco G, et al. (2015). Hysteroscopy as a valid tool for endometrial pathology in patients with postmenopausal bleeding or asymptomatic patients with a thickened endometrium: Hysteroscopic and histological results. Gynecol Obstet Invest, 79(3):210-216.
Publisher | Google Scholor - Vitale SG, Haimovich S, Laganà AS, Alonso L, Di Spiezio Sardo A, Carugno J. (2021). Endometrial polyps: An evidence-based diagnosis and management guide. Eur J Obstet Gynecol Reprod Biol, 260:70-77.
Publisher | Google Scholor - Nappi L, Indraccolo U, Di Spiezio Sardo A, et al. (2009). Are diabetes, hypertension, and obesity independent risk factors for endometrial polyps? J Minim Invasive Gynecol, 16(2):157-162.
Publisher | Google Scholor - Hase S, Mitsumori A, Inai R, Takemoto M, Matsubara S, Akamatsu N, et al. (2012). Endometrial polyps: MR imaging features. Acta Med Okayama, 66(6):475-485.
Publisher | Google Scholor - Bakour SH, Gupta JK, Khan KS. (2002). Risk factors associated with endometrial polyps in abnormal uterine bleeding. Int J Gynaecol Obstet, 76(2):165-168.
Publisher | Google Scholor - Ghoubara A, Sundar S, Ewies AAA. (2018). Predictors of malignancy in endometrial polyps: study of 421 women with postmenopausal bleeding. Climacteric, 21(1):82-87.
Publisher | Google Scholor - Gimpelson RJ, Rappold HO. (1988). A comparative study between panoramic hysteroscopy with directed biopsies and dilatation and curettage. A review of 276 cases. Am J Obstet Gynecol,158(3Pt1):489-492.
Publisher | Google Scholor - Ceci O, Franchini M, Cannone R, Giarre G, Bettocchi S, Fascilla FD, et al. (20190. Office treatment of large endometrial polyps using truclear 5C: feasibility and acceptability. J Obstet Gynaecol Res, 45(3):626-633.
Publisher | Google Scholor - Namazov A, Gemer O, Ben-Arie A, Israeli O, Bart O, Saphier O, et al. (2019). Endometrial polyp size and the risk of malignancy in asymptomatic postmenopausal women. J Obstet Gynaecol Can, 41(7):912-915.
Publisher | Google Scholor - Lee SC, Kaunitz AM, Sanchez-Ramos L, Rhatigan RM. (2010). The oncogenic potential of endometrial polyps: a systematic review and meta-analysis. Obstet Gynecol, 116(5):1197-1205.
Publisher | Google Scholor - Shor S, Pansky M, Maymon R, Vaknin Z, Smorgick N. (2019). Prediction of premalignant and malignant endometrial polyps by clinical and hysteroscopic features. J Minim Invasive Gynecol, 26(7):1311-1315.
Publisher | Google Scholor - Elfayomy AK, Soliman BS. (2015). Risk factors associated with the malignant changes of symptomatic and asymptomatic endometrial polyps in premenopausal women. J Obstet Gynaecol India, 65(3):186-192.
Publisher | Google Scholor - Ngo YG, Fu HC, Chu LC, Tseng CW, Chen CY, Lee CY, Ou YC. (2020). Specific hysteroscopic findings can efficiently distinguish the differences between malignant and benign endometrial polyps. Taiwan J Obstet Gynecol, 59(1):85-90.
Publisher | Google Scholor - Elyashiv O, Sagiv R, Kerner R, Keidar R, Menczer J, Levy T. (2017). Hysteroscopic resection of premalignant and malignant endometrial polyps: Is it a safe alternative to hysterectomy? J Minim Invasive Gynecol, 24(6):977-982.
Publisher | Google Scholor - Ferrazzi E, Zupi E, Leone FP, Savelli L, Omodei U, Moscarini M, et al. (2009). How often are endometrial polyps malignant in asymptomatic postmenopausal women? A multicenter study. Am J Obstet Gynecol, 200(3):235.e1-235.e6.
Publisher | Google Scholor























